
Abstract
Both psychological distress and fatigue are common post stroke. Although there is recognition that the phenomena are related, the nature of the relationship is unclear.Cross-sectional study of 98 independently functioning participants within 2 years of stroke. Significant relationships were observed between fatigue and general anxiety, health-related anxiety and stroke-specific anxiety (r range from .31 to .37). In the final regression model, depression, pain and stroke-specific anxiety were significant, accounting for 32 per cent of the variance in fatigue scores (p < .001). The findings provide insight into the importance of anxiety-related factors post stroke, their relevance to our understanding of post-stroke fatigue and their implications for post-stroke intervention.
Introduction
Fatigue is one of the most frequently reported symptoms post stroke with reported prevalence rates ranging from 30 to 70 per cent (De Groot et al., 2003; Ingles et al., 1999; Lerdal et al., 2011; Schepers et al., 2006). Fatigue has been defined as an ‘overwhelming sense of tiredness, exhaustion, lack of energy, or difficulties sustaining routine actions’ (Naess et al., 2005: 245). Our current understanding and assessment of fatigue encompasses two dimensions, psychological fatigue (fatigue during a cognitive process) and physiological fatigue (fatigue during a physical process) (Choi-Kwon and Kim, 2011; Zwarts et al., 2008). Fatigue is frequently described as one of the most difficult symptoms to cope with following stroke (Lerdal et al., 2011; Zwarts et al., 2008) and has negative implications in terms of rehabilitation and the patient’s family, social and occupational life (De Groot et al., 2003; Radman et al., 2012). The onset and maintenance of fatigue is likely to involve a dynamic interaction of biological, psychosocial and behavioural phenomena; however, little is known about the exact nature of the relationships between these phenomena (Choi-Kwon and Kim, 2011; Ingles et al., 1999).
Psychological distress is a broad conceptual term that refers to symptoms of depression, anxiety and negative affect (De Weerd et al., 2011; Quale and Schanke, 2010). Existing research has focused primarily on depression and its relationship with post-stroke fatigue (PSF) with several studies demonstrating a strong relationship between the two phenomena (Naess et al., 2005; Schepers et al., 2006; Snaphaan et al., 2011). However, the role of anxiety in PSF has been less well studied. This is despite the fact that anxiety (23%) is reported to be as prevalent as depression (19%) in the initial aftermath of stroke (Bergersen et al., 2010; De Wit et al., 2008; Sagen et al., 2009) and may be more likely to persist over time (Morrison et al., 2005).
The aim of this study was to examine the association of PSF with different aspects of psychological distress, including depression and specific types of anxiety. The relationship between PSF and related conditions such as pain and sleep disruption was also explored.
Methods
Participants were recruited to the study from the neurovascular clinic and rehabilitation day hospital of a university teaching hospital and from a local stroke support group. Inclusion criteria included people aged over 18 years who had experienced a stroke as diagnosed by a stroke consultant according to World Health Organization criteria (National Institute of Neurological Disorders and Stroke, 1990) between 1 month and 2 years of data collection. Participants who had significant cognitive impairment that would negate capacity to provide informed consent were excluded, as were people with moderate to severe communication difficulties (receptive and/or expressive) who could not participate in the interview process. Furthermore, those who had major comorbid medical difficulties or acute health difficulties other than stroke were excluded.
A cross-sectional design was used. Quantitative data were collected using a battery of psychometric measures assessing fatigue (Fatigue Assessment Scale (FAS); Michielsen et al., 2003), cognitive functioning (Montreal Cognitive Assessment (MoCA); Nasreddine et al., 2005), functional impairment (The Modified Rankin Scale (mRS); Rankin, 1957; Van Swieten et al., 1988), pain (Numeric Pain Rating Scale (NPRS); Breivik et al., 2000), sleep disturbance (single item Likert scale), generalised depression and anxiety (Hospital Anxiety and Depression Scale (HADS); Snaith and Zigmond, 1994), health anxiety (Short Health Anxiety Inventory (SHAI); Salkovskis et al., 2002) and stroke-specific anxiety (author-constructed questionnaire, see Appendix 1). The HADS was modified by removal of Item 8 (I feel as though I am slowed down) to avoid potential confounding of depression scores with the fatigue scores.
An author-constructed stroke anxiety questionnaire (see Appendix 1) was used to examine the participant’s cognitive, behavioural and emotional responses to stroke as well as the nature and perceived causes of their symptoms. Items were selected based on previous research on people’s responses to and mental representations of physical illness (Leventhal et al., 1984; Moss-Morris et al., 2002) and our previous research exploring experiences of psychological distress post stroke (Crowe et al., 2012). The measure explores participants’ symptoms of anxiety specific to their stroke experience and whether participants hold maladaptive representations of their experience that may be contributing to their distress and subsequent behavioural responses. Cronbach’s alpha for the measure was .85.
Ethical approval for the study was obtained from both Hospital and University ethics committees. An alpha level of .05 and power of .80 were used in this study. Previous studies exploring the relationship between psychological distress and PSF found a medium effect size (Schepers et al., 2006; Snaphaan et al., 2011). A priori analysis suggested that a sample size of 103 participants was required in this study to detect a medium effect size for multiple regression analyses with seven variables. Data were analysed using IBM SPSS Statistics Version 21.0. Relationships between fatigue and psychosocial, demographic and clinical variables were explored using Pearson product moment correlations (for continuous variables) and point-biserial correlations (for dichotomous variables).
Hierarchical multiple regression investigated which psychosocial and clinical factors were associated with fatigue and the relative influence of each. Only variables that correlated with a p value of .01 or less were entered into the multiple regression models. Depression and clinical factors that were significantly associated with fatigue were first entered into the model, followed by generalised anxiety, health anxiety and stroke-specific anxiety in step 2. No problems with multicollinearity were detected in the data and assumptions regarding normally distributed residuals were met.
Results
A total of 107 participants were recruited over an 11-month period. Data from three participants were deemed invalid as participants had failed to complete the entire assessment battery. In addition, there were six instances where participants’ performance on the MoCA raised concerns in relation to their capacity to consent and to respond to self-report measures in a reliable and valid manner. The final sample included in the analyses consisted of 98 participants (70 males, 28 females).
Demographic and clinical characteristics for participants are presented in Table 1. All but three participants were of White Irish ethnicity. Participants ranged in age from 32 to 94 years of age with a mean age of 65.41 years (standard deviation (SD) = 11.47 years). Mean time since stroke was 7.13 months (SD = 6.42 months) and 17 participants (17.3%) had experienced multiple strokes.
Participants’ demographic and clinical characteristics (N = 98).

Data available for 89 participants (i.e. from hospital setting only).
The prevalence of fatigue among participants was 47 per cent (male = 46%, female = 50%). The prevalence of anxiety based on participants’ HADS scores was 36.7 per cent (n = 36) while 15.3 per cent (n = 15) of participants scored above the cut-off for depression. In relation to cognitive impairment, participants’ mean MoCA score was 23.96. Although this score is lower than the cut-off score of 26 originally proposed by Nasreddine et al. (2005), it is broadly in line with mean scores observed (M = 24.13) in an Irish normative population (Kenny et al., 2013). Participants’ level of functional impairment ranged from ‘none’ to ‘moderate disability’ (i.e. requires some help but able to walk without assistance).
Participants’ level of fatigue was significantly associated with stroke location – occipital lobe (rpb = −.24, n = 89, p < .05), physical comorbidity – arthritis (rpb = .234, n = 89, p < .05), psychiatric comorbidity – depression/antidepressant medication (rpb = .225, n = 89, p < .05), functional impairment (mRS) (r = .244, n = 98, p < .05), sleep disturbance (r = .21, n = 98, p < .05) and higher levels of pain (r = .345, n = 98, p < .001). No significant associations were found between any other demographic or clinical factors and levels of fatigue (i.e. age, gender, marital status, living arrangements, employment status, educational level, stroke type, time since stroke, number of strokes and MoCA score).
Pearson correlation coefficients between fatigue and the various psychosocial variables assessed are displayed in Table 2. Significant, moderately strong correlations (r ranges from .37 to .44) were observed between fatigue and overall psychological distress, depression and general anxiety as measured by the HADS. Fatigue was also significantly associated with health anxiety (r = .31) and stroke-specific anxiety (r = .37). Significant, moderate-to-strong correlations were observed between each of the three anxiety measures as well as between each anxiety measure and depression (r ranges from .47 to .56).
Correlation between fatigue and psychosocial variables.
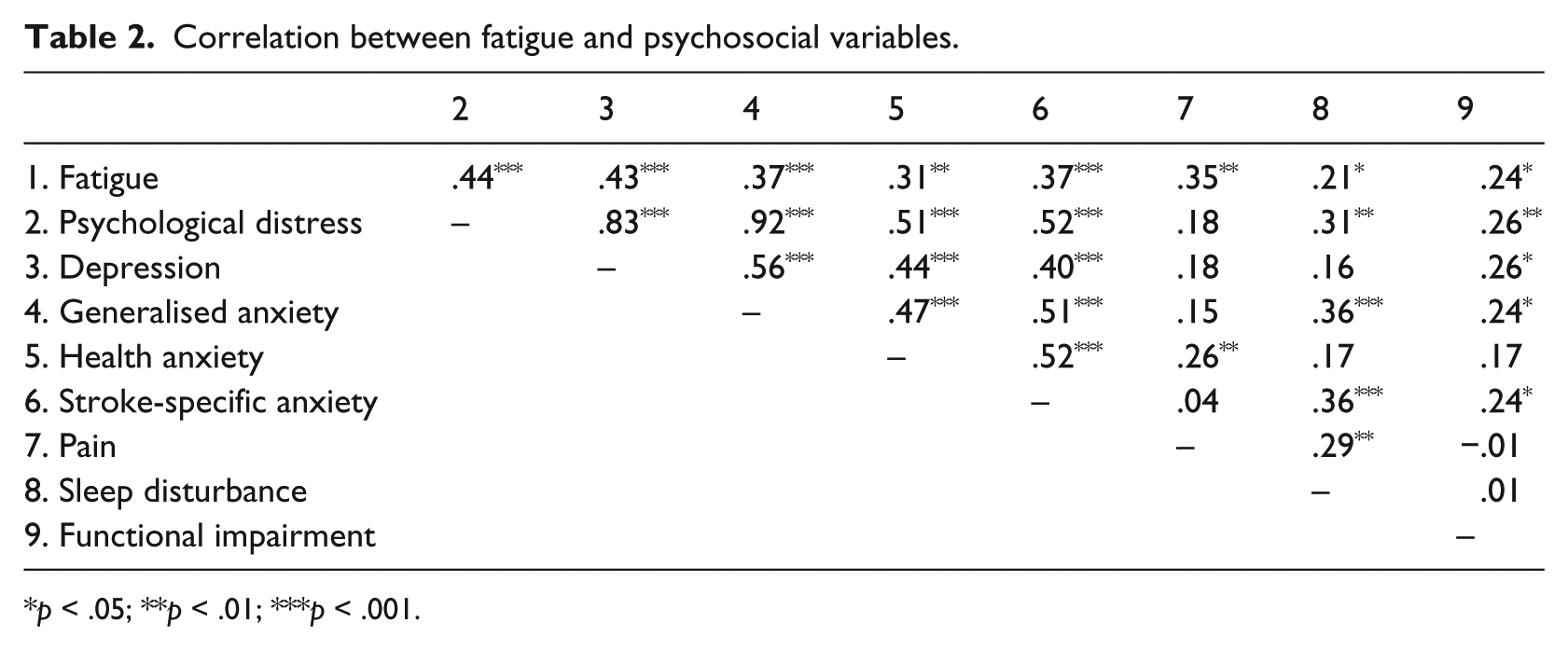
p < .05; **p < .01; ***p < .001.
A hierarchical multiple regression was conducted with fatigue as the dependent variable. Depression (Hospital Anxiety and Depression Scale–Depression (HADS-D) and pain were first entered into the model, followed by the three anxiety variables in step 2. The final regression model (see Table 3) was significant: R2 = .32, F(5, 92) = 8.48, p < .001. Depression and pain accounted for 26 per cent (Adjusted R2 = .24) of the variation in fatigue with both variables statistically significant (p < .01). The addition of general anxiety, health anxiety and stroke-specific anxiety in step 2 accounted for an additional 6 per cent of the variance in fatigue (Adjusted R2 = .28). In the final model, three of the five variables (depression, pain and stroke-specific anxiety) significantly accounted for the variance in fatigue scores (p < .05). In terms of the unique variance in fatigue accounted for by each variable, depression accounted for 4 per cent (part r2 = .041), pain for 7 per cent (part r2 = .074) and stroke-specific anxiety for 4 per cent (part r2 = .035).
Hierarchal regression model (psychological and clinical variables) for fatigue.

p < .05; **p < .01; ***p < .001.
Discussion
Psychological distress and fatigue are important issues post stroke. Furthermore, the findings help expand our understanding of psychological distress post stroke to account for the prevalence and influence of anxiety-related phenomena. This is the first study to assess the potential role anxiety-related factors may play in relation to PSF; preliminary evidence suggests a role for stroke-specific anxiety in relation to PSF. The study’s findings also support previous research highlighting the relationship between PSF and depression.
The prevalence rates of fatigue, anxiety and depression among this sample are broadly in line with previous rates reported among stroke populations (Bergersen et al., 2010; Falconer et al., 2010; Sagen et al., 2009; Schepers et al., 2006). Of note, rates of anxiety among this sample were more than double that of depression. Rates of anxiety have been found to be much higher than depression in studies of other aspects of cardiovascular disease, for example, acute coronary syndrome (Januzzi et al., 2000).
To the authors’ knowledge, this study was the first to address anxiety and its relationship to PSF specifically. Furthermore, the fact that the study explored specific types of anxiety, each with slightly different underpinning mechanisms, helped to better understand the intricate interplay between fatigue and psychological distress post stroke. Our study demonstrated a positive relationship between PSF and psychological distress. The direction and magnitude of this relationship was relatively consistent across all measures of distress used in the study. The finding that depression (based on HADS-D score) had the strongest relationship with fatigue out of all the psychological variables assessed is unsurprising and reiterates why it has been the predominant construct of interest in the literature on PSF. Given that existing research has yet to reliably determine the temporal order and reciprocal influence of the two constructs, only tentative inferences can be made at this point. However, it is possible that fatigue may initially be part of the physical sequelae of stroke, while depression may become more influential after the immediate physical effects of the illness have passed in terms of explaining the cognitive (e.g. impaired concentration) and behavioural (e.g. reduced activity) manifestations of fatigue.
The next part of the study looked at the relationship between anxiety and PSF specifically, while controlling for the influence of previously implicated variables. In line with previous findings (Lerdal et al., 2009), depression and pain significantly account for the variance in fatigue scores where the unique variance accounted for by each was 4 and 7 per cent, respectively. These findings support previous research identifying pain as one of the most important clinical variables influencing PSF (Naess et al., 2012). Pain may contribute to PSF both directly and indirectly through a number of mechanisms including cognitive (i.e. catastrophising, hypervigilance, biased attention to somatic symptoms), behavioural (i.e. reduced activity, behavioural avoidance) and neurophysiological (i.e. Hypothalamic–pituitary–adrenal axis dysregulation) mechanisms, all of which have been implicated in theoretical models of psychological distress (Deary et al., 2007; Turk, 1999). Although there have been previous reports showing the positive relationship between psychological distress and pain (Turk, 1999), this relationship was only partially supported in this study; health anxiety, but not depression or generalised anxiety were significantly associated with pain. The fact that an item on physical slowing was eliminated from the HADS (item 8) may partially explain this finding. In relation to the anxiety-related variables, general anxiety, health anxiety and stroke-specific anxiety all showed moderately strong associations with PSF. However, in the final regression model, general anxiety and health anxiety were no longer significant when the influence of depression, pain and stroke-specific anxiety were controlled for.
The relationship between stroke-specific anxiety and PSF remained significant while controlling for the influence of each of the other variables. Stroke-specific anxiety uniquely accounted for 4 per cent of the variance in fatigue scores. This suggests that stroke-specific anxiety may be of equal importance to depression in terms of understanding PSF. In addition, these findings support the argument for examining various types of distress and the constructs underlying each type of experience individually. In this instance, it would appear that in terms of understanding the relationship between fatigue and psychological distress following stroke, people’s stroke-specific concerns may be among the most significant issues to consider. The measure of stroke-specific anxiety assessed participants’ response to stroke in terms of increased negative affect, hypervigilance, interpretation of ambiguous bodily sensations, invasive images and worries about stroke, beliefs about stroke recurrence and behavioural avoidance. Subsequently, it is plausible that the development of an intervention to target these phenomena may be of benefit.
The current sample comprised individuals without significant cognitive, physical or communicative impairments. Therefore, the findings of this study may not be generalisable to the wider population of people who have experienced a stroke, many of whom experience significant impairment across these domains. Furthermore, the timeframe post stroke ranged from 1 month to 2 years in this study; it is not possible, therefore, to make inferences beyond this period as the phenomena assessed in this study and the relationships between them may change over time. The cross-sectional design of this study precludes us from drawing inferences about the temporal and causal order of the relationships between the variables assessed. The use of longitudinal studies is particularly important in order to inform our understanding of fatigue given the variability of PSF over time and the relative influence of different variables at different time points.
Participants with medical comorbidities associated with fatigue, such as thyroid conditions, depression or arthritis, were included in the study in order to reflect the demographic of stroke patients as accurately as possible. The fact that significant associations were found between fatigue and comorbid depression and arthritis makes it more difficult to differentiate the relative influence of pre-stroke, post-stroke and non-stroke factors in relation to fatigue.
Conclusion
An improved understanding of the physical sequelae of stroke has led to improved patient outcomes and quality of life. Although issues such as fatigue and psychological distress in the aftermath of stroke can be equally debilitating, our understanding of these invisible sequelae is less well developed. Our findings suggest that the application of a model encapsulating both physical and psychological factors may be helpful when conceptualising these complex phenomena and supporting the individual in managing these difficulties.
Footnotes
Appendix 1
Please read each statement carefully before answering.
Acknowledgements
The study was supported by St. James’s Hospital Dublin, The Volunteer Stroke Scheme Dublin and Trinity College Dublin. Special thanks to all participants who volunteered to take part in the study. Thank you also to Lisa Masterson, Suzanne Walsh and all the staff at the Stroke Clinic and Older Adult Day Services at St. James’s Hospital for their assistance in organising the data.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.