
Abstract
The Injustice Experience Questionnaire has shown promising ability to predict problematic rehabilitation in pain conditions, especially concerning work status. A Danish language version of the Injustice Experience Questionnaire was developed and completed by 358 patients with long-lasting pain/somatoform symptoms. These patients also completed questionnaires concerning sociodemographics, anxiety and depression, subjective well-being, and overall physical and mental functioning. Our results showed satisfactory interpretability and face validity, and high internal consistency (Cronbach’s alpha = .90). The original one-factor structure was confirmed, but subscales should be interpreted cautiously. The Danish version of the Injustice Experience Questionnaire is found to be valid and reliable.
Introduction
Perceived injustice (PI) is frequently a dominant psychological element in patients with prolonged or chronic symptoms, such as chronic pain and medically unexplained syndromes. Such patients have often experienced their symptoms for many years, sometimes after a sudden onset due to injury, trauma, or a failed operation. Over this time, they may have suffered multiple losses—for example, their job, income, social status, sense of identity, and friends—and frequently feel both grief and anger relating to these losses (Harris et al., 2003). Many of these patients find themselves preoccupied with issues of justice and fairness (McParland et al., 2011). Qualitative studies further show that many patients feel that they have been misunderstood and stigmatized, which increase feelings of anger and perceptions of injustice (Holloway et al., 2007). It has been suggested that strong feelings of PI may independently influence the possible recovery in these patients (Sullivan et al., 2008).
To investigate the role of PI in patients with chronic pain and disability, Sullivan developed the Injustice Experience Questionnaire (IEQ) in 2008 (Sullivan et al., 2008). The IEQ assesses the degree to which individuals perceive their post-injury life as being characterized by injustice, and offers promising new perspectives for better understanding psychological aspects of pain conditions. Sullivan and colleagues report that PI may represent a risk factor for poor recovery outcomes, particularly regarding measures of physical function and return to work, and it is established that the IEQ has predictive value regarding problematic rehabilitation outcomes (Sullivan et al., 2012). Further studies indicate that high levels of PI are associated with more intense pain, and higher levels of catastrophic thinking, depression, and disability (Scott and Sullivan, 2012; Sullivan et al., 2009a).
The IEQ questionnaire includes two inter-correlated factors that comprise six items each and are labeled “severity/irreparability” and “blame/unfairness.” In the original study, the IEQ had a Cronbach’s alpha of .92 and a test-retest reliability of .90 (Sullivan et al., 2008). The scale has been translated into Spanish and validated, showing a Cronbach’s alpha of .89 and a test-retest intraclass correlation of .98 (Rodero et al., 2010). Thus, the IEQ represents a promising tool for better understanding of feelings of injustice and development of better targeted interventions.
Until now, there has been no Danish version. This study aimed to describe the development, content validation, and psychometric validation of the Danish language version of the IEQ. We investigated whether the Danish version has comparable psychometric properties to the English and Spanish versions.
Methods
Setting and sample
The participant sample comprised 358 individuals with either a diagnosis of chronic benign pain or a “somatoform” diagnosis (predominantly a somatoform pain disorder, ICD10 F45–48). All participants had been referred for assessment and treatment at either the Crossdisciplinary Pain Center, Rigshospitalet (N = 162) or the Liaison Clinic, Mental Health Center (N = 196), which are both multidisciplinary clinics in Copenhagen, Denmark. Upon referral, patients at each clinic were asked to complete several commonly used questionnaires, including information on sociodemographic data and a paper-and-pencil Danish version of the IEQ. The participants were not financially compensated for this, nor did questionnaire completion have any impact on their further assessment or treatment at the clinics. Data were collected in 2014, between 1 January and 31 December. Data collection was performed in accordance with the guidelines for the Danish national scientific ethics committee, and the database was approved by the national Danish Data Protection Agency.
Measurement tools
Sociodemographic information
The collected sociodemographic data included age, gender, marital status, number of children, educational level, current employment status, and duration of symptoms.
PI
The IEQ assesses the degree to which individuals perceive their present condition as being characterized by injustice. Respondents rate their experiences of 12 different thoughts/emotions/attitudes described in the questionnaire items, using a 5-point Likert scale ranging from 0 meaning “not at all” to 4 meaning “all the time” (Sullivan et al., 2008). The final score is the sum of all items, with high values indicating high PI levels. PI was originally defined as a cognitive appraisal of severity (item example, “Most people don’t understand how severe my condition is”), blame (item example, “I am suffering because of someone else’s negligence”), unfairness (item example, “It all seems so unfair”), and loss (item example, “My life will never be the same”) related to the condition.
A cut-off score of 30 was initially suggested to indicate clinically relevant cases of PI (Sullivan et al., 2008). A later study showed that a cut-off score of 19 is optimal for predicting employment status at 1-year follow-up (Scott et al., 2013b).
Depression and anxiety
The Hospital Anxiety and Depression Scale (HADS) is a 14-item anxiety and depression screening instrument for use in non-psychiatric patients (Zigmond and Snaith, 1983). It has been validated and found reliable for use in the Danish general population (Bjelland et al., 2002), as well as in patients with chronic pain (Härter et al., 2001; Pallant and Bailey, 2005). Scores range from 0–21 for both measures, with higher scores indicating greater anxiety and depression. The average Cronbach’s alphas are reported as .83 for anxiety and .82 for depression (Bjelland et al., 2002).
Subjective well-being
The World Health Organization’s well-being scale, WHO-5, is a well-being index including five items concerning feelings of positive mood, vitality, and general interest. It is answered using a five-point Likert scale, with higher scores indicating higher well-being. The scores are added and multiplied by four, giving a final score ranging from 0–100. The Danish language version of this scale has been validated (Bech et al., 2003).
Overall functioning measure
The Short Form Health Survey-36 (SF-36) is a standardized, well-validated, multi-dimensional questionnaire that measures health, level of function, and well-being in eight dimensions (Ware and Gandek, 1994). The Danish language version has been validated and found to be reliable (Bjorner et al., 1998). The dimension Physical function is measured using 10 items concerning physical disabilities. Role physical is addressed by four items regarding present physical limitations. Bodily pain is evaluated based on two items about pain and impact of pain. General health is assessed using five items concerning self-rated health perception. The scores on these first four dimensions are used to calculate an overall Physical health component. The dimension, Vitality, is measured with four items concerning feelings of energy and tiredness. Social functioning is assessed using two items about social limitations. Role emotional is measured using three items about daily limitations for emotional reasons. Finally, Mental health is addressed in five items concerning present mood and nervousness. The scores for these last four dimensions are used to compute an overall Mental health component. All SF-36 scores range from 0–100, with higher scores indicating better function on the specific dimension. Population studies usually show norms of around 50 for the two-component sum scores (Ware et al., 1995).
Validation process
Translation
We obtained permission from Michael Sullivan to process the Danish translation. First, the English version was translated to Danish by five people with mixed health and communication backgrounds. All five versions were compared and discussed at a meeting, and a version was agreed upon. This initial version was then presented to a native English speaker who was also fluent in Danish for back-translation. At the second meeting, the back-translated version was compared with the original English version, and the Danish version was fine-tuned using this new information. A second version was agreed upon, and was used for a face validity investigation including six patients with chronic pain and seven patients with somatoform disease. All patients completed the total set of questionnaires, and were then interviewed regarding any difficulty in understanding, any double meanings in items, and whether the questions related to things that they knew from their own lives. The responses were positive. We made small changes to the layout, but no item wording was changed at this stage. The authors then agreed on the final version.
Analytical strategy
Due to the nature of the material, it was not possible to perform a test-retest procedure for reliability. We did not consider this a major problem since very high test-retest correlations are reported for the English and Spanish versions of the IEQ. Internal consistency was evaluated using Cronbach’s alpha and distribution statistics. The internal structure was evaluated using factor analysis. Construct validity analysis is an assessment of the association between the questionnaire and other measures of related variables or dimensions. We anticipated that low IEQ scores would correlate with better mental health functions, higher well-being, and higher scores on the SF-36 dimensions. Interpretability and face validity of the IEQ were tested during development of the translation.
Statistics
All data handling and statistical analyses were completed using SPSS 21 with standard settings, and the level of significance set at p < .05. Missing data were treated as missing. Only completed questionnaires were included in the sum score computations (completer’s analysis) (N = 316). The factorial structure of the IEQ was investigated using Principal Component Analysis, with a Varimax rotation applied to utilize a clear factor structure. Spearman correlations were used to investigate relationships between IEQ and the sociodemographic data, Pearson correlations for relationships between IEQ and the continuous data variables.
Results
As shown in Table 1, most patients suffered from pain conditions lasting several years. One-third of the patients were medicated with opioids. A slight majority of patients were female, and less than one-third of patients held a current job.
Patient characteristics (N = 358).
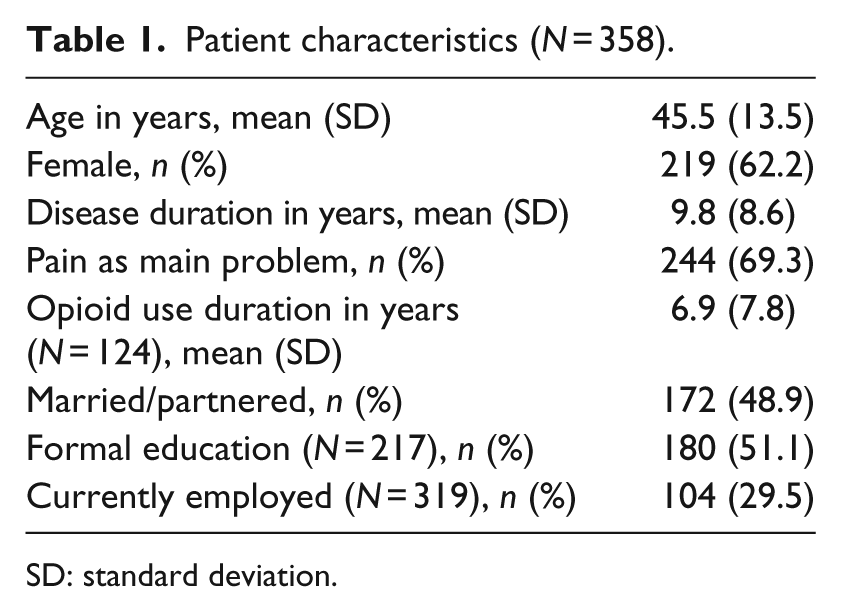
SD: standard deviation.
Table 2 presents basic data regarding the utilized Danish measurement tools. All continuous variables were tested for normal distribution using the Kolmogorov–Smirnov test and via inspection of frequency (histogram) plots and Q-Q plots.
Danish measurement tools.
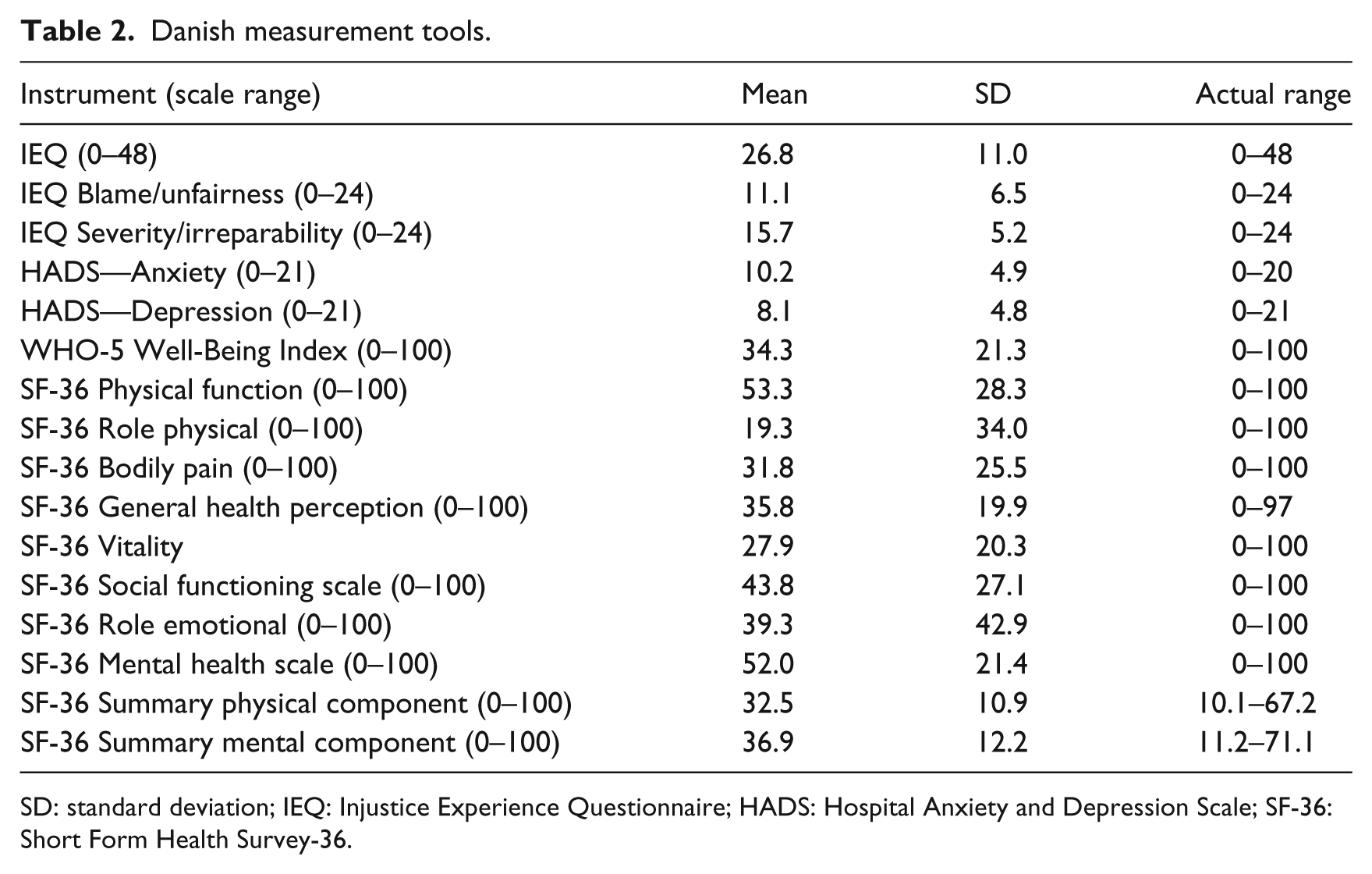
SD: standard deviation; IEQ: Injustice Experience Questionnaire; HADS: Hospital Anxiety and Depression Scale; SF-36: Short Form Health Survey-36.
Table 3 shows the internal consistency of the IEQ. Item analysis inspection shows that no item behaved in a statistically unexpected manner.
IEQ score analysis.
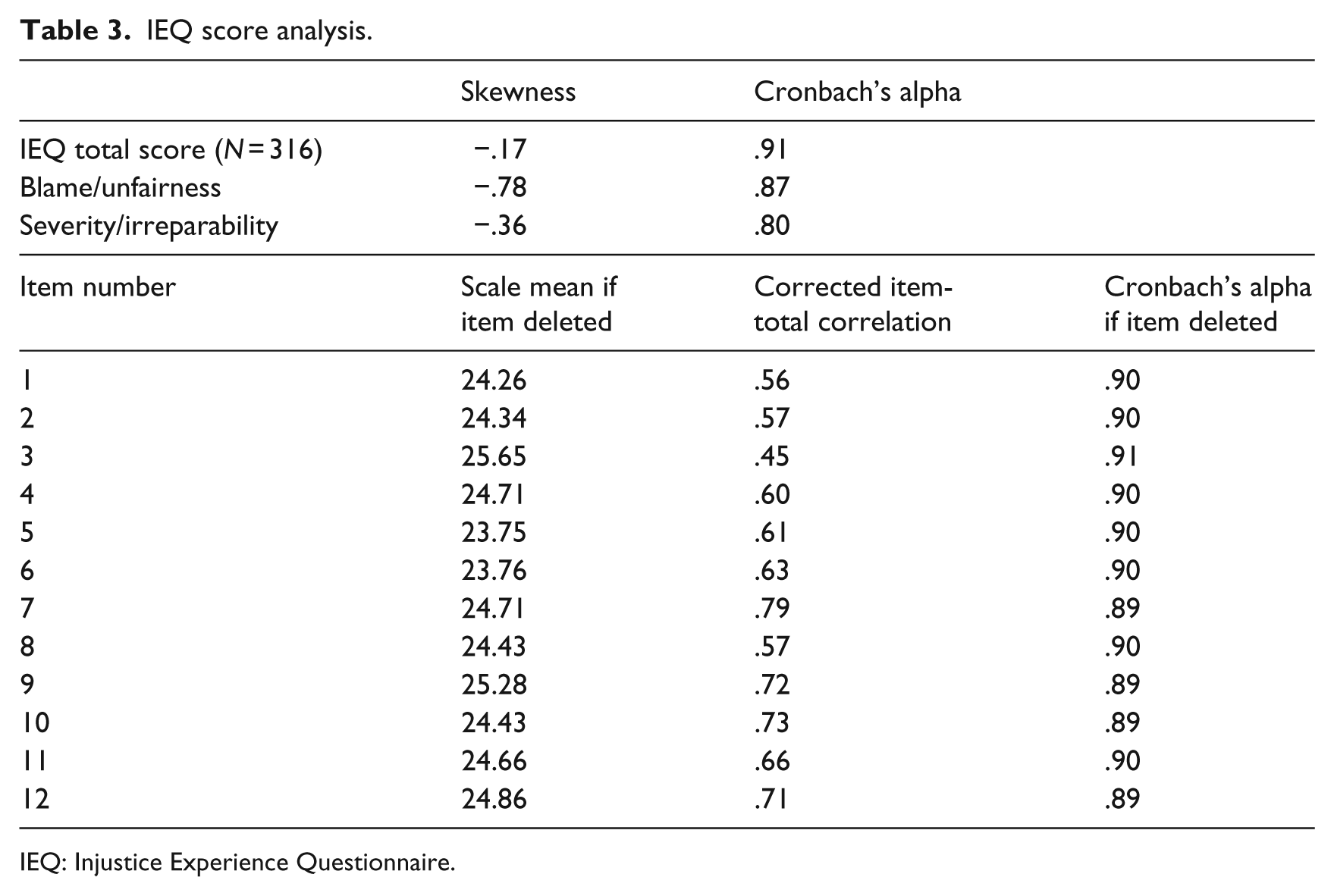
IEQ: Injustice Experience Questionnaire.
The Kaiser–Meyer–Olkin measurement of sampling adequacy was .91, and Bartlett’s test of sphericity showed highly significant results (p < .0001), which allowed for a factor analysis. Two factors had an eigenvalue of >1. The first had an eigenvalue of 6.0, explaining 49.7 percent of the variance. The second factor had an eigenvalue of 1.02, explaining 8.5 percent of the variance. Inspection of the Scree plot (Figure 1) supported the one-factor structure of the IEQ.
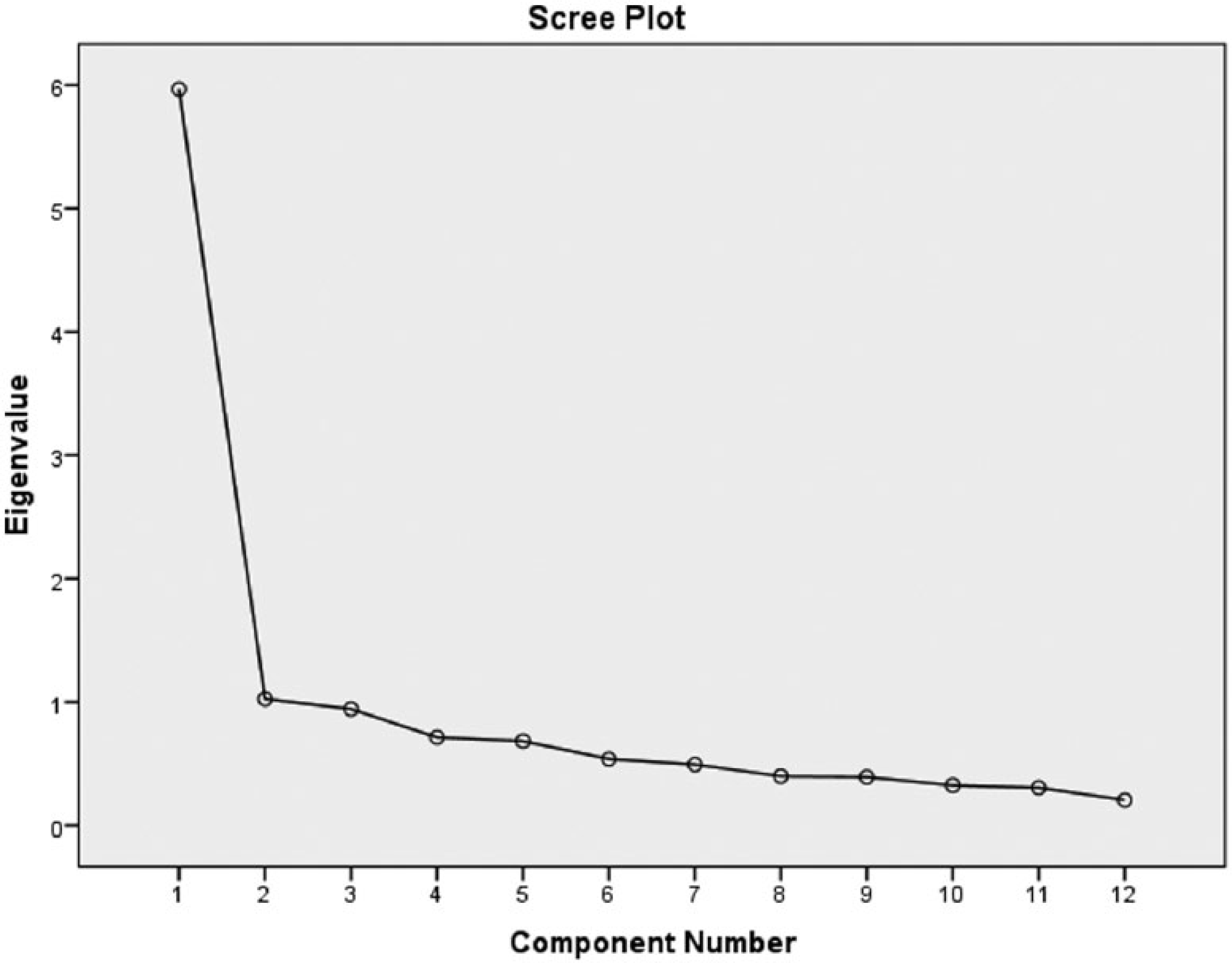
Scree plot of the factorial structure of the Danish IEQ.
When the IEQ was forced into a two-factor structure and a Varimax rotated solution was applied, the items did not fully agree with the distribution of the English version. Following division into the blame/unfairness and severity/irreparability subscales, two items were in a different group compared with the English original version—with item 3 grouped under severity/irreparability while item 5 grouped under blame/unfairness. Analysis of the item contents did not justify this change of structure.
Table 4 shows correlations between IEQ and sociodemographic data. Notably, all correlations were very small. The only significant correlation was that between current unemployed status and IEQ total score (as well as the blame/unfairness subscore).
Correlations of IEQ with sociodemographic data.
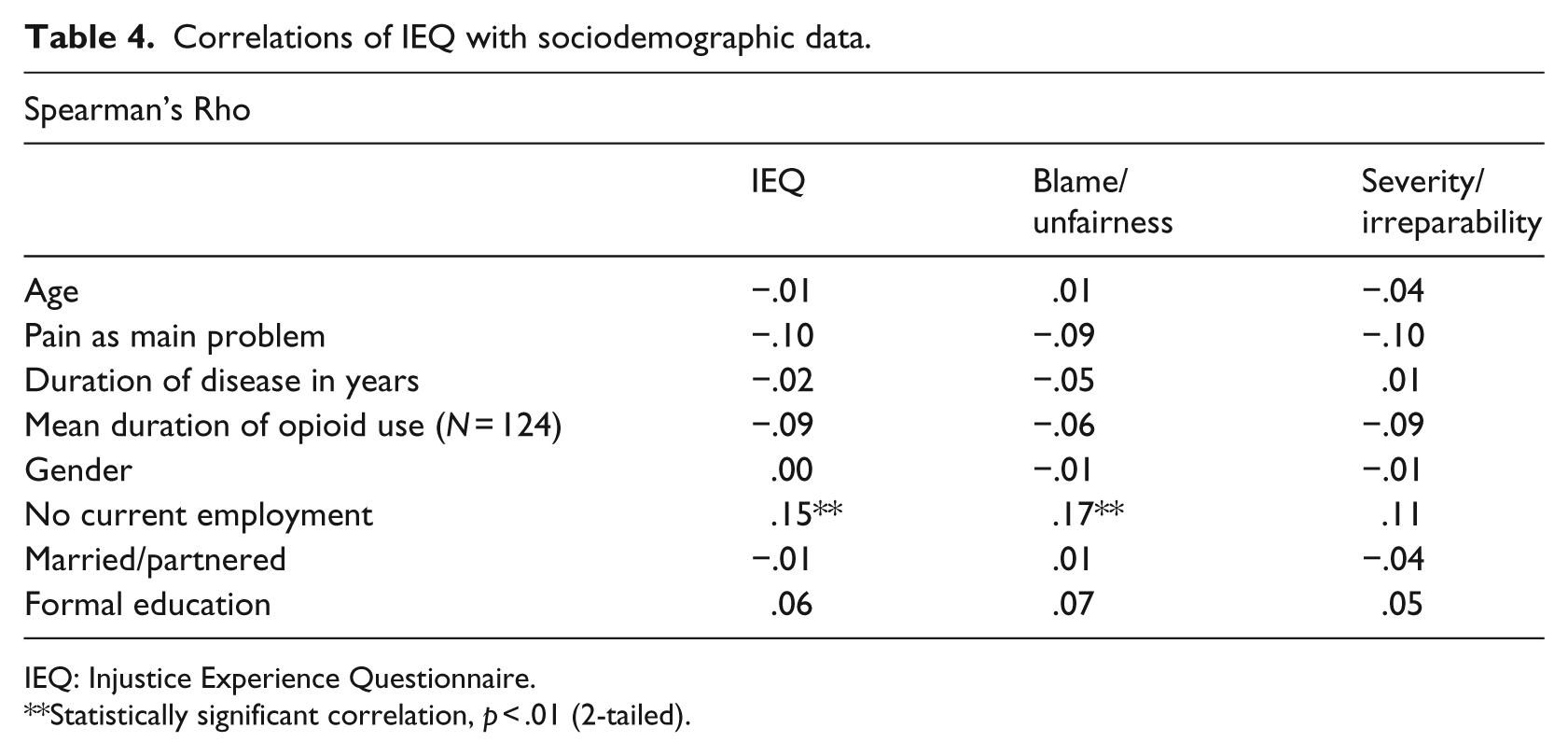
IEQ: Injustice Experience Questionnaire.
Statistically significant correlation, p < .01 (2-tailed).
Construct validity was analyzed by investigating correlations between the IEQ and the other continuous variables, as seen in Table 5. As anticipated, high PI levels were positively correlated with high anxiety and depression scores, and were significantly negatively correlated with good health and well-being. Notably, the negative correlations were highest with the mental subscales of SF-36, but all scores were also negatively correlated with the physical subscales of SF-36. PI was also found to be moderately negatively correlated with both Bodily pain and General health perception, indicating a relationship between feelings of injustice and high levels of symptoms.
Construct validity: Pearson correlations between the IEQ and measures of anxiety, depression, well-being, and health-related quality of life.
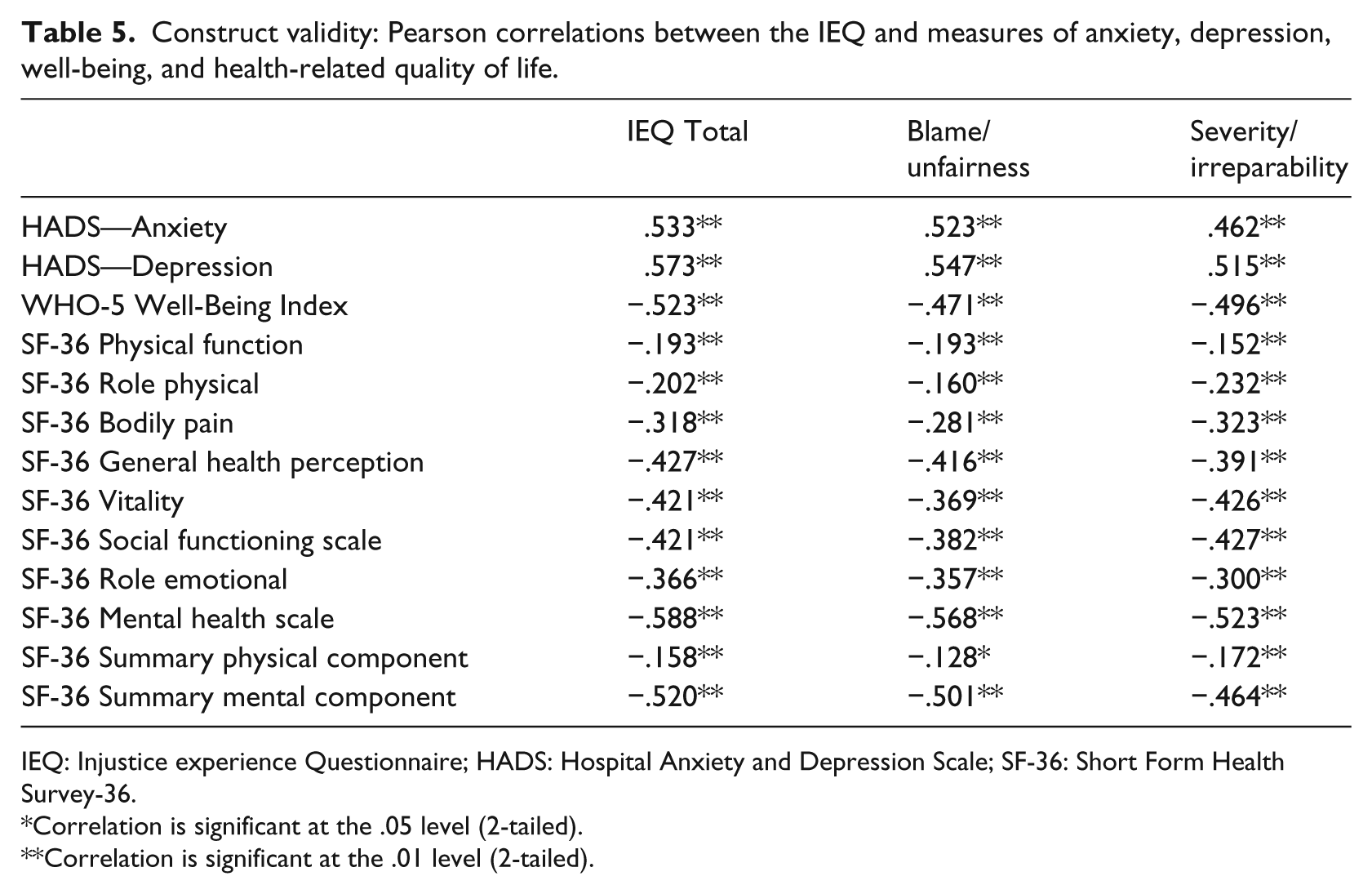
IEQ: Injustice experience Questionnaire; HADS: Hospital Anxiety and Depression Scale; SF-36: Short Form Health Survey-36.
Correlation is significant at the .05 level (2-tailed).
Correlation is significant at the .01 level (2-tailed).
Discussion
Our results validated the Danish version of the IEQ in several ways. Interpretability and face validity were tested by interviews and found to be well accepted in the target population. The internal consistency was high, with normal distribution of scores and a Cronbach’s alpha of .90. Item analysis revealed no outlier items. Internal structure analysis verified a one-factor structure, and the construct validity was confirmed by hypothesized correlations with related questionnaires.
Compared with the blame/unfairness and severity/irreparability subscales of the original English version (4), in the Danish version, two items showed higher loadings with a different subscale (4). Similarly, in the Spanish validation study (Rodero et al., 2010), all items did not fit into the predefined subgroups, although the item deviations were not the same in the Danish and Spanish language versions. It is possible that the subgrouping of other versions of the scale will not be consistent with the English version.
Concerning the sociodemographic data, we identified only one significant (but low) correlation; it was between being unemployed and the IEQ score. This finding supports previously observed links between PI and a lack of work rehabilitation (Scott et al., 2013b; Sullivan et al., 2008, 2009b). Aside from the IEQ, work life has been the major focus of the literature concerning PI. Baron (Baron et al., 1999) found that PI correlates with covert workplace aggression, Cohen-Charash (Cohen-Charash and Mueller, 2007) found perceived unfairness to predict interpersonal counterproductive work behavior, and Francis (Francis and Barling, 2005) reported a relationship between PI and a higher degree of job strain. Howard (Howard and Cordes, 2010) observed that PI is related to emotional exhaustion and employee withdrawal. It remains unknown why experiences of injustice are so tightly connected to negative work-life events. One possibility is that work-life may be a sensitive social area with high social exchange, thus representing a possible area to act out feelings of anger by behaving aggressively toward others or to simply withdraw or stay away from. Another possibility is that pain levels can be mediated through anger. Anger is reportedly a main mediator between PI and pain intensity and between PI and depression (Scott et al., 2013a). Therefore, the negative link between PI and work could also exist because PI represents a mental mirror of a long period with pain and impairment. In this case, high PI would simply reflect and be caused by higher pain intensity, which could be the reason for work rehabilitation failure.
This discussion of “the chicken and the egg” seems to have empirical support on both sides. Concerning fibromyalgia, Rodero (Rodero et al., 2010) found that PI predicts “global functioning” even controlling for pain intensity, pain catastrophizing, and pain acceptance. Additionally, in a sample of patients undergoing knee arthroplasty, PI modestly predicted postsurgical pain even after controlling for other relevant variables. On the other hand, a recent investigation suggested that PI only closely mirrors pain, showing that initial differences in PI among patients with rheumatoid arthritis and whiplash disappeared completely when results were controlled for pain intensity (Ferrari, 2014b). A prospective study of whiplash victims demonstrated that PI was low just after the accident, and stayed low for all patients after 3 months, with IEQ scores only changing among the non-recovered victims between 3 months and 6 months after the accident (Ferrari, 2014a).
Our results also revealed a weak but significant correlation between level of physical symptoms (inclusive pain) and IEQ scores. However, due to the nature of our cross-sectional study, no conclusions can be drawn regarding causation. It cannot be determined whether high pain leads to high PI or if high PI causes high symptom level and pain. This important question may be a target for future research. It might also be possible that pain and PI mutually aggravate each other in a vicious circle.
Our study has several limitations. We had no information available about the patients who did not answer the questionnaires. However, as this was a validation study, we considered this to be only a minor problem. As mentioned, we also lacked a test-retest procedure to examine the reliability of the Danish language version of the IEQ. However, given the high test-retest correlations from the English and Spanish validations (Rodero et al., 2010; Sullivan et al., 2008), we have no reason to assume that there would be a problem regarding the Danish version.
In conclusion, our results indicate that the Danish version of the IEQ is valid and reliable. However, we suggest caution in the interpretation in the suggested subscales.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.