
Abstract
This study asked whether traceable knowledge transformations are occurring among indigenous Mexican women and, if so, the processes through which these shape their engagements with sexual health values and views. Thirty-nine interviews with rural and urban indigenous Mexican female adolescents were analysed through the lenses of social representations theory. Results evince that participants express transformations in terms of their social context, what constitutes a healthy youth and the uses of folk medicine, which are brought about by selecting, displacing and hybridising knowledge. Discussion centres on the consistency of themes across the sample and the variety of processes mapped.
In Latin America, the socioeconomic, social development and health indicators for indigenous peoples are worse than country averages, mirroring global trends (Macdonald, 2012; Montenegro and Stephens, 2006). In Mexico, 15.7 million people self-identify as indigenous, corresponding to 13.9 per cent of the population (INEGI, 2012). Although fertility rates have declined among both indigenous and non-indigenous Mexican women, indigenous females of fertile age report 2.7 births on average, one more birth than the national mean (INEGI, 2011: 25). Furthermore, 15.9 per cent of indigenous adolescents have at least one child, a significantly higher proportion than the 12.6 per cent of their non-indigenous counterparts (INEGI, 2012: 109).
Qualitative research examining the health of indigenous Mexican women has largely focused on customs, traditions and barriers to promoting healthcare-seeking behaviours. Recent studies in this field show that indigenous Mexican adult women’s knowledge of biomedical issues is at odds with those of health staff, and that they face pervasive structural barriers to accessing healthcare services, notably discrimination (Chopel, 2014; Gamlin, 2013; Smith-Oka, 2009). The literature evinces that these women make health decisions driven by a culture of secrecy (Chopel, 2014) and embarrassment (Gamlin, 2013), and a system of knowledge purporting a humoral understanding of health/illness (Smith-Oka, 2012). While this research is essential for fine-grained documentation of the contextual conditions of sexual and reproductive health of indigenous females, by focusing on adult, frequently middle-aged women, such studies reinforce representations of this group as marginal, backwards and with few resources to attain health. The disadvantages of being a woman in an indigenous group are indisputable, but few studies refrain from portraying these women’s identity and beliefs as fixed, culturally specific and ‘traditional’, with limited possibilities for change (González Montes, 2007, is a counterexample).
Research into indigenous adolescents’ understandings and experiences of sexual health has undergone a different process. In Latin America, this body of the literature is at an incipient stage (Pedrero and Oyarce, 2011) due to researchers historically converging on the idea that indigenous peoples in Latin America did not display a ‘transition period’ in the Western sense of youth, but that their move from childhood to adulthood was indicated by cohabitation (Feixa and González, 2005). However, researchers studying indigenous youth identity processes have recently disputed these assumptions by documenting that increased access to schooling, the ubiquity of mass media and constant contact with diverse ideas through migration and travel have all influenced a renewed understanding of this period (Manago, 2012; Pérez Ruiz, 2011; Saraví et al., 2014; Urteaga, 2011).
Against this backdrop, current ways of being young and indigenous by questioning traditions have recently been documented in Mexico. For instance, indigenous youth are declining the customary practice of arranged marriage at a young age, thereby enabling them to spend this time engaging in educational or work activities (Valladares de la Cruz, 2008: 88). Intergenerational change in terms of cultural values has been found among a Mayan community in Mexico: only indigenous adolescents enrolled in high school display ‘new cultural values’ of independence relative to those of their mothers, grandmothers and out-of-school counterparts (Manago, 2014: 871). Knowledge of medicinal plants previously used for reproductive health is being lost intergenerationally among Nahua indigenous women (Smith-Oka, 2008). Similarly, a recent report mentioned the interest expressed by indigenous adolescents in sexual and reproductive health education (Busquets et al., 2013: 39), which contrasts with the secrecy and embarrassment found among indigenous Mexican adults. This literature sheds light on current shifts in values, preferences and knowledge. However, existing accounts overlook the potential impact of these transformations on contemporary indigenous youth’s understandings of healthy/unhealthy practices. To bridge this gap, this study uses a psychosocial approach to examine representations of sexual health 1 among indigenous female adolescents, focusing on their dialogue with ideas and practices attributed to their elders. It seeks to address questions of whether traceable knowledge transformations are occurring among indigenous young women and, if so, the processes through which these shape their engagement with values and views on sexual health.
Theoretical underpinnings
The research presented here maps out social representations (Moscovici, 2008 [1961]), mobile and ever-changing sets of ideas, values and practices, constructed in dialogical engagements with the world, that furnish us with cognitive resources to apprehend social issues and to creatively respond to them (Jovchelovitch, 2007). Social representations theory (SRT) focuses on how lay people, in their everyday lives, make sense of scientific or abstract, yet socially relevant, notions such as health.
Social representations are constructed through dialogue: people use communication with others (be they physically present or absent individuals) and references to ideas and customs in order to inform their positions with respect to an issue (Marková, 2007). Mapping out the dialogue of indigenous adolescents with their ancestors, by means of their discursive accounts, is important to identify current health understandings and knowledge sources among a group that has consistently been associated with tradition.
The SRT tool of cognitive polyphasia – the coexistence of representational sources or ‘modalities of knowledge’ to explain and act upon a socially relevant issue (Moscovici, 2008 [1961]: 190) – is useful in ascertaining the processes through which knowledge transformations occur, which apply to this research. Drawing on the academic production on the subject, Jovchelovitch and Priego-Hernández (2015: 174–177) identified a typology of cognitive polyphasia:
Selective prevalence. Discrete types of knowledge are held together and used independently at different points in time/space.
Hybridisation. Several types of knowledge are retrieved concomitantly, producing a distinct amalgamated knowledge.
Displacement. One type of knowledge is chosen from a pool of parallel types, so that the latter are displaced in favour of the former.
This typology’s distinction of multifaceted types of knowledge and their interactions can potentially delineate the processes of knowledge construction and transformation with reference to the past (elders, communities) and present (adolescents themselves).
Methods
Study settings
Two settings in the highlands of central Mexico were considered, dovetailing with the distribution of indigenous peoples in urban/semi-urban (38%) and rural (62%) contexts (INEGI, 2012: 105). Tehuacán, the urban setting, is the second-largest city in Puebla State, and a municipality with ‘indigenous presence’ (20.8% of the population is indigenous; CDI, 2010). Tehuacán attracted indigenous migrants from the region in the late 20th century, due to its then booming textile industry, which declined markedly in the 2000s. The rural setting is located in an ‘indigenous municipality’ with 84.4 per cent indigenous inhabitants (CDI, 2010). Further particulars of the rural setting were anonymised, given its small size and potential for the identification of participants. Two non-governmental organisations (NGOs) were initially approached and served as gatekeepers for early contacts. Xasasti Yolistli and SEPICJ work on community development with indigenous women and youth, as well as other disadvantaged groups.
Ethical clearance was obtained from the Department of Social Psychology (then Institute) at the London School of Economics and Political Science and, as a funded doctoral project, initial research plans were submitted to the Mexican National Council for Science and Technology. Voluntary verbal informed consent was obtained from each participant. Permission from parents/guardians was sought for under-18 participants, but omitted if participants’ living conditions allowed them to decide study participation on their own (e.g. participant was head of household).
Data collection
Fieldwork was undertaken between January and May 2009, including indigenous youth aged 15–19 years, the World Health Organization benchmark for ‘late adolescence’. Selection relied on self-identification following criteria adopted by the Mexican Commission for the Development of Indigenous Peoples (Serrano Carreto et al., 2002), considering as indigenous those adolescents who spoke Nahuatl or whose head of household did. Nahuatl is an indigenous language spoken in both settings, which broadly designates participants’ membership of the Nahua indigenous group.
While efforts were made to include diverse schooling, sexual and reproductive experiences, the sampling strategy followed a corpus construction process: initial participants were contacted and, after a few interviews, additional participants were sought through referrals in order to expand the range of discursive themes, growing the corpus until no additional variability was found (Bauer and Aarts, 2000: 31). The interview guide consisted of three phases: first, health history; second, sexual health in participants’ own terms; third (interview core), sexual experiences, sexual outcomes and protective/risk-taking practices (questions adapted from Cleland et al., 2001). Thirty-nine indigenous female youth were recruited for in-depth interview (20 rural and 19 urban), which were conducted in Spanish by the author and lasted 78 minutes on average.
Data analysis
Using a larger data corpus and a different typology of cognitive polyphasia, the author (Priego Hernández, 2011) identified three general themes through thematic analysis procedures (Braun and Clarke, 2006) and the use of NVivo software: (a) the macro-level (society), (b) negotiations between romantic partners (relationships) and (c) micro-level, personal understandings of sexual health (beliefs).
For this article, data were examined by drawing on the preceding thematic analysis, focusing specifically on the ideas, values and practices that indigenous young females attributed to previous generations of indigenous peoples (distinguished from those of their partners and peers), and how they overlapped or differed from those of participants themselves. Dialogical theorists (e.g. Linell, 2009) refer to this analysis as the identification of the voices of third parties absent from the conversation (with the interviewer, in this case), dovetailing with the theoretical underpinning of social representations being constructed in dialogue.
The author summarised each individual interview, crosschecking details against the electronic coding. In terms of content, the author systematically noted instances in which participants referred to the knowledge, opinions, experiences and/or advice of their parents, older relatives and the community where they lived, and grouped them by theme in an iterative and inductive process. In terms of process, the already established categorisation of cognitive polyphasia (presented above) was used to distinguish how participants positioned themselves in relation to their elders about those themes, as represented in their speech (i.e. whether participants selectively aligned with the ideas they attributed to their elders, mixed those beliefs with some of their own or rejected them).
As a quality assurance measure, analytical and interpretative work in progress for this article was presented as a scientific conference paper (Priego-Hernández, 2014), seeking ‘peer debriefing’ (Lincoln and Guba (1985) in Flick, 2007).
Findings
Participants’ average age was 17.2 (SD = 1.3) years. Twenty were enrolled in education (7 rural and 13 urban) and an equal number reported sexual experience (penis-in-vagina intercourse; 12 rural and 8 urban), of which 14 had been pregnant at least once (9 rural and 5 urban). The majority of rural participants were engaged in agricultural activities, while work for the textile industry was a common source of income among urban participants. Fifteen urban participants were domestic migrants (7.8 years in the city on average), with 4 originating from Tehuacán.
The analysis rendered three themes, comprising two sub-themes each, as shown in Table 1. First, the changing context of sexual health, which is experienced in a social environment characterised by conservatism and hardship. Second, participants’ understandings of a healthy youth. Socially, youth is valued as a time to achieve goals of importance to participants and their families. Biologically, youth is perceived as a period of immaturity and growth. Third, engagements with folk and established medicine, which are favoured unevenly by participants depending on setting. The findings illustrate how these themes and their corresponding sub-themes were constructed in dialogue with the ideas and voices of their elders and communities through the cognitive polyphasic processes of selective prevalence, hybridisation and displacement.
Resulting themes and processes.
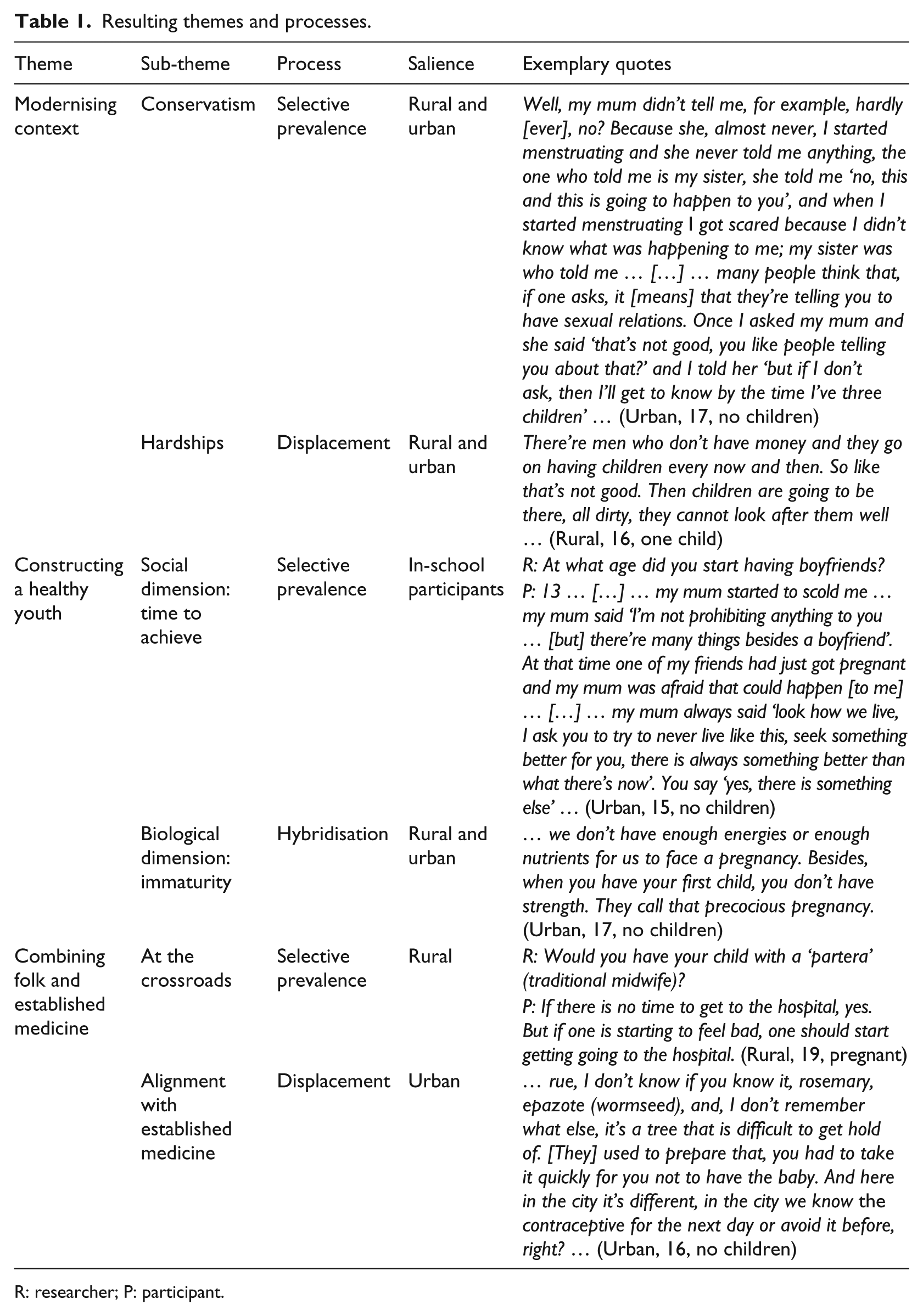
R: researcher; P: participant.
‘We are modernising’: contextualising sexual health
Participating indigenous young women set the broad, evolving context of their representations around the conservatism of their communities and the harsh living conditions they often experience. The perception of their communities’ conservatism and reserved approach to sexual education, romantic relationships and sexual topics in general was consensual across the sample, and participants acknowledged their own enacting of this demure approach to sexuality. While they frequently associated their elders with feelings of embarrassment and conservative attitudes, they simultaneously explained that such restrained demeanour is expected because they themselves are either in a village (rural participants) or from one (participants in both settings): … since we are village people, we almost don’t have communication with our parents, not much, little. Right now, let’s say that we are modernising: I’m the one who tells my things to my mum … (Rural, 18, no children) I don’t tell anything to my siblings. If they ask how [women] get pregnant, I say ‘who knows, I don’t’, because they’re too young for me to say that … in my village, nothing: nobody tells you how it’s a man with a woman; nobody would tell you, not even teachers, nothing. All I know is because I got to know here (in the city) … (Urban, 19, one child)
Participants in both settings acknowledged the need to discuss sexual topics and being furnished with knowledge, likening this learning process to a health need. At the same time, however, they tacitly stated stereotypes of backwardness and marginalisation that they have interiorised (they are, after all, ‘village’ people), likely exacerbated by talking to an outsider (researcher). Participants also admitted that at times, they also conform to their elders’ ‘discreet’ or ‘shy’ way of conveying information. This is a selective process that adapts the approach to sexual health to the social situation, demanding knowledge from those who know (elders, health and education professionals) yet quietly enacting conservatism, for example, by withholding such knowledge from those deemed too young to know.
There was also consensus about a general sense of hardship. Participants are acutely aware of the difficulties that their parents, extended families and they themselves have faced to achieve the (sometimes limited) quality of life they currently enjoy. They referred to their own experiences and those of their communities, in which the toil and hardships in life were shaped by sexual and reproductive decisions, including (delaying) sexual activity, birth spacing and (avoiding) bearing many children. When asking a rural participant, for example, about the number of children her mother had, she replied, ‘Five. [We are] all alive’, evoking the fact that, at the time her mother had children, infant mortality among indigenous populations was common. Participants reflected on how much a child ‘costs’ in material, emotional and symbolic terms: … it scares me when I hear that some ladies suffer a lot, their waist is broken when they are giving birth, their back, all their body aches. And I think ‘nothing hurts in me right now’… (Rural, 19, no children) I have a sister who, gosh, [has children] year after year, only now she stopped, and I’ve seen how she suffers … (Urban, 19, one child)
Indigenous young women positioned themselves as part of the indigenous group, which is consistently believed to marry girls early and to expect them to bear many children, according to agrarian modes of reproduction. In taking this as a reference to avoid, they also inserted themselves in the contemporary generation, with their current needs and projects, thereby questioning the relevance of the sexual and reproductive practices they have seen in others, distancing themselves from the evident disadvantages of past generations and displacing this knowledge for one that better suits their realities.
Constructing a healthy youth: social and biological dimensions
The social dimension of a healthy youth is defined by the behavioural expectations set in dialogue with ideas from elders. Participants referred to their expectations of heterosexual socialisation by questioning their parents’ understanding of romantic relationships in current times. They stressed the importance of having boyfriends and getting to know them, even if relationships did not lead to marriage. This is in stark contrast with their mothers, who had little time to enjoy socialisation with the opposite sex: [mum] had the need to go and work and buy her things. That’s why she says that she didn’t have time for boyfriends … But times change … (Rural, 15, no children)
Simultaneously, however, participants agreed with their parents’ expectations of delaying romantic engagements in order to avoid sexual activities. They acknowledged these teachings were intended to ensure that they were able to better themselves and accomplish educational attainments and a comfortable lifestyle, in contrast to the hardships experienced by their parents. Their parents’ and communities’ expectations are thus incorporated as young women’s individual life projects: … when my mum turned 14 she was pregnant with me. And now she says that I should not do the same … […] … I say ‘but I am 17 now and in comparison to when you had me’. [She] says ‘no, but now times have changed and you are too young to have a baby’… […] … it’s right, what my mum says, I am not prepared to have children. (Urban, 17, no children)
The perception of youth as a time to achieve was mapped out across the sample, although those who argued for the adequacy of such teachings were young women with no reproductive experience, especially those enrolled in education. This social dimension of a healthy youth entails a careful handling of tensions between positioning in agreement with participants’ elders regarding educational and material progress and subtly challenging them regarding a more open approach to socialisation with the opposite sex, in a selective process. In this way, it responds to the ‘modernising’ context theme by trying to move away from hardships and, slowly, away from a conservative approach to sexual matters.
The second dimension of a healthy youth is biological, manifested in the form of beliefs about the female body, which are nurtured both by popular knowledge handed down by older women and by medically legitimated knowledge attributed to health service providers. These beliefs emphasised the need for women to be fully grown, strong and with regular menstrual periods in order to conceive optimally. Some participants suggested that adolescents are not sufficiently mentally prepared to become parents. The understanding of youth as a period of immaturity was endorsed and displayed in both contexts: P
2
: … [mum said] ‘you still don’t have the age to be a mum’ … When would be an ideal age to be a mum, then? Who knows, we are told that between 18, 20 years. Then, as nurses say, the womb is more mature, well, it doesn’t get hurt. (Rural, 17, one child)
Participants suggested that this understanding of the body as being underdeveloped implies that their lives can literally be put at risk, that children born to adolescents might not achieve full development, and that calendar-based contraceptive methods are inappropriate for adolescents, due to their supposed menstrual irregularity. While in general these explanations were used to justify why young women should avoid early pregnancy, the same biological immaturity argument was used by girls with reproductive experience to justify the need for contraception to avoid further pregnancies: … [the doctor] said ‘if you want, have the [intrauterine] device, because you’re too young and got pregnant’. He said ‘but don’t do it again; do it by [age] 19, no, 20. Only then get pregnant, because you were too young when you got pregnant’… (Rural, 16, one child)
Some participants noted the dubiousness of the purported biological underdevelopment of adolescents by comparing themselves with their mothers and asserting that teenage childbearing is indeed possible and acceptable in biological terms, if not always in social ones. The trend across the sample was to use a hybrid mixture of both ‘popular’ and ‘medically legitimated’ knowledge, to justify the purported immaturity. This understanding of the body and mind of adolescent females as ‘immature’ and not fit for reproductive purposes seems an apposite complement to the representation of youth as a period in which ‘to achieve’ accomplishments before a woman embarks on sexual and reproductive engagements, for which her body and mind would be ready only later on.
For a population that historically has had little control over their conditions of living, avoiding the risk of getting pregnant by appealing to social and biological reasons is proposed as a means of control over participants’ future. Youth is literally understood as a period for growth, thereby incorporating a more fluid identity removed from the indigenous stereotypes of unprogressiveness and ignorance.
Combining folk and established medicine
The third theme encompassed traditional medicine as opposed to those ideas and behaviours coming from academic and medical discourses, which the author terms ‘established’ medicine. Whereas providers of established health services were portrayed as holders of knowledge that participants endorse, they also referred to engagements with their cultural heritage by narrating the use of ‘folk’ medicine, comprising traditional, local and indigenous knowledge. These included beliefs and practices perceived as health enhancing: herbal remedies (menstrual cramp relievers, abortifacients and childbirth facilitators), massages (sobadas) by traditional midwives (parteras) and temazcal, a therapeutic bath practiced in Mesoamerican cultures. Participants communicated their use of folk medicine depending on their social setting.
Rural participants positioned themselves at the crossroads between folk and established medicine by acknowledging the legitimacy and effectiveness of both. Established medicine was seen as authoritative and sought after, while folk medicine was less expensive and more accessible. Rural participants emphasised that practical use of traditional knowledge was influenced by tangible material needs, rather than preference for one type of medicine: … [husband] told me to go to the hospital, but since we had no money for them to take me [there], then he said ‘better to call Mrs [partera’s name]’… (Rural, 16, one child) … my mum says that in the clinic they tell them not to drink those teas [to facilitate childbirth], but I remember that when my mum was about to give birth, she made her tea … she entered [the hospital], and about ten minutes later, my little brother was born. That’s why I say that it’s effective … (Rural, 18, no children)
Rural participants, as in the excerpts above, communicated the usefulness of both folk and established medicine by linking it to practical experience. One type of knowledge is drawn upon depending on the situation (e.g. inducing labour as opposed to the actual delivery) and resources (e.g. home attendance of ailments deemed to be financially and geographically accessible), in a selective prevalence process.
Urban participants, in contrast, recognised the need and practical use of both folk and established medicine, subtly favouring the latter in their dialogues:
3
When I was pregnant I went to have check-ups every month, every month Did you do anything else? Well yes, I went with a lady in [nearby neighbourhood] so that she <me la acomodara> [lit. to accommodate or adapt, meaning to put the foetus in an appropriate position] because she (baby) was across [the womb] […] Would you have gone with her? <¿A que me pasara mi parto?> [lit. to pass my delivery, meaning to give birth] No, because I don’t trust parteras, because there have been cases in which they don’t know how to cut the belly button, whereas in the hospital they put a catheter to clean them, to get all the blood out, they cut their belly button with special scissors made for that. (Urban, 16, one child)
Urban participants endorsed both kinds of medicine. However, they displayed a subtle alignment with established medicine that they associated with current times, enhanced quality of care and effectiveness. In this group, it is possible to observe how established medicine is inconspicuously displacing folk medicine approaches.
Discussion and concluding implications
This study examined sexual health knowledge among a diverse sample of indigenous Mexican young women. It sought to provide a nuanced view of their representations vis-à-vis those of their communities and elders and to test the framework of varieties of cognitive polyphasia for analysing potential knowledge transformations.
The most interesting finding of this study was the overall consistency of discursive themes. This suggests that transformations around the same issues are occurring across indigenous Mexican female adolescents of the same age group, notwithstanding the diversity of sexual and reproductive experiences and schooling of participants in both settings. The literature on identity has identified schooling, media and migration as triggers of identity changes among indigenous youth (Manago, 2012; Pérez Ruiz, 2011; Saraví et al., 2014; Urteaga, 2011). The work of health staff and indigenous/peasant NGOs can also account for impacts on the knowledge and values among the study sample. First, perspectives attributed to health staff were used to complement, contrast or contest those attributed to the community. Despite participants’ obstacles to access (e.g. established medicine lacks folk medicine’s perceived advantage of being inexpensive), health staff appear able to raise awareness among them. Perspectives ascribed to health staff came to the fore when giving biological explanations for which sexual and reproductive practices are healthy during adolescence, hybridising with those coming from the community and elders to discourage specific behaviours. Second, while very few participants were part of indigenous associations, some reported having participated or heard of NGO workshops and presentations on such topics as contraception, especially in the rural setting. In Mexico, NGO activities that aim to better the lives of indigenous and peasant women and youth have been found to be transformative for indigenous women (González Montes, 2007; Valladares de la Cruz, 2008). Hence, it is possible that local NGOs’ social development activities have diffused ideas that ‘challenge customs’ (González Montes, 2007) among participants.
This study provides evidence to substantiate structural conditions such as conservatism marked by shame, in this case intertwined with interiorised marginalisation, and hardship, as previously documented in the literature (Chopel, 2014; Gamlin, 2013). However, participants were acutely aware of these conditions and problematised them, thereby expressing their agency and willingness to transform their realities, in an ongoing process. Hardships are traits of previous generations that participants want to displace with better quality of life, whereas the conservative approach to sexual health is still selectively deployed depending on the situation, demonstrating that contextual traits undergo different levels of transformation.
Participants reported engagement with their communities’ network to understand what is socially and biologically healthy, in order to steer decisions to delay sexual activity, dovetailing with studies with marginalised youth in Latin America (Bayer et al., 2010; Gonçalves et al., 2011). Yet, a struggle between parents’ expectations and participants’ desires for open socialisation was identified, mainly for in-school participants (the majority located in the urban setting), demonstrating that participants drew on their parents’ knowledge while at times questioning it, in a selective prevalence process that accounted for the social dimension of youth. Regarding the biological dimension of youth, ‘medicalised’ and community sources were joined in a hybrid understanding of immaturity.
The plurality of participants’ engagements with both folk and established medicine indicates multidimensional rather than dichotomised understandings of folk and established medicine, which has also been reported among indigenous groups worldwide (Nettleton et al., 2007: 468). In many cases in the rural setting, favouring of one type of medicine over another was not a matter of preference but of financial barriers to access established healthcare services, in selective prevalence processes. In the urban setting, while participants still drew on both forms of knowledge, they subtly distanced themselves from the past, which they associate with folk medicine. It can be surmised that this is related to the geography of the city (more opportunities for mobility) and urban participants’ opportunities to engage with a wider set of ideas (Urteaga, 2011).
On the theoretical front, the typology of cognitive polyphasia proved to be a useful heuristic to identify knowledge interaction, highlighting the consistency of discursive themes across the sample, as well as the varied processes through which they are accrued. However, this classification can be improved in at least two ways. First, for the purposes of this article, the term ‘types of knowledge’ was used when categorising varieties of cognitive polyphasia, which contrasts with the ‘systems of knowledge’ proposed by Jovchelovitch and Priego-Hernández (2015). This is because, in order to map out systems of knowledge, it would be necessary to identify discrete epistemological assumptions behind each actor, voice or opinion. For instance, a cognitive style for science or religion would need to be delineated before relating it to any position (De-Graft Aikins, 2003). Using the more modest idea of ‘types of knowledge’, the typology can be grounded to any dialogue for analytical purposes so that, for example, youth, parents and educators might draw on the same scientific or religious system of knowledge to express nuanced positions within it, which also constitutes a form of cognitive polyphasia. Second, while this study focused on the perspectives of adolescents and their communities and elders, further studies might focus on a wider set of actors, gauging the applicability of this framework in multi-party dialogue (Marková, 2007).
These findings underscore three interrelated implications. First, they challenge the need to tailor ‘culturally specific’ health programmes to indigenous youth (Pedrero and Oyarce, 2011). A more productive approach might be to capitalise on transformations already occurring among these groups, which in this case appear to be aligning with Mexico’s nationwide health policies by promoting the delay of sexual and reproductive experiences and by consciously assessing the pertinence of established medicine. Second, the findings support the need for sex education to focus on information, interpersonal skills and values (Stone and Ingham, 2006). More needs to be done to engage with indigenous youth as resourceful agents and to understand what they value and consider healthy, which might be thematically homogeneous but conveyed through contradictory processes. These two implications indicate the need to account for the aspirations for personal realisation that participants displayed. In this regard, sexual health interventions should provide safe spaces for indigenous youth to reflect on how sexual and reproductive health decisions fit into their life projects and shape the accomplishment of their goals.
Third, this study has implications for professionals working with migrant indigenous youth and their families. The findings presented here evince that while health knowledge is ‘in transition’ among indigenous young females, it draws heavily on the ideas and values handed down by, and negotiated with, their elders and community. This, on one hand, complicates assumptions of immutable beliefs and insuperable problems (such as inconsistent healthcare-seeking behaviours and limited agency over health) frequently reported among these groups in the context of migration (e.g. Espinoza et al., 2014; Holmes, 2012). On the other hand, the findings indicate that young migrant (urban students) females engage in protective practices while ‘growing’, wherein they privilege sexual abstinence and focus on achieving academic goals as a means to overcome hardship. A suggested task for health practitioners working with multigenerational migrant families is to leverage these protective practices while opening up possibilities for discussing sexual health matters further (e.g. a focus on protected sex rather than exclusive abstinence, as well as the effectiveness of folk medicine).
The findings discussed in this article would benefit from juxtaposition with evidence from indigenous male youth, especially as research on sexual and reproductive health in Latin America has largely focused on indigenous women. This is arguably due to researchers’ assumption that these groups understand reproduction, contraception and childbearing as the exclusive remit of women. Similarly, longitudinal designs would help to map out knowledge transformations over time. These research directions should provide further evidence that while indigenous knowledge should not be romanticised, recognition of its plurality and continuous transformation is the first step towards aligning it to the objectives of any health intervention.
Footnotes
Acknowledgements
This work is dedicated to the participants of the study. The author is grateful to Professor Sandra Jovchelovitch and Dr Claudine Provencher for their support and to two anonymous reviewers for their insightful feedback on an earlier version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Mexican National Council for Science and Technology (CONACYT studentship 303574, registry 205782). The author also received support from the Mexican Secretariat of Public Education, the Juarez Autonomous University of Tabasco, Mexico, and the LSE Department of Social Psychology.