
Abstract
Social Cognitive Theory has been used to explain findings derived from focus group discussions (N = 4) held in the United Kingdom with the aim of informing best practice in personalised nutrition. Positive expectancies included weight loss and negative expectancies surrounded on-line security. Monitoring and feedback were crucial to goal setting and progress. Coaching by the service provider, family and friends was deemed important for self-efficacy. Paying for personalised nutrition symbolised commitment to behaviour change. The social context of eating, however, was perceived a problem and should be considered when designing personalised diets. Social Cognitive Theory could provide an effective framework through which to deliver personalised nutrition.
Introduction
Nutrigenomics is the study of how gene expression is altered or determined by foods and/or food constituents (Hendriks, 2013), the application of which is the delivery of dietary advice based on individual genetics (Ronteltap and Van Trijp, 2007). Personalised nutrition is healthy eating advice that is tailored to suit an individual based not only on genetic data but also on personal health status, lifestyle, nutrient intake and phenotypic data (Gibney and Walsh, 2013). While direct-to-consumer (D-T-C) genetic testing has been available via the Internet for some time, personalised nutrition is relatively recent (Annas and Elias, 2014).
A substantial body of qualitative research has investigated the general public’s willingness to accept genetic testing (see Stewart-Knox et al., 2015 for a review). Relatively few qualitative studies, however, have considered personalised nutrition. Qualitative research into personalised nutrition has been conducted in Canada (Morin, 2009) and, more recently, in Europe (Fallaize et al., 2015; Stewart-Knox et al., 2013). These studies have shown that although positive about personalised nutrition and cognisant of the benefits, there are diverse preferences for how services should be delivered and reservations about the service provider’s ability to protect personal data. Although such studies have provided an insight into what the public requires from personalised nutrition, there remains a need for further qualitative analysis to explore and improve our understanding of how to inform best practice for the provision of personalised nutrition.
Social Cognitive Theory (SCT) comprises several psychological constructs which are thought to interact with personal, behavioural and environmental factors to bring about behaviour change (Bandura, 1977, 1982, 1997). SCT postulates that outcome expectancies, the beliefs surrounding the consequences of initiated actions, are explained by intention to act out the behaviour (e.g. healthy eating), which are underpinned by the perceived risks and benefits associated with behaviour change (Bandura, 2004). Self-regulation is the perceived ability to control actions through goal setting, self-monitoring, feedback, self-reward, self-instruction and social support (Bandura, 1997; McAlister et al., 2008). Such factors are likely to interplay in response to personalised nutrition intervention. Self-efficacy, which is the belief in one’s capabilities to learn or perform actions involved in behaviour change, can be enhanced by the learning of new behaviours either through direct experience or, vicariously, through observation and modelling of others’ behaviour (Bandura, 1997). Environmental factors are those which are external to the individual, both physical and social, and which may affect behaviour (Glanz et al., 2002). We would hypothesise that some of these factors may inform an individual’s perceptions surrounding personalised nutrition and propensity for dietary behaviour change.
The purpose of this analysis has been to develop theory with which to inform best practice in the delivery of personalised nutrition. Most research that has applied SCT to the understanding of dietary health behaviour change has been quantitative (Guillaumie et al., 2010; Nixon et al., 2012; Stacey et al., 2014). This research in contrast has adopted a qualitative ‘bottom up’ approach in which SCT has been employed as a conceptual framework with which to understand perceived determinants of and compliance with personalised nutrition and successful dietary behaviour change, and which are likely to have implications for effective service delivery.
Methods
Ethical approval was granted by the Research Ethics Committee of Ulster University and Newcastle University, United Kingdom.
Two novel data sets (Newcastle and Belfast), which were conducted as initial pilot studies for the Food4Me qualitative enquiry into public perceptions of personalised nutrition, have been used for this analysis. These data are unique in that they were collected at a different time (6 months + prior) to the previously published studies (Fallaize et al., 2015; Stewart-Knox et al., 2013) and as such they were exploratory for the purpose of designing the methods used in subsequent qualitative and quantitative studies and for the development of theory to achieve behaviour change in response to personalised nutrition intervention. These studies have provided data sufficient to explore new theoretical questions (Heaton, 2004).
Sampling
Study participants were recruited through social research agencies in the United Kingdom (Belfast and Newcastle-Upon-Tyne). Those who reported ill health, learning disabilities or being a health professional were excluded. Participants were also excluded if they had a background in food and nutrition or were individuals who had previously taken part in research related to nutrition. Two focus groups were held in each region (Belfast and Newcastle Upon-Tyne). Each focus group comprised eight discussants both male and female of mixed age (Table 1).
Focus group – sample description.
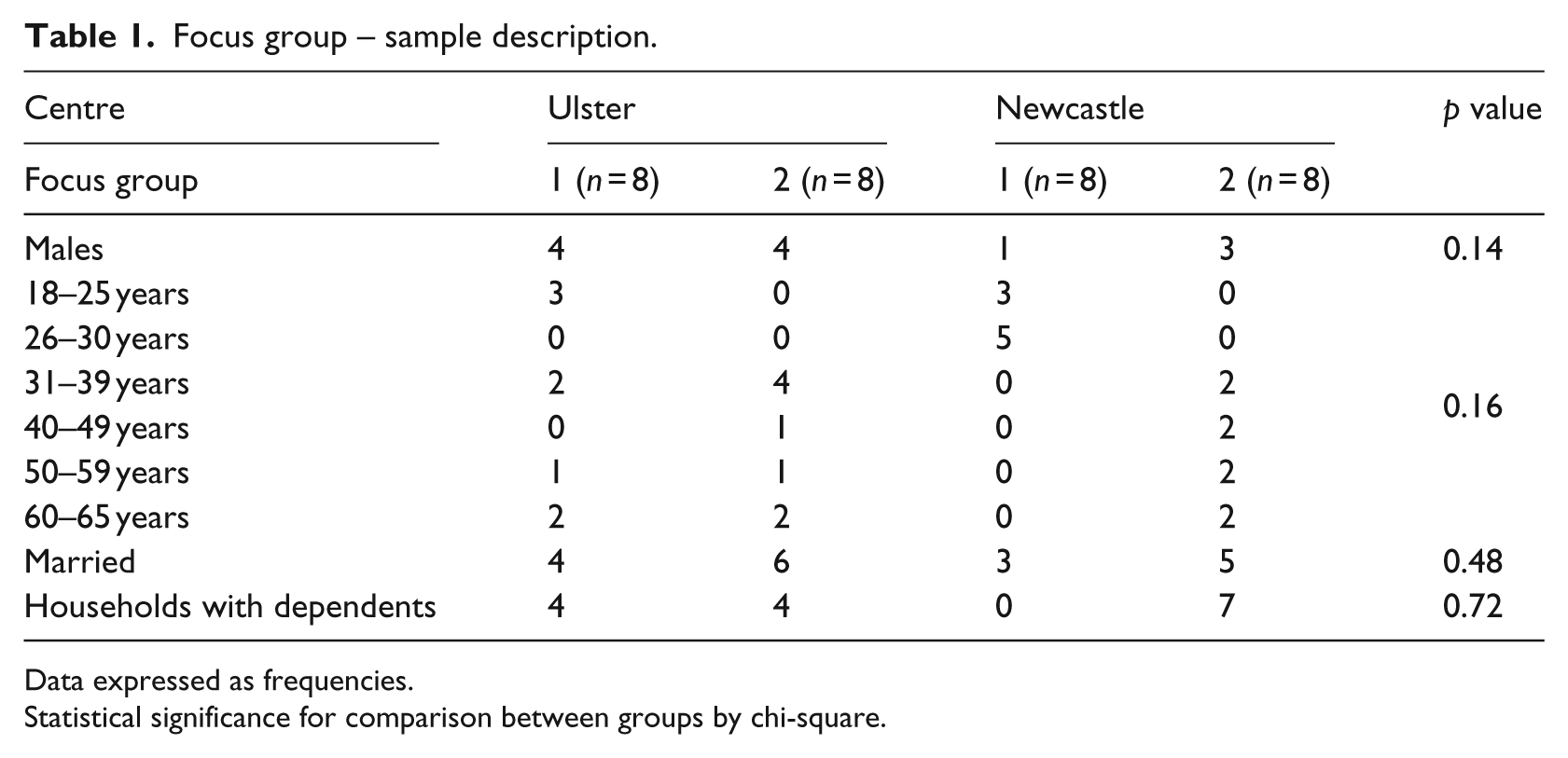
Data expressed as frequencies.
Statistical significance for comparison between groups by chi-square.
Materials
Discussions followed a standardised protocol (Table 2) which aimed to generate responses on how best to implement personalised nutrition in practice to achieve dietary behaviour change. Discussion was prompted by scenarios depicting personalised nutrition based on three successive levels of ‘medicalisation’: dietary and lifestyle; phenotypic; or, genotypic. Each scenario was displayed on an illustrated prompt board. The Food4Me definition ‘Personalised nutrition is healthy eating advice that is tailored to suit an individual based on their own personal health status, lifestyle and/or genetics’ was also displayed throughout the discussion. Research materials related to this study can be accessed through the Food4Me website (http://www.food4me.org/) or requested from the corresponding author.
Focus group schedule.
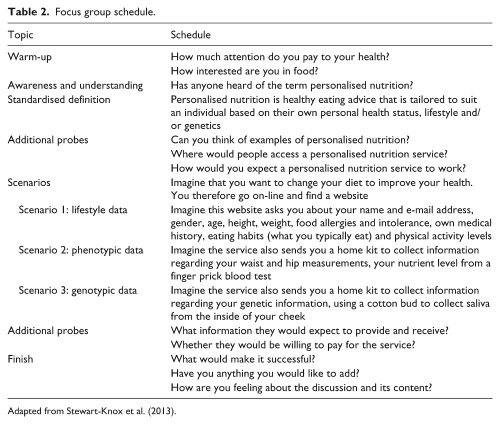
Adapted from Stewart-Knox et al. (2013).
Procedure
After reading the participant information sheet, volunteers signed consent forms and completed a demographic profile questionnaire. Each discussion lasted between 1 and 1.5 hours and was audio-recorded. Focus groups were led by a trained moderator, with an observer present to document the order in which discussants spoke (to aid transcription) and to record any other pertinent observations.
Data analysis
Discussions were transcribed verbatim and anonymised. NVivo (Qualitative data analysis software, QSR International Pty Ltd Version 9, 2012) was used for data storage and retrieval.
Data were analysed using thematic content analysis to capture their richness. The first stage in the coding process involved the systematic reading and re-reading of each transcript enabling the analysts to become immersed in data. This first stage of data recontextualisation (Bishop, 2007; Moore, 2007) was followed by the inductive coding of themes. The third stage involved analysing and interpreting the themes in relation to the underlying determinants of intention to adopt personalised nutrition. To assure consistency, the analysis was conducted only for recurrent themes (and not isolated remarks), which occurred in all transcripts. Finally, to assure rigour, consistency and reliability of the coding and analysis, a second author checked the transcripts, against the coding framework, to confirm the selected quotes provided a coherent description of the underlying constructs, after which any discrepancies were discussed and amended as necessary. Themes were then re-visited for theoretical implications and subsequently fitted to elements of SCT using a hybrid approach involving both inductive and deductive or theoretical coding (see Boyatzis, 1998). An a priori coding framework used the core constructs of SCT (i.e. positive and negative outcome expectancies, self-regulation, self-efficacy and environmental factors) (Bandura, 1977).
Results
Main themes identified through thematic content analysis suggested that the perceived benefits of personalised nutrition were immense and would encourage uptake (Stewart-Knox et al., 2013). Ability to follow personalised nutrition advice, however, was considered a function of individual motivation, willpower and commitment to the dietary regime. The theoretic analysis which follows, therefore, has sought to tease out the motivational factors perceived important to the adoption of personalised nutrition and to effective response, dietary change. Initial themes arising from these data suggested that effective personalised intervention should incorporate elements of SCT associated with goal setting (such as a target weight or fitness goal) and self-regulation (ability to control personalised nutrition through individualised feedback and monitoring). The social and physical environments were also considered important for potential personalised nutrition service providers to consider.
Outcome expectancies of personalised nutrition
Positive outcome expectancies
SCT postulates that outcome expectancies, the beliefs surrounding the consequences of initiated actions, are explained by intention, for example, to adopt personalised nutrition, and underpinned by the perceived risks and benefits associated with behaviour change (Bandura, 2004). Positive outcomes (benefits) attributed to personalised nutrition included to lose weight:
I suppose if you weigh yourself and you ended up being a wee bit heavier than what you want to be, that’d be a trigger. (FG1, Ulster, Male, 31–39 years) Well if it was a magical cure and I was gonna lose weight or do something like that I mean. (FG2, Newcastle, Female, 31–39 years)
Negative outcome expectancies
There was the notion that personalised nutrition was unlikely to provide results over and above that of the generic, public health approach to dietary health promotion. Respondents alluded to basic health promotion guidelines which were considered ‘standard’ and freely available on the Internet:
Y’know quite a bit of these things in terms of healthy lifestyle, you know you could write the things down now, they’re bog standard. (FG1, Ulster, Male, 60–65 years) Your eat well plate and all that sort of stuff tells you, you should eat a balanced diet and what you should have, what you shouldn’t. (FG2, Newcastle, Female, 31–39 years)
As discussion progressed through the levels of personalised nutrition (lifestyle and dietary data, blood sample, saliva sample), it became clear that participants held negative outcome expectancies associated with risk associated with lack of data protection and potential selling of data to other agencies and companies:
I’d just worry if its government, y’know the NHS government then they might share it with other government agencies, y’know the police, crime. (FG1, Ulster, Male, 31–39 years) The other thing as well, I can’t imagine why you would ever need to put your name and your email address in. That just screams to me that they’ll want to contact you or sell you something … (FG2, Newcastle, Male, 31–39 years)
Discussion centred on ways in which positive outcome expectancies could be brought about and negative expectancies expelled. Among suggestions for establishing the authenticity of the provider was to show organisational logos/emblems. A guarantee that all personal and health-related information supplied would be protected would also be required:
You’re probably more likely (to avail of a personalised nutrition service) if you see an emblem that you recognise. (FG1, Ulster, Female, 31–39 years) I would want a guarantee that at no time in 30 year time down the line my information’s gonna end up somewhere else and unless them could give me a cast iron guarantee that I trusted I couldn’t go with it. It would have to be cast iron. (FG2, Newcastle, Male, 31–39 years)
Self-regulation of behaviour
SCT holds that self-regulation of behaviour can be achieved by setting of goals (outcomes), personal coaching through self-instruction, self-monitoring, self-reward, support from peers and feedback (Bandura, 1997). Being able to monitor progression through setting of goals and feedback provided through an on-line interactive account were considered among ways that personalised nutrition could potentially affect behaviour change. It was deemed important to be able to make decisions with regard to which level of personalised nutrition was used and then for the user to have goals followed by feedback on the attainment of such goals. Without relevant and individualised feedback, the user could experience difficulty in self-monitoring their dietary health behaviour.
Goal setting
According to SCT, goal setting (short-term or long-term objectives) is linked to successful behaviour change (Bandura, 1997). Discussants were aware that a personalised eating plan would be more effective if they had a specific goal or target to work towards such as fitness and sports performance:
If it’s for your own goals, like if you’re sports person and you’re saying right I’m looking to bulk become a rugby player or something like that. (FG2, Ulster, Male, 40–49 years) If you wanted to get serious and you wanted to concentrate on losing weight and toning and things. (FG1, Newcastle, Female, 26–30 years)
Self-monitoring and feedback
Self-monitoring according to SCT involves reflecting upon progress and performance and is essential for the setting and re-setting of goals (McAlister et al., 2008). Feedback is important for self-monitoring (McAlister et al., 2008). Discussants agreed that feedback (e.g. progress reports), both on-line and in person, throughout the personalised nutrition process, would assist in self-monitoring and in achieving dietary behaviour change:
I think it depends if it was an on-going thing and it was something people were tracking your progress or you want to track your own progress on-line and constant. (FG1, Ulster, Male, 18–25 years)
Intrinsic feedback such as ‘feeling better’ was also considered important to implementing the tasks involved in personalised nutrition:
If you’re feeling a bit rough and you change your diet and all of a sudden you feel a little bit better, well that’s helped me. (FG2, Newcastle, Male, 60–65 years)
Self-efficacy for behaviour change
Self-efficacy, the belief in one’s personal ability to successfully conduct tasks or effect behaviour changes, is important in bringing about expected outcomes (Bandura, 1997). According to SCT, those with lower self-efficacy would be less likely to consider the outcome or goal as achievable. As the statements below indicate, self-efficacy was considered important to dietary change and was perceived to impact upon perseverance in pursuit of dietary goals:
The backbone, the willingness to stick to it. (FG1, Ulster, Male, 60–65 years) You’d be able to follow, you know, maybe for so long and then you’d just go crazy and then undo it all wouldn’t you? (FG2, Newcastle, Female, 40–45 years)
Enhancing self-efficacy
Self-efficacy is linked not only to perceived ability to make changes but also to commitment to behaviour change (Bandura,1991, 2004). Indi-viduals who are committed to behaviour change are more likely to set goals and, if efficacious, to achieve them. In keeping with SCT, therefore, discussants perceived that personalised nutrition would require commitment. Paying for personalised nutrition appeared to symbolise commitment and some indicated that they would be more compliant if paying for the service:
Well the only thing is if you’re paying for it, you’ll stick with it. There’s more incentive to stick to it. (FG1, Ulster, Male, 60–65 years) It’s all about willpower. You can’t have as much as you want but if you’re not going to have the willpower to do it then you’ve just wasted your time, my time and a lot of money, so yeah. (FG1, Newcastle, Female, 18–25 years)
Environmental factors and uptake of personalised nutrition
Environmental factors are those which are external to the person, both physical and social, which may interact to affect behaviour change (Glanz et al., 2002). While considering changes that could be made to the environment (e.g. the service interface and personnel), it was suggested that a personalised nutrition plan could be enhanced with the development of tools or resources to enable behaviour change.
Social environment
SCT considers that the social environment, particularly family, friends and colleagues, has the potential to impact upon behaviour change (Glanz et al., 2002). Accordingly, a personalised dietary plan needed to be achievable within busy social lifestyles. Understanding of the social context of food and constraints therein, including eating outside of the home in catering establishments and with the family, was considered important to the effectiveness of personalised nutrition:
Thinking about people who have to dine out regularly, y’know somebody who’s going to lots of big dinners or things like that. (FG2, Ulster, Male, 50–59 years) How would that work as a family? Does that mean everybody’s the same or that everybody would have to be different? (FG2, Newcastle, Female, 50–59 years)
Social support
SCT defines social support as encouragement from others through feedback or verbal persuasion (McAlister et al.,2008). Discussants perceived a need for continuing support from the personalised nutrition service provider. There was also a general consensus that although the on-line interface for personalised nutrition had benefits, face-to-face contact was the preferred way of initially setting up an effective personalised dietary programme, as well as dealing with subsequent problems and for support:
I suppose you could work it face to face because then from there they can talk you through it if you haven’t got a clue, then maybe start to put together a programme or an eating programme or sort of active programme. (FG1, Newcastle, Male, 26–30 years) Personal touch you know, you’d want brought in and sat face-to-face maybe y’know if there was something seriously wrong, more than just a phone call. Can you imagine somebody sends you out all this horrific stuff on the internet and you’re thinking ‘my god, what do I do from here’. (FG2, Ulster, Male, 31–39 years)
Peer support can act as a precursor of self-efficacy by fostering independence (Bandura, 2004). Accordingly, support from others featured in the reported discussions. Interaction with those undergoing a similar programme in a coaching role could prove beneficial for some in achieving their dietary goals:
Maybe if it put you in contact with other people in a similar situation, I don’t know if it could do that. (FG1, Ulster, Female, 31–39 years) See what it’s like and then if she (a friend) was that bothered about it, you know what I mean she would ask me or ask somebody have you done it. (FG1, Newcastle, Female, 18–25 years)
Physical environment
The physical environment, the surroundings and available resources, according to SCT, can impact upon behaviour (Glanz et al., 2002). The setting or environment in which a personalised nutrition service was considered important to sustained dietary behaviour change and depending upon personal preference could be implemented at home, the workplace and/or the retail environment:
I think better from the comfort of your own home personally. When you’ve got a family and different things you are busy aren’t you? (FG2, Newcastle, Male, 40–49 years) It could be promoted through the workplace as well. Y’know it’s quite good sort of say having a morning for health checks like that, they have all those sorts of things available so it’s a quite good place to target individuals. (FG1, Ulster, Female, 50–59 years) Could it be something the big supermarkets could bring in, personalised shoppers? (FG1, Newcastle, Female, 26–30 years)
Discussion
This analysis has explored theory with which to inform how personalised nutrition should be implemented to achieve dietary behaviour change. In line with SCT, findings have suggested that individual outcome expectations, for example, those tied to weight loss, need to be taken into account when setting dietary goals. This agrees with previous qualitative research (Stewart-Knox et al., 2013) and subsequent survey (Poínhos et al., 2014) conducted as part of the Food4Me project which found that those who expected benefits were more likely to indicate intention to adopt personalised nutrition. Negative outcome expectancies were associated with on-line security and data protection which unless addressed were perceived to deter uptake of personalised nutrition, a finding that also agrees with previous qualitative (Morin, 2009; Stewart-Knox et al., 2013) and survey research (Poínhos et al., 2014; Stewart-Knox et al., 2009). More pertinent to dietary behaviour change, these results also suggest that personalised nutrition was not perceived to offer positive outcome expectancies over and above that of consuming a healthy diet. The addition of phenotypic and genetic information to lifestyle assessment was deemed useful only where there were perceived con-sequences associated with inherited life-threatening conditions. That the participants did not have prior experience with personalised nutrition, however, could go some way towards explaining this finding. Although personalised nutrition was operationally defined for the purpose of the discussion, the definition did not distinguish personalised nutrition from current practice in public dietary health promotion. A future challenge in delivering personalised nutrition to the general public, therefore, will be to convey the potential benefits over and above that of healthy eating.
These data have also emphasised the perceived importance of goal setting, self-regulation and feedback as a means through which to enhance self-efficacy to achieve positive outcome expectations. Ability to self-regulate behaviour is likely to influence compliance with personalised nutrition advice. Self-regulation has been highlighted in previous qualitative studies as motivators for undergoing personalised nutrition (Stewart-Knox et al., 2009). Discussants in this study alluded to a service which could provide on-line and/or face-to-face feedback on dietary assessments, phenotypic measures and genetic tests to enable them to monitor their progress. A recent review considering the efficacy of genome-based interventions, likewise, concluded that feedback and monitoring devices may enhance response to interventions (Bloss et al., 2011). Goal setting, monitoring and the provision of regular feedback on body fat distribution and other markers of dietary health and fitness, may be required in order to maximise progress in achieving dietary goals.
Theory would suggest that self-efficacy is a major determinant of behaviour change (Bandura, 1982). Self-efficacy was perceived to impact upon goal setting. Self-efficacy was evident in themes concerned with the perceived ability to comply with personal dietary recommendations, suggesting the importance of building ways of maximising self-efficacy into the system to aid compliance. The Food4Me survey found that those with high perceived self-efficacy were more likely to intend to adopt personalised nutrition (Poínhos et al., 2014). Self-efficacy can be encouraged through vicarious learning, mastery experience, verbal persuasion and physiological factors (Bandura, 1982, 1997). Together, these data suggest that personalised nutrition should take into account individual self-efficacy when setting dietary goals, monitoring progress and providing feedback on dietary health markers. Self-efficacy could be enhanced not only through direct experience with services but also through providing accounts of others’ experiences (e.g. through podcasts, blogs and interactive websites).
Paying for a personalised nutrition service was suggested to encourage compliance and bring about greater commitment to dietary recommendations. A recent study has suggested that the general public would be willing to pay more for personalised nutrition than for standard nutrition advice (Fischer et al., 2016). Future personalised nutrition services will need to consider the price point at which paying will enhance compliance with dietary recommendations or deter initial uptake of the service.
Consistent with SCT, the social environment and support, both from the service provider and peers, was considered important for the translation of personalised nutrition results to behaviour change. This suggests that providers may have to deliver ‘round-the-clock’ support services so clients have the sort of back-up necessary to ensure adherence to prescribed eating plans. Problems were perceived in eating out and other social occasions implying that the eating context may also have to be taken into account when planning menus. Personalised dietary recommendations to be effective may also have to take into account the food preferences of other members of the individual’s household. The physical environment in which the individual functions may also need considered. Discussants also suggested that personalised plans should be accommodated in the workplace and not just the home environment.
A limitation of this study is that because the technology was new to the market at the time of data collection, none of the discussants had any direct experience with personalised nutrition. This has limited the degree to which we can infer behaviour change from the responses. Certain constructs integral to SCT, particularly those associated with self-reward, however, did not feature among the themes discussed. Intrinsic feedback, although alluded to in these discussions, would only become evident once participants had experienced personalised nutrition. Intrinsic rewards such as those associated with enhanced well-being would only be experienced subsequent to behaviour change. Future empirical work is required with users of personalised nutrition to better understand the role of monitoring and reward in this setting.
Although successful in eliciting preferences for new nutrition-related technologies, the findings, by virtue of being qualitative, cannot be generalised to the wider population. Another limitation and one that is specific to the focus group approach is the tendency for discussion to reach consensus within the groups (Strauss and Corbin, 1998), thereby restricting the range of opinion expressed. The study has nevertheless achieved its aim which was to identify what would encourage uptake and adoption of the technology in those who never had done so previously and furthered our understanding of how different psychological, social and environmental factors may function and interact to guide an individual’s decision towards or against adopting personalised nutrition.
Conclusion
This research appears to be one of few qualitative studies to probe perceived requirements of personalised nutrition in the United Kingdom. The analytic approach adopted in the qualitative analysis is novel in adopting a ‘bottom up’ approach to the development of theory. These data appear to fit well with SCT which has provided an appropriate lens through which to understand requirements of personalised nutrition intervention for successful dietary behaviour change.
That the constructs of SCT were closely linked to the determinants of personalised nutrition and putative components of successful behaviour change could imply that the theory could be used to inform the design of individualised strategies for behaviour change that could be built into future personalised nutritional interventions.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the European Commission under the Food, Agriculture, Fisheries and Biotechnology Theme of the 7th Framework Programme for Research and Technological Development (265494).