
Abstract
This study investigated the association between the 3-month postoperative sense of coherence and the 5-year postoperative outcome of decompressive surgery for lumbar spinal stenosis. The participants with a lower sense of coherence at the 3-month follow-up had a poorer functional ability and lower satisfaction with surgery, higher pain ratings, lower life satisfaction and more depressive symptoms 5 years postoperatively. A low 3-month sense of coherence associated with greater pain and a poorer functional ability 5 years postoperatively. Evaluating sense of coherence and depressive symptoms in patients who have had lumbar spinal stenosis surgery may help in identifying those in need of enhanced support for postoperative recovery.
Background
Sense of coherence (SOC) was developed by Antonovsky (1981) as a concept of salutogenesis, according to which the orientation towards life is intricately connected with health. Antonovsky described this as a way of seeing life as comprehensible, manageable and meaningful. SOC is associated with good coping abilities and good mental health (e.g. Geyer, 1997). Those with a greater SOC generally appear to cope better when facing different somatic diseases (Chumbler et al., 2013; Eriksson and Lindström, 2005, 2006), although contrary findings have also been reported (Flensborg-Madsen et al., 2005). SOC mostly develops during youth and is seen as a relatively stable measure. Nevertheless, SOC can be affected by various life-changing events (Snekkevik et al., 2003; Volanen et al., 2007) and can also improve with age (Feldt et al., 2011; Nilsson et al., 2010).
SOC has been associated with depressive symptoms (e.g. Eriksson and Lindström, 2006; Erim et al., 2011; Geyer, 1997). A low SOC may predict the later onset of depression (Luutonen et al., 2011; Sairenchi et al., 2011), while a high SOC may protect against it (Büchi et al., 1998). Improvement in SOC has corresponded with recovery from depression (e.g. Skärsäter et al., 2005) and SOC might also improve with psychosocial interventions (Kähönen et al., 2012; Langeland and Wahl, 2009). Furthermore, SOC has associated with depression in somatically ill patients, for instance with cardiovascular diseases (Haukkala et al., 2013), and with musculoskeletal and spinal problems (Badura-Brzoza et al., 2008; Sinikallio et al., 2011; Büchi et al., 1998).
Lumbar spinal stenosis (LSS) is a common and chronic condition, especially among the elderly population (Kalichman et al., 2009). The first choice for its treatment is conservative (Genevay and Atlas, 2010), but when conservative treatment fails, surgery is indicated (Kovacs et al., 2011). Indicators of decreased mental health, such as depression, anxiety and poor coping (Celestin et al., 2009), have previously been reported to modulate the outcome of surgery among patients with lumbar problems. In LSS, this especially appears to be the case with depressive symptoms (e.g. Sinikallio et al., 2007; McKillop et al., 2014; Pakarinen et al., 2014). Although some studies have yielded variable results (Aalto et al., 2011; Abbott et al., 2010; Mannion et al., 2007) for different postsurgical rehabilitation methods (mainly focusing on physiotherapy), postoperative rehabilitation in LSS has proven effective according to a recent meta-analysis (McGregor et al., 2013). Nevertheless, taking psychosocial aspects in consideration in postoperative rehabilitation might improve the outcomes (Abbott et al., 2010; Christensen et al., 2003).
LSS surgery can be seen as a major life event, and as such may have an effect on SOC (Volanen et al., 2007). In spinal patients, psychological distress is associated with a poorer SOC (Badura-Brzoza et al., 2008), and in earlier studies on LSS patients, SOC has strongly associated with depressive symptoms (Sinikallio et al., 2006, 2011). In patients with low back surgery, SOC correlated significantly with the disability score and had good predictive value postoperatively (Santavirta et al., 1996a, 1996b). According to an earlier study by Sinikallio et al. (2011), preoperative SOC interfered with postoperative recovery among LSS patients in a 1-year follow-up. However, we are unaware of previous follow-up studies in this patient group exceeding a duration of 1 year.
This study was the first to investigate the association between SOC and the outcome of LSS surgery over a 5-year follow-up. We focused on the 3-month SOC due to its role in clinical decision-making with respect to postoperative LSS rehabilitation. At this follow-up point after surgery, the overall level of recovery of patients is evaluated, and any possible activity restrictions are lifted on the instruction of the surgeon. Thus, this evaluation point may offer potential for redelineating the recovery plan of patients if considered necessary.
Methods
Study design
The present prospective clinical study included participants with radiologically and clinically defined LSS who underwent decompressive surgery. Selection for surgery was carried out by an orthopaedist or a neurosurgeon at Kuopio University Hospital, between October 2001 and October 2004. Altogether, 102 participants received an account of the study during their outpatient visit to the Department of Physical and Rehabilitation Medicine, provided informed consent and responded to the study questionnaires. After 5 years of follow-up, 6 subjects had died, 11 could not be reached and 11 did not complete the questionnaires. Thus, at the 5-year follow-up, 74 of the original subjects responded to the questionnaires.
As our study design was naturalistic, participation in the study did not change the treatment delivered at the clinical unit at the time of this study. However, half of the participants received physical exercise intervention (PEI) (Aalto et al., 2011). The aim was to recruit all criteria-fulfilling participants with LSS. The study design has been described in more detail by Sinikallio et al. (2006) and Aalto et al. (2006, 2011) and was approved by the Ethics Committee of the University of Eastern Finland and Kuopio University Hospital.
The inclusion criteria for the study population were the presence of (a) severe pain in the back, buttocks and/or lower extremities; (b) radiographic evidence of compression of the cauda equine or degenerative changes in the nerve roots and (c) the surgeon’s clinical evaluation of degenerative LSS requiring operative treatment. All participants also had a history of ineffective responses to conservative treatment, such as use of analgesics, physiotherapy and/or guided physical exercise in a gym. The exclusion criteria were as follows: emergency or urgent spinal surgery precluding recruitment and protocol investigations, cognitive impairment prohibiting completion of the questionnaires or other failures in co-operation and the presence of metallic particles in the body preventing the magnetic resonance imaging (MRI) investigation.
All the participants underwent open or microscopic decompressive surgery of the affected level(s), that is, laminotomy, hemilaminectomy or laminectomy, with undercutting facetectomy. In total, 19 participants had additional fusion (two with instrumentation). All the participants received routine preoperative information at the hospital about immediate postoperative mobilisation. They were advised to remain active with no restrictions on normal daily living.
Participants undertook routine follow-up visits to the orthopaedic or neurosurgical clinic postoperatively, at which the surgeon also confirmed that there were no restrictions on rehabilitation. PEI started 3 months postoperatively for half of the participants. Other postoperative treatments (e.g. analgesics, other types of physiotherapy) prescribed by the surgeon/general practitioner (GP) were not prohibited. PEI included a supervised training session once a week lasting for 12 weeks and was repeated 12 months postoperatively, but this intervention was not found to influence the surgical outcome in a 2-year follow-up (Aalto et al., 2011).
Questionnaires
Data collection took place before surgery and 3 months and 5 years postoperatively using the same questionnaires. Questions concerning sociodemographic background, lifestyle and health were included in the preoperative questionnaire, which was mailed to the participants by the secretary (at the 5-year follow-up point by a nurse) of the Department of Physical and Rehabilitation Medicine. The questionnaires have been described in more detail by Sinikallio et al. (2006) and included the following:
Self-reported walking capacity in metres (continuous scale) (Aalto et al., 2006).
Estimation of overall back and leg pain intensity with a visual analogue scale (VAS: 0–100 mm), 0 mm indicating ‘no pain’ and 100 mm ‘the worst possible pain’ (Price et al., 1983).
Comorbidity assessed with one modified item (item number 3) of the Work Ability Index (WAI) questionnaire: the self-reported number of current or recurring diseases diagnosed by a physician (range 0–49). The number of diseases was then recorded as a sum score (Tuomi et al., 1998).
Subjective disability measured with the validated Finnish version of the Oswestry Disability Index (ODI; scale 0%–100%: where 0% equals no disability and 100% equals extreme disability; Fairbank et al., 1980; Fairbank and Pynsent, 2000);
Satisfaction with the surgical outcome assessed using a 7-category scale as follows: −3 = surgery was a total failure, −2 = condition is now considerably worse, −1 = condition is now slightly worse, 0 = no change, 1 = condition has slightly improved, 2 = condition has considerably improved and 3 = totally cured (Sinikallio et al., 2007).
Assessment of life satisfaction (LS) with a 4-item self-evaluation scale (LS-4; range 4–20, higher scores indicating lower satisfaction) (Allardt, 1973; Koivumaa-Honkanen et al., 2005).
Assessment of depressive symptoms with the Finnish version of the 21-item Beck Depression Inventory (BDI) (range 0–63), higher scores indicating more depressive symptoms (Beck et al., 1961).
Assessment of SOC with the validated 13-item SOC scale (range 13–91). Each item has response options on a 7-point Likert scale. There are no specific cut-off values for high/normal/low SOC scores. Thus, we used the mean score as the cut-off in our analyses, with higher scores indicating better coping resources (Antonovsky, 1981, 1993).
Statistical analyses
Statistical analyses were performed using SPSS/PC (version 19.0; SPSS, Chicago, IL, USA), with p < 0.05 considered to indicate statistical significance.
The means were compared using the Student’s t-test and the Kruskal–Wallis test where appropriate. Cross-sectional analysis was performed by comparing the groups with a higher and lower SOC at the 3-month and 5-year follow-up points. Longitudinal analyses were also performed to compare the change within the groups between the 3-month and 5-year follow-up points.
Several linear regression models (method: enter) were tested – four models for the 5-year ODI and the 5-year VAS and two models for the 5-year SOC. All the models were adjusted for age and gender.
In the first model for the 5-year ODI, the predictive values of the 3-month SOC, walking capacity and VAS were assessed. An additional 3-month variable, BDI, was included in the second model, satisfaction with surgery in the third model and receiving/not-receiving PEI in the fourth model. The models for the 5-year VAS were similar, except that the 3-month VAS was replaced with the 3-month ODI.
In the model for predicting the 5-year SOC, the first model included walking capacity, ODI, BDI and VAS, and the second model receiving/not-receiving PEI as an additional 3-month variable.
Results
The mean age of the study group at the 5-year follow-up point was 67 (standard deviation (SD) 11) years and 35 per cent were male. The mean SOC score was 73 (SD 12) at the 3-month and 71 (SD 12) at the 5-year follow-up point.
The group with a lower SOC at the 3-month follow-up point also concurrently had higher pain ratings, more depressive symptoms and less satisfaction with life than the group with a higher 3-month SOC. At the 5-year follow-up point, a low 3-month SOC was associated with more depressive symptoms, lower LS, higher pain ratings, lesser satisfaction with surgery and a poorer functional ability (ODI) (Table 1).
Three-month and 5-year characteristics in relation to the 3-month sense of coherence.
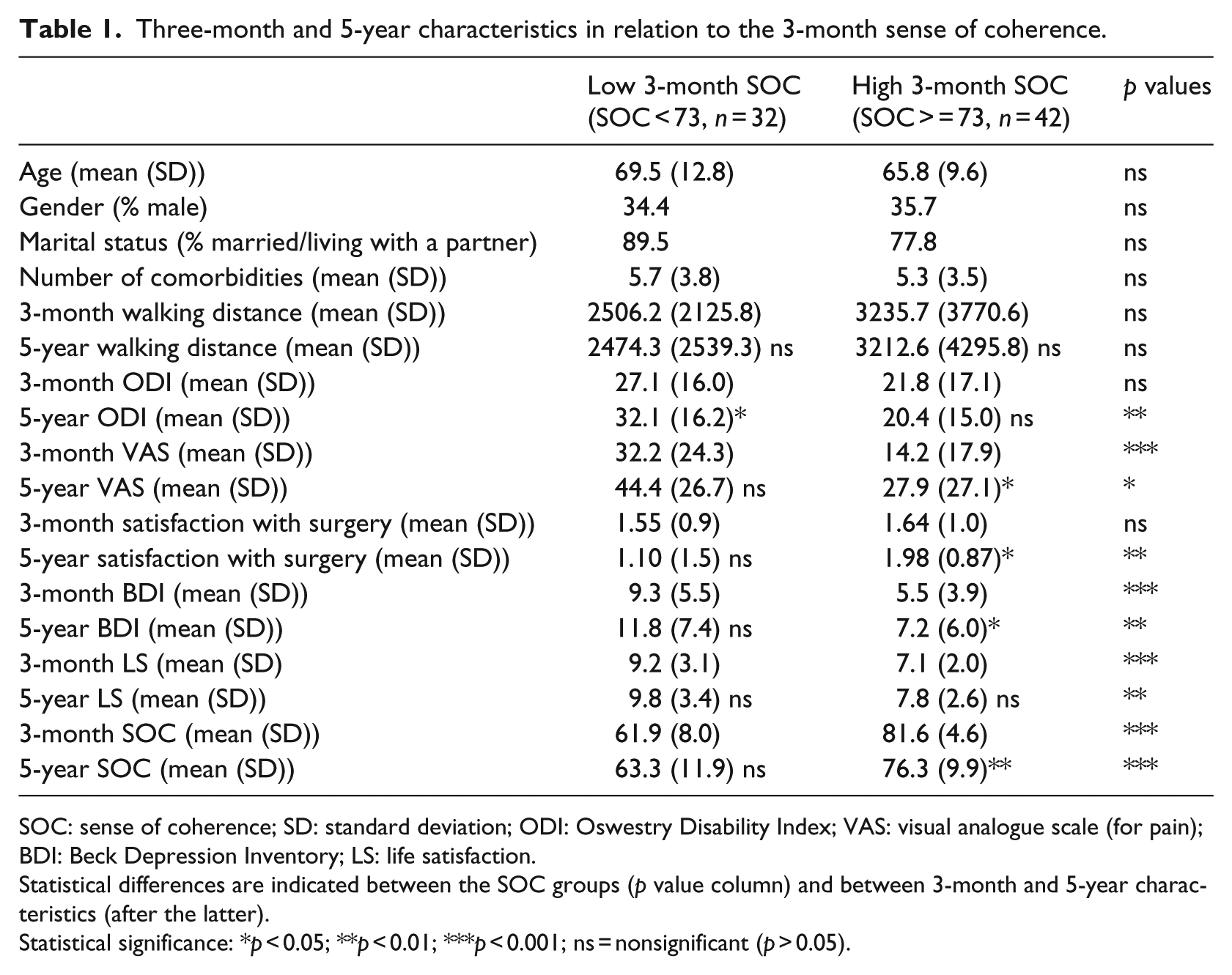
SOC: sense of coherence; SD: standard deviation; ODI: Oswestry Disability Index; VAS: visual analogue scale (for pain); BDI: Beck Depression Inventory; LS: life satisfaction.
Statistical differences are indicated between the SOC groups (p value column) and between 3-month and 5-year characteristics (after the latter).
Statistical significance: *p < 0.05; **p < 0.01; ***p < 0.001; ns = nonsignificant (p > 0.05).
In the follow-up, we compared the change within the groups having a lower and higher 3-month SOC. In the group with a lower SOC, ODI significantly decreased between the 3-month and 5-year follow-ups, while in the group with a higher 3-month SOC, VAS and BDI increased and SOC decreased between these follow-ups. However, satisfaction with surgery was higher at the 5-year follow-up point (Table 1).
In linear regression analysis, the 3-month SOC and walking distance were independently associated with the 5-year ODI (Table 2). These associations remained the same after adjustments for 3-month surgery satisfaction, which also had an independent association with the 5-year ODI (B = −4.06, standard error (SE) = 2.02, p < 0.05). When the 3-month BDI was adjusted for, the only significant association was between the 3-month walking distance and 5-year ODI (B = −0.00, SE = 0.00, p < 0.05). After adjustments for receiving/not-receiving PEI, the associations were similar to the first model, but PEI was not associated with the 5-year ODI (B = −3.14, SE = 4.10, p = ns).
Linear regression analysis in relation to ODI and VAS at the 5-year follow-up point (B values shown with standard error).
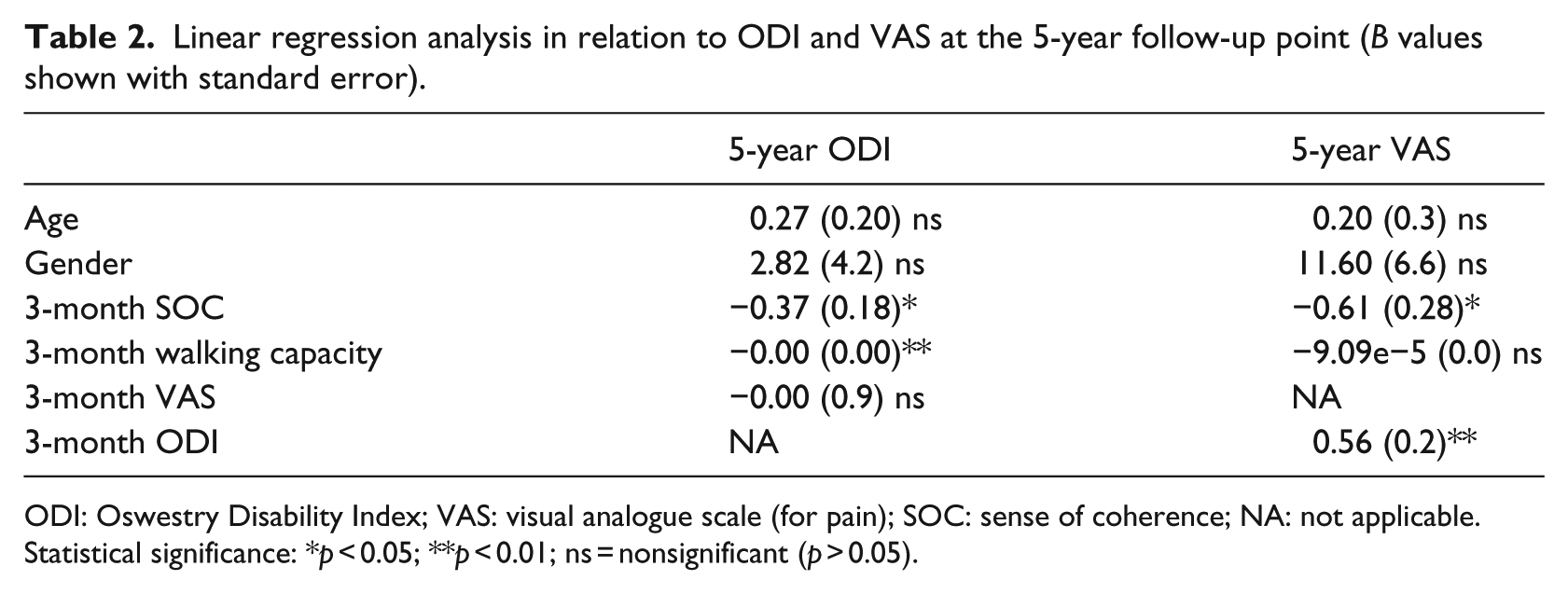
ODI: Oswestry Disability Index; VAS: visual analogue scale (for pain); SOC: sense of coherence; NA: not applicable.
Statistical significance: *p < 0.05; **p < 0.01; ns = nonsignificant (p > 0.05).
In the first linear regression model for the 5-year VAS, the 3-month ODI and SOC had an independent association with the 5-year VAS (Table 2). This association was also seen when BDI was adjusted for (B = −0.79, SE = 0.31, p < 0.01). In the model in which satisfaction with surgery was adjusted for, an association between the 3-month SOC and 5-year VAS was also observed (B = −0.62, SE = 0.28, p < 0.05). After adjusting for receiving/not-receiving PEI, the associations were similar to the first model, and PEI had no association with the 5-year VAS (B = −11.04, SE = 0.6.38, p = ns).
In linear regression analysis for the 5-year SOC, we used a model for the 3-month variables. A significant association was detected between a low SOC and a high BDI (Table 3). When including receiving/not-receiving PEI in the analysis, the same association between the 3-month BDI and 5-year SOC was observed (B = −1.33, SE = 0.34, p < 0.001), and PEI was not associated with SOC.
Linear regression analysis in relation to SOC at the 5-year follow-up point.

SOC: sense of coherence; ODI: Oswestry Disability Index; BDI: Beck Depression Inventory; VAS: visual analogue scale (for pain).
Statistical significance: **p < 0.01; ns = nonsignificant (p > 0.05).
Discussion
This was the first study to examine the associations between postoperative SOC and the long-term outcomes of LSS surgery. The analyses were performed according to the 3-month SOC, since this follow-up point after surgery was the time at which any possible activity restrictions were lifted on the instruction of the surgeon, and because of this, it can be a definitive changing point in the recovery process.
The main finding in our study was the association between a low SOC and a poorer surgical outcome. After multiple adjustments, the 3-month SOC had predictive value for both higher pain ratings and poorer functional capability at the 5-year follow-up. The latter association has also been observed in a 1-year follow-up (Sinikallio et al., 2011). Although low SOC has been linked with disability in other spinal conditions (e.g. Santavirta et al., 1996a, 1996b), some studies considering other medical conditions have not detected such an association (e.g. Gison et al., 2014). This could be explained by differences in the pathophysiological processes, symptoms and rehabilitation of medical problems.
When comparing participants with a higher and lower 3-month SOC, life dissatisfaction, BDI and pain ratings were higher among those having a low SOC at the 3-month follow-up point. Interestingly, at the 5-year follow-up, in addition to BDI, VAS and LS, the 3-month SOC was also associated with satisfaction with surgery and functional capability. Thus, the participants with a higher SOC also had a better outcome at this later follow-up point.
Other studies have demonstrated that the surgical outcome in LSS often declines with time, but surgery is nevertheless considered to be more beneficial than conservative treatment for up to 3–4 years, and possibly even 10 years (Amundsen et al., 2000; Anjarwalla et al., 2007; Atlas et al., 2005; Katz et al., 1996). In our study, the functional capability actually slightly weakened during the follow-up in the group with a lower 3-month SOC. Furthermore, in the group with a higher SOC, pain ratings, SOC and BDI were worse at the 5-year follow-up when compared with the 3-month follow-up point. Interestingly, the group with a higher SOC was more satisfied with surgery 5 years than 3 months after the surgery, even though the pain ratings and BDI were slightly higher. This could be explained by their better adjustment to their illness and better coping mechanisms than participants in the group with a lower SOC.
Interestingly, the mean SOC in this participant group (mean = 73) was higher than among the Finnish general population (mean = 64) (Volanen et al., 2007) or among Finnish surgical low back patients (mean = 65) (Santavirta et al., 1996a). Our study population was older than in these earlier studies, and SOC has previously been shown to improve with age (Nilsson et al., 2010), which might explain the differences in the mean SOC. In studies on older patient groups (Lindmark et al., 2010), the mean SOC has been closer to ours. Nevertheless, in our study, those with a lower SOC, which was still relatively high, had a poorer outcome. The associations between ageing, health and SOC require further investigation.
In linear regression analysis, a strong association was observed between BDI and SOC. This is in line with earlier findings and underlines the significance of depressive symptoms in connection with a low SOC. Our results also suggest that those with a high postoperative SOC might benefit more from surgery in the long term and for a longer time than those with a low postoperative SOC. Thus, monitoring postoperative psychological distress would enable the identification of those at risk of poorer recovery. The BDI may be influenced by physical conditions. Nevertheless, it is one of the recommended tools for screening depression in spinal pain patients (Choi et al., 2014). The BDI is also acceptable and easy to use for both patients and clinicians and is in wide clinical use, which allows for direct clinical comparisons.
Very few studies have included psychosocial support as a part of postoperative rehabilitation in LSS. Nevertheless, the results of these studies appear promising, suggesting that psychosocial support may improve treatment outcomes (Abbott et al., 2010; Christensen et al., 2003).
Altogether, these associations between SOC and different psychological and physical variables support the salutogenic model of health in the LSS participant group. Those with a higher SOC appeared to have a better outcome after surgery. The LSS participants with a lower postoperative SOC (i.e. more psychological distress) did not appear to gain as much benefit from the surgery as those with better psychological well-being, and depressive symptoms were also more common among them. In the future, psychological well-being should be taken into account when evaluating surgical patients preoperatively and during postoperative rehabilitation. Further research is needed to investigate the effects of interventions aimed at increasing postoperative SOC in patients with LSS.
Conclusion
SOC is associated with adverse psychological and physical outcomes of LSS surgery in the long term. Evaluating SOC and depressive symptoms in patients who have had LSS surgery may help in identifying those needing enhanced support for postoperative recovery.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: M.P. was supported by a grant from the Finnish Medical Foundation and S.M.L. was supported by a grant from the Finnish Cultural Foundation.