
Abstract
Despite the prevalence of depression and alcohol use among HIV-infected individuals, few studies have examined their association together in relation to nonadherence to antiretroviral therapy in sub-Saharan Africa. This study examined depressive symptoms, alcohol use, and other psychosocial factors (stigma, demographic characteristics) in relation to nonadherence to antiretroviral therapy among clinic-attending, HIV-infected individuals in South Africa (n = 101). Nonadherence was assessed using event-level measurement (missed doses over the past weekend). Multivariable logistic regression analyses revealed that only alcohol use, over and above depressive symptoms and education level, was associated with antiretroviral therapy nonadherence(AOR = 1.15; 95%CI = 1.02–1.29; p < .05). Findings point to the independent association of alcohol use and nonadherence to antiretroviral therapy above and beyond depressive symptoms.
Introduction
Depressive symptoms and alcohol use are prevalent among HIV-infected individuals, and both are associated with antiretroviral therapy (ART) nonadherence (Mayston et al., 2012). ART nonadherence contributes to greater morbidity and mortality among HIV-infected individuals, and higher likelihood of sexual HIV transmission when virus is detectable (Cohen et al., 2011). In areas most affected by the HIV/AIDS epidemic, such as areas of sub-Saharan Africa where access to multiple ART regimens is also limited, there are even greater consequences to ART nonadherence, including developing drug resistance and failing the only available first- and second-line ART regimens (Marconi et al., 2008; Palombi et al., 2009).
Although the majority of research examining depression, substance use, and ART adherence has been conducted in the United States, Nakimuli-Mpungu et al. (2012) published a meta-analysis of studies examining the relationship between these outcomes among HIV-infected individuals in sub-Saharan Africa. In this meta-analysis, the prevalence of depressive symptoms was 31.2 percent across 23 studies, and the likelihood of optimal ART adherence was 55 percent lower among those with depressive symptoms compared to those without (Nakimuli-Mpungu et al., 2012). Regarding alcohol use, six studies were identified that reported on the prevalence of alcohol use disorders (AUDs) among HIV-infected individuals, including four in South Africa (prevalence ranged from 7 to 31 % Kekwaletswe et al., 2011; Myer et al., 2008; Nachega et al., 2011; Olley et al., 2006), one in Uganda (7.8% prevalence; Nakimuli-Mpungu et al., 2011), and one in Nigeria (21.7% prevalence; Farley et al., 2010). Additionally, five studies reported on any alcohol use in the past month (Do et al., 2010; Etienne et al., 2010; Martinez et al., 2008; Peltzer et al., 2010; Weidle et al., 2006), and one reported on any alcohol use in the past 3 months (Simbayi et al., 2007). However, too few studies were identified to be able to pool estimates of alcohol use and AUDs among HIV-infected patients in sub-Saharan Africa (Nakimuli-Mpungu et al., 2012). Further, only three studies assessed the relationship between alcohol use and ART adherence, and each of these found a significant negative relationship between alcohol use (even at subclinical levels) and ART adherence (Etienne et al., 2010; Kekwaletswe et al., 2011; Nachega et al., 2011). Finally, only one study examined the association between depressive symptoms and alcohol use together in a larger model in relation to ART adherence (Etienne et al., 2010).
Although data have accumulated in recent years, overall, there are still limited data on the prevalence of alcohol use and AUDs among HIV-infected individuals in sub-Saharan Africa, and their relationship with ART adherence after accounting for co-occurring depressive symptoms. Documenting this relationship is particularly relevant in South Africa, where the largest number of HIV-infected individuals is living worldwide, and rates of per capita alcohol consumption are among the highest in the world (Shield et al., 2013). Aims of this study were to (1) add to the existing published literature the prevalence of alcohol use among clinic-attending, HIV-infected individuals in South Africa, and (2) examine the relationship between alcohol use and ART nonadherence in this population after accounting for depressive symptoms and other relevant psychosocial factors.
Method
Participants and procedures
Participants were recruited from a peri-urban public hospital–based ART clinic in South Africa. Patients were eligible if they were (1) ⩾18 years of age; (2) receiving ART for a minimum of 6 months; and (3) able to complete all study procedures. Patients were excluded if they had been diagnosed with bipolar or psychotic disorder. Clinic nurses informed ART receiving patients about the research study; if interested, the patient could approach a research staff member in a private room at the clinic to learn more about the study. After study procedures were explained, interested participants provided written informed consent, including permission to obtain blood test results from this clinic visit. Study procedures included a one-time self-report questionnaire administered in English, Xhosa, or Afrikaans depending on participant preference. Participants were reimbursed with a grocery voucher (ZAR 50, ~US$5) for their time. Clinic nurses were also given grocery vouchers for providing patients with basic information about the study. All study procedures were approved by the Stellenbosch University Health Research Ethics Committee, and permission to conduct the study was granted by the Western Cape Department of Health.
Assessments
Demographic information
A locally developed demographics questionnaire assessed age, gender, education level, marital status, employment, annual family income, and race/ethnicity.
Alcohol use disorder identification test
The alcohol use disorder identification test (AUDIT) is a 10-item self-report measure used to assess alcohol use and related problems (Babor et al., 2001). The AUDIT has been previously validated among South African HIV-infected patients receiving ART and had good sensitivity and specificity compared to the Mini-International Neuropsychiatric Interview (M.I.N.I.) (Myer et al., 2008). Scores range from 0 to 40, and a score ≥8 indicates alcohol-related problems (Pérula-de Torres et al., 2005; Reinert and Allen, 2007; Saunders et al., 1993).
Beck depression inventory
Depressive symptoms were assessed using the Beck Depression Inventory (BDI-II), a 21-item self-report assessment of depressive symptoms (Beck et al., 1996). The BDI-II has been shown to have good psychometric properties in a South African sample (e.g. α = 0.93; Steele and Edwards, 2008). Scores from 0 to 13 are considered minimal depressive symptoms, 14 to 19 reflect elevated or mild depressive symptoms, 20 to 28 reflect moderate depressive symptoms, and 29 to 63 reflect severe depressive symptoms.
HIV-related stigma
Perceived HIV-related stigma was assessed using the 40-item Berger’s HIV stigma scale (Berger et al., 2001). Higher scores reflect greater perceived stigma. Response options for each item are on a scale from 1 (strongly disagree) to 4 (strongly agree). The scale has good psychometric properties (α = 0.96) and had excellent internal consistency in our sample (α = 0.93) (Berger et al., 2001).
CD4 count and viral load were included as biological markers of health status and disease progression. The most recent CD4 count and viral load results (within the past 6 months) were obtained from patients’ medical records, which were measured during routine blood tests at their clinic visit.
ART nonadherence
ART nonadherence was assessed using self-reported, event-level measurement: “Did you forget to take any of your HIV medications over the past weekend?” Event-level measurement has often been used in assessing HIV-risk behavior (i.e. to describe a specific behavior during a recent time window rather than reporting overall rates of behavior) to minimize overreporting, recall, and social desirability biases (Gillmore et al., 2002; LaBrie et al., 2005; Schroder et al., 2003; Tortu et al., 2000). The event-level assessment was drawn from a larger six-item self-report measure of adherence and was selected to minimize recall bias noted in prior work with this sample (Kagee and Nel, 2012). Of note, this item was significantly correlated with self-reported adherence in the past week (rpb = .31, p < .01), in the past 2 weeks (rpb = .37, p < .0001), and past month (rpb = .31, p < .001), and was selected to minimize recall bias.
Statistical analysis
First, bivariate analyses were conducted examining the relationship between the demographic and clinical variables listed above and the dependent variable (ART nonadherence). Next, a multivariable logistic regression model was conducted, entering into the model variables related to ART nonadherence in bivariate analyses. To be overly conservative, we included variables that were significantly related to ART nonadherence at p < .15. Model fit was assessed using the Hosmer–Lemeshow (H–L) goodness-of-fit statistic (p > .05 indicates good fit for the logistic regression model). All analyses were run in SPSS version 21.
Results
Demographic and clinical characteristics of sample
In total, 107 participants were enrolled into the study. Of those, 5.6 percent had substantial missing data (n = 6) and were excluded from the current analyses. Of the final sample (n = 101), mean age was 35 years (SD = 7), and the majority of participants were female (82.2%) and Black (66%). Approximately half of participants (52.1%) had elevated depressive symptoms on the BDI (scores ⩾14), and approximately 17 percent scored in the elevated range on the AUDIT. Approximately 17 percent of the sample reported missing a dose over the past weekend. Table 1 lists other demographic and clinical characteristics for the total sample and by ART nonadherence over the past weekend.
Demographic and clinical characteristics of sample and by missed dose status in the past weekend.
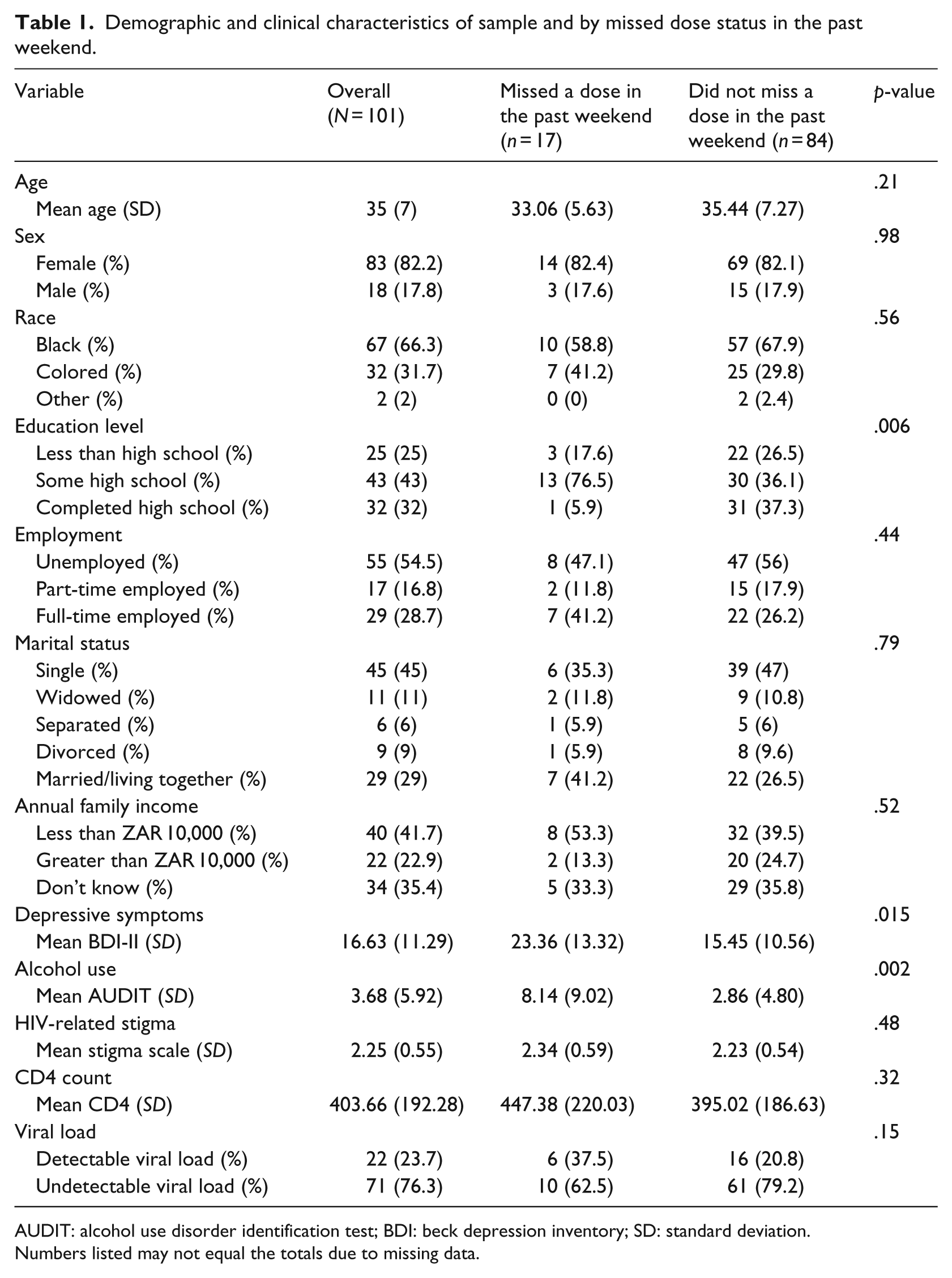
AUDIT: alcohol use disorder identification test; BDI: beck depression inventory; SD: standard deviation.
Numbers listed may not equal the totals due to missing data.
Bivariate analyses
At the bivariate level, greater alcohol use (rpb = .33, p < .01) and depressive symptoms (rpb = .26, p < .05) were significantly positively related to ART nonadherence; individuals who missed a dose over the past weekend (compared to those who did not) had mean BDI-II scores of 23.36 (SD = 13.32) versus 15.45 (SD = 10.56) and mean AUDIT scores of 8.14 (SD = 9.02) versus 2.86 (SD = 4.80), respectively. Of note, AUDIT and BDI-II scores were not significantly correlated with each other (r = .15, p = .2).
Of the demographic characteristics, only education was related to ART nonadherence (χ2(2) = 10.15, p < .01). All other variables were not significantly related to ART adherence (all ps > .15; see Table 1), with the exception of viral load (detectable vs. not), which, as expected, was related to self-reported ART adherence (χ2(1) = 2.05, p = .15).
Multivariable logistic regression model
Variables significantly related to the dependent variable (ART adherence: “Did you forget to take any of your HIV medications over the past weekend?” 0 = no; 1 = yes) were included in the multivariable logistic regression model (BDI-II, AUDIT, and education level). Viral load was not included as a covariate, as detectable virus is the direct biological consequence of ART and rather supports the credibility of distinguishing individuals based upon missing a dose in the past weekend. In the final model, only alcohol use was associated with ART nonadherence (adjusted odds ratio (AOR) = 1.15; 95% confidence interval (CI) = 1.02–1.29, p < .05). The H–L statistic indicated good model fit (χ2(8) = 5.84; p > .05).
Discussion
This study adds to the published literature (1) the prevalence of depressive symptoms and alcohol use among clinic-attending, HIV-infected patients in South Africa, and (2) associations between depression, alcohol use, and ART adherence in a multivariable model. Findings point to elevated rates of depressive symptoms and alcohol use among individuals who reported a recent missed ART dose. In the final adjusted model, findings point to the important role of alcohol use over and above depressive symptoms and education levels in relation to ART nonadherence.
Findings are in line with another recently published study examining the association between alcohol use and ART adherence among clinic-attending, HIV-infected patients in South Africa (Morojele et al., 2014), which found that approximately 20 percent of the sample (n = 304) reported hazardous alcohol use on the AUDIT. Although Morojele et al. (2014) did not account for depressive symptoms, they did examine other psychosocial factors in relation to ART adherence that were included in this study, including demographic characteristics and HIV stigma. Similar to the current study, in their results, AUDIT scores were associated with ART adherence even after accounting for these other factors (Morojele et al., 2014).
It was somewhat surprising in our sample that depressive symptoms and alcohol use were not significantly correlated given high comorbidity reported elsewhere among HIV-infected samples (Chander et al., 2006; Sullivan et al., 2011). Perhaps with a larger sample that had been recruited specifically based upon elevated depressive symptoms and/or alcohol use patterns, this would have illustrated a stronger relationship. Other research in South Africa has found that individuals with hazardous/harmful rates of alcohol use are less likely to be on ART medication (Kader et al., 2014). Thus, by only including individuals who are on ART, this likely excludes individuals with more severe alcohol use, which may also bias the relationship between depressive symptoms and alcohol use found in our sample.
Study findings must be interpreted in the context of important limitations. First, this was a clinic-attending patient sample, which may not generalize to non-clinic-attending, HIV-infected patients. Second, this was a cross-sectional survey, and thus we cannot infer directionality or causality. Third, we relied on self-report measurement of adherence, depression, and alcohol use. Self-report, particularly of sensitive information, may be subject to social desirability and recall biases. Although we tried to address limitations of self-reported ART nonadherence using recent, event-level measurement (i.e. “Did you forget to take any of your HIV medications over the past weekend?”), it may be that nonadherence over the past weekend may not be representative of the participant’s cumulative behavior. That being said, prior research has documented the benefits of using event-level measurement for behaviors susceptible to recall and social desirability biases (Kiene et al., 2009; Reynolds et al., 2010). Furthermore, this item was found to be, at borderline significance, related to detectable viral load (p = .15), suggesting the measure is reflective of a longer time window of ART adherence than just the past weekend. Particularly for patients with depressive symptoms or hazardous alcohol use, who may be susceptible to recall biases, limiting the time window to a recent period may have increased the reliability and validity of reporting.
Despite these noted limitations, study findings add to the existing literature the prevalence of alcohol use among HIV-infected, clinic-attending patients in South Africa. Given that data have been scarce reporting on alcohol use and AUDs among HIV-infected patients in sub-Saharan Africa (Nakimuli-Mpungu et al., 2012), it is important to continue to add to this literature to enable pooled estimates in future meta-analytic work. Additionally, this study examined the relationship between alcohol use and ART adherence after controlling for depressive symptoms, one of the most important comorbid psychosocial factors among HIV-infected, alcohol-using patients in relation to ART nonadherence (Berger-Greenstein et al., 2007). Current findings point to the association of alcohol use and ART nonadherence above and beyond depressive symptoms. Future research is needed to replicate these results in a larger sample using community-based recruitment, and to continue efforts to develop and implement evidence-based, integrated interventions to address both alcohol use and ART adherence simultaneously (Kekwaletswe and Morojele, 2014).
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the National Research Foundation (NRF) in South Africa and Stellenbosch University. Dr Magidson’s work on this manuscript was supported by NIMH grant T32MH093310.