
Abstract
Perceiving ethnic discrimination can have aversive consequences for health. However, little is known about whether perceiving language-based (how one speaks a second language) discrimination poses the same risks. This study examined whether perceptions of language-based and ethnic discrimination are associated with mental and physical health. Among 132 Mexican and Dominican immigrant women, perceiving ethnic and language-based discrimination each predicted psychological distress and poorer physical health. When examined together, only ethnic discrimination remained a significant predictor. These results emphasize the importance of understanding how perceived ethnic and language-based discrimination play an integral role in the health of Latina immigrant women.
Navigating day-to-day life can be stressful if an individual perceives unfair, suspicious, or rude treatment from others due to discrimination. The psychological literature often focuses on only one form of discrimination at a time. However, discrimination can be perceived from multiple sources. Many ethnic minority individuals are also immigrants, and others may discriminate against them because of their ethnicity or because of the way they speak their host country’s language. Indeed, these issues may become increasingly relevant, considering that by 2050, it is projected that 19 percent of the United States will be foreign-born and 53 percent will be ethnic minorities (Pew Research Hispanic Center, 2008). Latino/as warrant particular attention as they are now the largest racial/ethnic minority in the United States and are projected to constitute about a third of the population by 2060 (US Census Bureau, 2013). In addition, about one-third of Latino/as in the United States are foreign-born and about three-quarters of them over the age of 5 years speak Spanish at home (US Census Bureau, 2013).
Studying multiple sources of perceived discrimination in Latino/as is important as perceiving discrimination can be stressful and could potentially lead to poor health. Indeed, a growing body of research has found that racial/ethnic discrimination has been associated with worse mental and physical health (Finch et al., 2001; Huynh and Fuligni, 2010). Pascoe and Smart Richman (2009) proposed that perceived discrimination leads to negative mental and physical health through three potential pathways. In the first, perceived discrimination can directly affect health. In the second, perceived discrimination can lead to a heightened physiological stress response, which, in turn, leads to poorer health. In the third, perceived discrimination can lead to more risky health behaviors (e.g. Flores, Tschann, Dimas et al., 2010; Yoshikawa, Wilson, Chae et al., 2004), which, in turn, leads to poorer health. Much empirical evidence supports parts of this model, especially pertaining to racial/ethnic discrimination. However, far less is known about the potential health consequences of perceiving language-based discrimination.
As with race/ethnicity, the way one speaks a language follows one around through every context of daily life. Language is a necessary component for interactions with others and for optimal functioning and integration into a society. In addition, language impacts how people perceive others. One’s fluency, grammar, and accent can reflect the length of time one has been in a country and one’s class, can affect whether one is perceived as a perpetual foreigner, and can dredge up group stereotypes. New research has shown that even at a young age, American children tended to discriminate against other children who spoke English with an accent (Kinzler et al., 2009). Thus, the way one speaks a language can potentially elicit discrimination experiences because of the stereotypes it evokes. Also, because language is a constant and integral part of the self that impacts interactions with others, language-based discrimination may be particularly salient to immigrants who often speak the host language differently from the native-born.
Although the problem of language-based discrimination may be widely experienced by immigrants around the world, only a handful of studies have directly examined its links with health. Perceiving language-based discrimination has been linked to seeking mental health services, reporting more chronic health conditions, and engaging in HIV risk behaviors in Asian and Pacific Islander Americans (Spencer and Chen, 2004; Yoo, Gee, and Takeuchi, 2009; Yoshikawa et al., 2004). In addition, recent research has suggested that the impact of language-based discrimination can affect new generations. Immigrant Latina mothers who perceived more language-based discrimination reported that their infants went to the doctor for illness more often (Halim, Yoshikawa, and Amodio, 2013). Overall, the research pertaining to the potential health consequences of language-based discrimination is sparse. This study aims to address this gap.
In addition to examining the link between perceived language-based discrimination and health, it is also important to examine the separate influences of ethnic and language-based discrimination, as individuals may perceive both types. Ethnic and language-based discrimination have been found to be distinct constructs in Asian and Pacific Islander Americans (Yoo et al., 2009; Yoshikawa et al., 2004). Yet few studies have looked at these two types of perceived discrimination within a single study. Instead, various types of discrimination are sometimes asked about within a single question (e.g. Todorova et al., 2010), making it difficult to understand the separate influences of each on health. Is one type of discrimination more harmful than the other? The results of one study on Asian Americans suggest that language-based discrimination might be more strongly linked to physical health compared to ethnic discrimination (Yoo et al., 2009). Yet, there is reason to believe that the type of discrimination that is more relevant to health may vary across ethnic groups. A separate study found that among Latino/as, when ethnic discrimination and English proficiency were examined together, ethnic discrimination, but not English proficiency, predicted greater psychological distress (Zhang et al., 2012). Although English proficiency is different from perceiving language-based discrimination, this study suggests that a similar relationship might exist when language-based and ethnic discrimination are compared.
There are two alternative hypotheses, which this study aims to test. On one hand, ethnic discrimination might be perceived as more stressful than language-based discrimination, and thus be more predictive of health outcomes. Individuals may view ethnicity as an inherent quality that they possess and that cannot be changed or controlled. Hence, individuals may view differential treatment based on ethnicity as inescapable and feel helpless in the face of ethnic discrimination. If ethnicity is considered an essence of the self and considered to be an internal type of characteristic, individuals may also take ethnic discrimination more personally. In contrast, individuals may view the way one speaks a language as an external characteristic that is under one’s control. If an immigrant speaks the host language with an accent or with incorrect grammar, that individual may think that further study of the language and practice can improve their language skills. With improvement, experiencing language-based discrimination may not seem as inevitable, but instead as preventable. On the other hand, language-based compared to ethnic discrimination might be perceived as more stressful, and thus be more predictive of health outcomes. For immigrant groups in particular, language is often viewed as central to one’s identity (Rogers et al., 2012). Language links one to one’s ethnic group and to one’s kin. If language is more relevant than ethnicity to one’s personal self-concept, then discrimination based on language could potentially damage one’s health more. Thus, we will test two alternative hypotheses predicting whether ethnic or language-based discrimination has a stronger influence on health.
This study has two overall research aims. The first is to test whether perceiving both ethnic and language-based discrimination are independently linked to poorer mental and physical health. This is an important issue as a review revealed that past literature has failed to examine the “distinct and cumulative impact of multiple dimensions of perceived discrimination” and that this understates the association between perceived discrimination and health (Williams et al., 2003: 203). The second is to test whether ethnic or language-based discrimination is a stronger predictor of health outcomes when examined together. We sampled Latina immigrant women for several reasons. First, despite Latino/as’ large presence, few studies have examined other ethnic minorities besides African Americans when looking at discrimination and health (Williams et al., 2003). Second, health disparities between Latino/as and non-Hispanic Whites persist in America across certain indices of health (Vega et al., 2009), for example, in the higher rates of obesity among Latina women (Miranda et al., 2008). Thus, understanding the factors that put Latino/as at risk for poorer health is important. Third, we focused on mothers in particular because of emerging research suggesting that stress and psychological distress experienced by mothers, whether due to discrimination or other factors, can also affect the health of their children (e.g. Dunkel-Schetter and Tanner, 2012). Currently, the majority of children younger than age 1 year in the nation are ethnic minorities (US Census Bureau, 2012). Thus, the physical and mental health of ethnic minority immigrant mothers may have implications for future generations.
Method
Participants and procedure
Participants included 132 Latina women (69 Dominican, 63 Mexican). Participants were recruited from the maternity wards of New York City hospitals to take part in a larger study on child development. Participants were eligible for the study if they (1) were 18+ years of age, (2) were not living in a shelter, and (3) self-identified as Mexican or Dominican. All women were mothers of 14-month-olds at the time of data collection. Trained research assistants from primarily White and Latina backgrounds interviewed participants at their homes in the participant’s preferred language (70% Spanish, 30% English). Interviewer ethnicity and language (bilingual vs monolingual) did not predict significant differences in participants’ reports of the primary measures of interest. Participants were compensated US$75. All Latina women were primarily first-generation immigrants (Dominican: 77% foreign-born, Mexican: 95% foreign-born, χ2(1, N = 132) = 9.07, p = .003, ϕ = .26). A subset of the Latina sample (74%) was examined in a previous study (Halim et al., 2013), which examined a mother’s perceived discrimination in relation to her infant’s health.
Measures
Perceived ethnic discrimination
Women’s perceptions of ethnic discrimination were assessed averaging six items adapted from the Everyday Discrimination Scale (Williams et al., 1997), including
How often have you (been treated with less courtesy than other people/had trouble finding a job/received poorer service than other people at stores, restaurants, or banks/been treated poorly at work by coworkers/been treated poorly at work by supervisors/been treated poorly by the police) because you are (ethnicity)? (0 = Never, 1 = Rarely, 2 = Sometimes, 3 = Often; α = .78).
Item wording was adapted to be more sensitive to the experiences and stereotypes of Latina women.
Perceived language-based discrimination
Women’s perceptions of language-based discrimination were also assessed. We averaged six items adapted from the above perceived ethnic discrimination items, with the substitution of “ …because of how you wrote or spoke English” for “ …because you are (race/ethnicity)” (α = .78). Seven women were missing data. Five of these seven (4 Dominican, 1 Mexican) reported that these questions did not apply to them, and two were not asked these questions due to an interviewer error.
Psychological distress
Psychological distress experienced in the past 30 days were measured using Kessler’s K6 questionnaire (e.g. “During the past 30 days, about how often did you feel hopeless?” (1 = None of the time, 2 = A little of the time, 3 = Some of the time, 4 = A little of the time, 5 = All of the time) (Kessler et al., 2002) (M = 1.89, SD = .73).
Overall physical health
Participants reported their overall physical health (“Overall, how would you describe your health?” 1 = Poor, 2 = Fair, 3 = Good, 4 = Very good, 5 = Excellent) (McGee et al., 1999).
Demographic variables (covariates)
At the time of the child’s birth, participants reported annual household income (mean-centered). Participants’ education level was treated as a categorical variable (completed some college vs only completed high school or received a General Educational Development (GED) degree vs. did not complete high school) and dummy coded (0 = less than a high school education). Additional covariates included marital status (0 = unmarried, 1 = married), cohabitation status (0 = living alone, 1 = living with child’s father), age (mean-centered), and race/ethnicity. Ethnic group was included as a dummy variable in all analyses with Dominican-immigrant women as the reference group. For analyses on language-based discrimination, language of the interview was additionally included as a covariate (0 = English, 1 = Spanish; see Supplemental Materials).
Results
In the following section, we first describe ethnic group differences among the measures that we collected. We then examine whether ethnic discrimination predicts poorer mental and physical health in Latina immigrant women. Next, we further examine whether language-based discrimination also predicts poorer mental and physical health. Finally, we conducted analyses to understand how ethnic and language-based discrimination together predict health outcomes in Latina women. Correlations among variables can be found in Supplemental Materials.
Ethnic variation in measures
For the independent measures, Dominican immigrant women (M = .37, SD = .46) reported less perceived ethnic discrimination compared to Mexican immigrant women (M = .57, SD = .58), t(130) = 2.21, p = .029, d = .39. However, Dominican (M = .42, SD = .61) and Mexican immigrant women (M = .56, SD = .61) did not significantly differ in levels of perceived language-based discrimination, t(123) = 1.29, ns.
For the dependent measures, the two ethnic groups did not significantly differ in levels of psychological distress (Dominican: M = 1.90, SD = .78; Mexican: M = 1.87, SD = .63), t(130) = .26, ns. However, Mexican immigrant women (M = 3.03, SD = .88) reported poorer overall physical health compared to Dominican immigrant women (M = 3.48, SD = .99), t(130) = 2.72, p = .007, d = .48.
Perceived ethnic discrimination and health
We conducted two regressions with levels of psychological distress and physical health as outcomes. Predictors for both regressions included perceived ethnic discrimination and the demographic covariates. We hypothesized that greater perceived ethnic discrimination would be associated with higher levels of psychological distress and poorer overall physical health. Results confirmed our hypotheses (see Table 1).
Regression results of perceived ethnic discrimination predicting mental and physical health in Latina immigrant women.
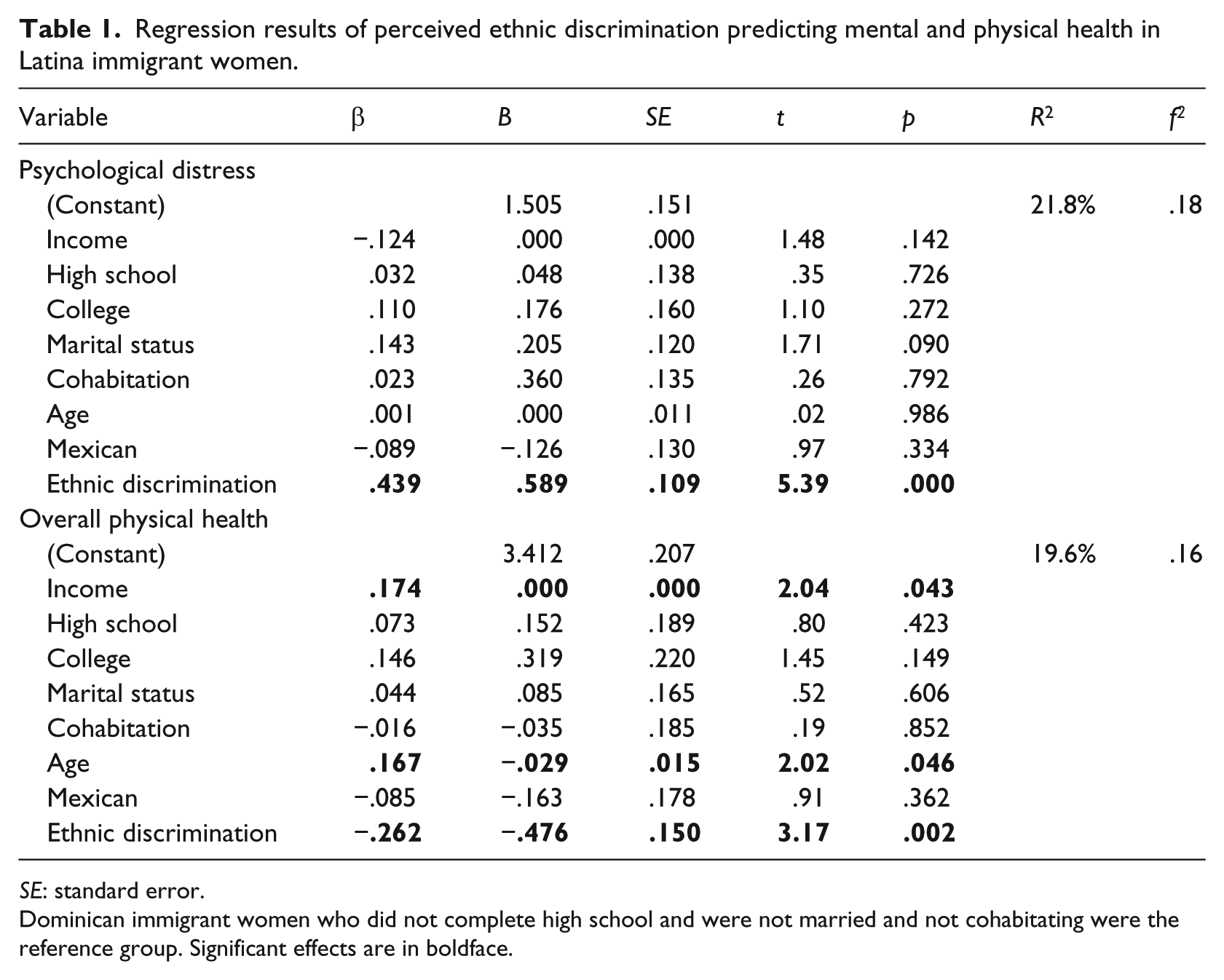
SE: standard error.
Dominican immigrant women who did not complete high school and were not married and not cohabitating were the reference group. Significant effects are in boldface.
Perceived ethnic discrimination was associated with higher levels of psychological distress, B = .59, β = .44, t(131) = 5.39, p = .001, and poorer physical health, B = −.48, β = −.26, t(131) = 3.17, p = .002. Exploratory analyses including interactions between perceived ethnic discrimination and ethnicity revealed no significant interactions.
Perceived language-based discrimination and health
We conducted two hierarchical multiple regressions. To examine whether perceived language-based discrimination was associated with higher levels of psychological distress and lower levels of physical health, in the first step we conducted regressions identical to those above with the exception that perceived language-based discrimination was substituted for perceived ethnic discrimination. In addition, language of the interview was included as a covariate. Results confirmed our hypotheses (see Table 2, Step 1).
Regression results of perceived language-based and ethnic discrimination predicting mental and physical health in Latina immigrant women.
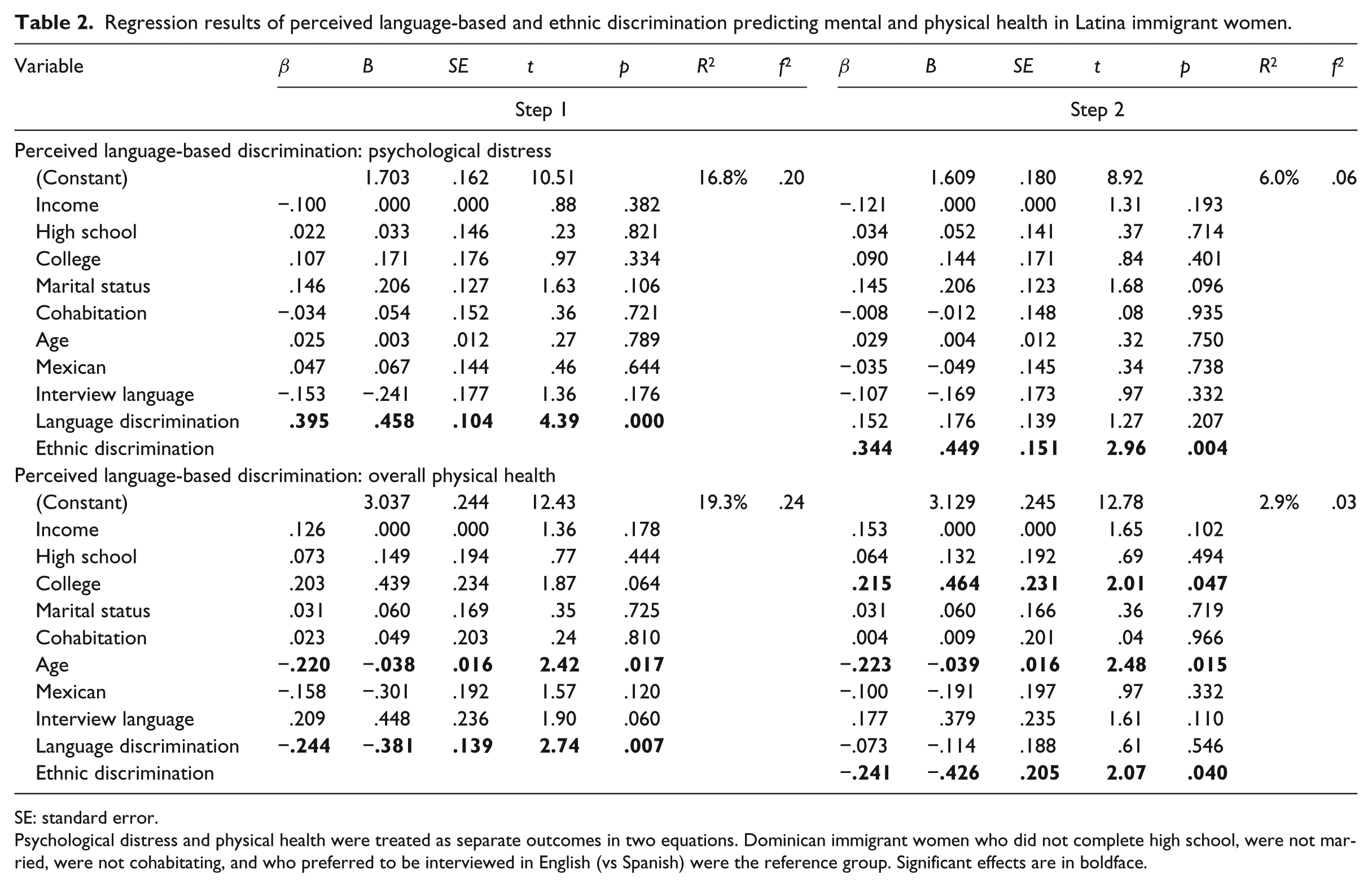
SE: standard error.
Psychological distress and physical health were treated as separate outcomes in two equations. Dominican immigrant women who did not complete high school, were not married, were not cohabitating, and who preferred to be interviewed in English (vs Spanish) were the reference group. Significant effects are in boldface.
Greater perceived language-based discrimination predicted higher levels of psychological distress, B = .46, β = .40, t(124) = 4.39, p < .001, and poorer physical health, B = −.38, β = −.24, t(124) = 2.74, p = .007. Exploratory analyses including interactions between perceived language-based discrimination and ethnicity revealed no significant interactions.
Interplay between perceived ethnic and language-based discrimination in predicting health
To understand how perceiving multiple forms of discrimination together affect health outcomes in Latina immigrant women, on the second step of the same two hierarchical multiple regressions as mentioned above, we added perceived ethnic discrimination as a predictor. Results revealed that, in the second step, only perceived ethnic discrimination predicted higher levels of psychological distress, B = .45, β = .34, t(124) = 2.96, p = .004, and poorer physical health, B = −.43, β = −.24, t(124) = 2.07, p = .040. Perceived language-based discrimination was no longer a significant predictor of psychological distress, B = .18, β = .15, t(124) = 1.27, p = .207, or physical health, B = −.11, β = −.07, t(124) = .61, p = .546. Exploratory analyses conducting analyses separately for Mexican and Dominican women showed no significant differences in these patterns, suggesting that these associations were robust across ethnic groups (see Table 2, Step 2).
Discussion
Among Latina immigrant women, consistent with previous research, this study showed that perceiving ethnic discrimination was associated with experiencing higher levels of psychological distress and lower self-reported health. This relation was robust across ethnic groups, as this association held for both women of Mexican and Dominican descent. Perceiving language-based discrimination was also associated with experiencing higher levels of psychological distress and lower self-reported health. This finding adds to the scant literature that exists about the potential consequences of perceiving language-based discrimination. Our results reveal additional consequences that are linked to language-based discrimination besides utilizing mental health care services, reporting chronic health conditions, and engaging in risky health behaviors (Spencer and Chen, 2004; Yoo et al., 2009; Yoshikawa et al., 2004). Our study also had the benefit of examining components of both mental and physical health within one single study. This allowed us to see how perceived discrimination plays a role in a person’s overall well-being. Furthermore, this research extends the language-based discrimination and health literature by showing that this link generalizes beyond Asian and Pacific Islander immigrants to Latina immigrants as well.
When we examined the two types of discrimination together, perceiving ethnic discrimination remained associated with poorer mental and physical health, whereas language-based discrimination was no longer a significant predictor. This finding is consistent with previous work comparing the impact of ethnic discrimination and language proficiency on psychological distress (Zhang et al., 2012). This finding also supports the hypothesis that perceiving ethnic compared to language-based discrimination may be more stressful, and thus be more strongly linked to health outcomes. Perhaps ethnicity may seem more permanent and less under one’s control, whereas the way one speaks can be shaped and improved. Thus, ethnic discrimination may seem inevitable, inescapable, and unending. Ethnicity could also be viewed as a more internal characteristic and more central to Latina women’s self-concepts compared to language. This may lead Latina women to take the implications of ethnic versus language-based discrimination more to heart. It is also possible that ethnic discrimination mediates the link between language-based discrimination and health. That is, if an individual perceives discrimination due to how one speaks English, that individual may then perceive more ethnic discrimination as well, and perceptions of ethnic discrimination would, in turn, predict poorer health. Future longitudinal and/or causal evaluation methods are needed to test this possibility.
Although our data suggest that ethnic versus language-based discrimination is a stronger predictor of health outcomes for Latina women, language-based discrimination still deserves attention as an important construct to study. When examined alone, language-based discrimination was associated with poorer mental and physical health. Moreover, in our sample, ethnic and language-based discrimination were distinct, but moderately correlated with each other. This correlation suggests that in everyday life, it is highly possible for immigrants to experience both types of discrimination. Thus, for ecological validity, further research on discrimination and health should include both types to further disentangle their effects and better understand their intersection.
The correlation between ethnic and language-based discrimination also suggests that women who report higher levels of ethnic discrimination will tend to report higher levels of language-based discrimination and vice versa. The correlation also suggests that those who perceive little of one type of discrimination will tend to perceive little of the other. Thus, there may be interesting individual differences to further explore in future research. Who are these women who perceive high or low levels of both types of discrimination? Are some women more sensitive to discrimination than others, vigilant to negative treatment, and more ready to interpret their treatment as based on race/ethnicity or language? Or do some women actually experience more discrimination than others due to their personal qualities or their environments? Several factors are likely involved, and understanding these individual differences is an important avenue to pursue.
Overall levels of perceived discrimination and ethnic group differences
Of note, we found associations between discrimination and health although the overall reported levels were relatively low on average (.37–.57 on a scale from 0 to 3, indicating perceiving discrimination between never and rarely). Indeed, many women in our sample reported never perceiving any discrimination at all across multiple contexts (30% for ethnic discrimination, 38% for language-based discrimination). The Dominican women in our sample mostly lived in communities where many neighbors spoke Spanish and were Dominican as well (on average 35% of their neighbors were Dominican, with a range from 3% to 80%) (XXX). Hence, these ethnic enclaves may have protected them from encountering high levels of discrimination from other-ethnic individuals. In addition, studies have shown that people, in general, are often hesitant to report personal experiences with discrimination (Taylor et al., 1990). We speculate that this might be especially true of first-generation immigrants. Nevertheless, although overall levels of perceived discrimination were low, we still found meaningful associations with mental and physical health. This suggests that, perhaps, even infrequent perceived discrimination can harm an individual.
Mexican and Dominican women perceived similar levels of language-based discrimination. However, Mexican women perceived more ethnic discrimination compared to Dominican women. We speculate that this difference might have been due to two factors. First, the Mexican women in our sample, on average, had darker skin than the Dominican women in our sample. Thus, others might have perceived the Mexican women as more Latino/a or as more of a foreign immigrant, making the Mexican women more susceptible to ethnic discrimination. Indeed, past studies have shown that there is a bias against having darker skin (Arce et al., 1987) and people stereotype and tend to mistreat worse individuals who look more versus less racially stereotypical (Eberhardt et al., 2006). Second, in New York, the Mexican immigrant community is newer than the Dominican immigrant community. Hence, unlike the Dominican sample, our Mexican sample lived in different areas of New York City and few lived in Spanish-speaking ethnic enclaves. The Mexican women lived in communities where only, on average, 7 percent of neighbors were also Mexican, and this percentage ranged from 0 to 27 percent for the whole sample (Yoshikawa, 2011). Mexican women in our sample might thus have had increased chances of encountering situations with other-ethnic individuals that might have involved discrimination. Overall, these findings suggest that Mexican immigrant women might face acute challenges in coping with not only language-based discrimination but also higher levels of ethnic discrimination.
Limitations and future directions
There are some limitations to this study. First, we have assumed that one important mechanism linking discrimination to mental and physical health is through a physiological stress response. Alternatively, discrimination may be linked through worse health behaviors. While these mechanisms have been well-supported for ethnic discrimination (Pascoe and Richman, 2009), it has yet to be seen if the same mechanisms holds true for language-based discrimination. In addition, although our measure of physical health has been validated in past research, a limitation of our study was that we did not include additional outcomes, such as chronic illness and use of health care services. Second, in this study, we were unable to include a measure of English proficiency when testing the relation between language-based discrimination and health. There is emerging research showing that low English proficiency predicted poorer quality of life and poorer health in Asian Americans (Gee and Ponce, 2010). It would be interesting to directly examine the distinct or interactive effects of language-based discrimination versus language proficiency on health outcomes. Finally, our sample was limited to Dominican and Mexican mothers from the New York metropolitan area. Future research should test whether these relations generalize to childless women, to other Latino/a groups, to individuals living in other regions, and to men. In terms of looking at men versus women, reviews of the literature on ethnic discrimination and health show generalizability across genders in the majority of existing studies (Pascoe and Richman, 2009; Williams et al., 2003). The few studies on language-based discrimination and health do not explicitly examine moderation by gender (e.g. Spencer and Chen, 2004; Yoo et al., 2009). We speculate that perhaps the correlation between language-based discrimination and health would hold across both genders, but perhaps the mechanisms (Kim et al., 2011), levels (Krieger and Sidney, 1996), or ways in which to cope with discrimination could vary by gender (Krieger and Sidney, 1996; Spencer and Chen, 2004).
Conclusion
For many ethnic minorities, perceiving discrimination based on ethnicity may be a part of everyday life—at work, at the grocery store, when going out to eat, in dealing with public services; the list goes on. For immigrants, an added component of everyday life may be perceiving discrimination based on the way one speaks the host language. Many ethnic minority immigrants may take these perceptions in stride, accepting them as just part of the fabric of a stratified society, especially when discourteous treatment seems insignificant. However, our study underscores that these types of perceptions are not trivial. Mean levels of perceptions of discrimination were surprisingly low. Nevertheless, even perceiving discrimination rarely or some of the time increased the risk of poorer mental and physical health. Our results also suggest that we may need to pay particular attention to perceptions of ethnic discrimination for Latina women, as these perceptions had stronger ties to health than did language-based discrimination. More broadly, as our sample consisted of mothers of infants, and as the link between mother and infant health gathers more evidence, our findings have implications not only for the health of ethnic minority women but possibly for the health and development of future generations as well. Thus, our findings emphasize the importance of reducing ethnic and language-based discrimination for the well-being and health of many individuals.
Footnotes
Acknowledgements
This study was conducted at the New York University Center for Research on Culture, Development, and Education (CRCDE), within the Department of Applied Psychology at New York University’s Steinhardt School of Culture, Education, and Human Development. We thank our colleagues and staff at the CRCDE, particularly Amanda Flores-Schrey, Odessa Despot, Fernanda Lucchesse, Lisa Tafuro, Erica Ramos, Erika Niwa, Joy Chung, Patricia Rojas, and Yana Raufova, the mothers and children who participated in our research, and Kay Deaux for her feedback on earlier versions of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the National Science Foundation grants BCS 021859 and IRADS 0721383 to H. Yoshikawa.