
Abstract
Health avatars were created to deliver previously tested live interventions for tobacco dependence and cholesterol management. The exploratory aims were to develop and test whether the avatar can be reliably assessed for autonomy supportiveness using the Health Care Climate Questionnaire and estimate the mean changes in motivation variables and correlate the avatars’ autonomy supportiveness with the motivation variables and health outcomes. The avatars were found to be reliably assessed for autonomy supportiveness on the Health Care Climate Questionnaire. Autonomy support was positively correlated with the change in motivations and reduction in low-density lipoprotein. These findings suggest that health avatars may be tested in clinical trials.
Keywords
Introduction
Tobacco use and elevated low-density lipoprotein (LDL) cholesterol are major risk factors for cardiovascular disease (CVD). Effective treatments exist with therapeutic lifestyle change and medications that lower the risk of CVD events including sudden death, myocardial infarction, and stroke (Stone et al., 2013; Fiore et al., 2008). Interventions that change patient lifestyle, increase use of medication, and reduce CVD events are time intensive for clinicians and are more successful over the long-term if based on the principles of human motivation and medical professionalism (Ng et al., 2012).
This brief report describes the creation and pilot testing of two Virtual Clinician Research Tools (VCRTs) that would deliver the effective Smokers’ Health Study intervention for tobacco dependence and lowering LDL cholesterol (Williams et al., 2006a, 2006b). The VCRTs integrated principles of self-determination theory (SDT; Deci and Ryan, 2000) with our tobacco dependence treatment guidelines (Fiore et al., 2008) and the National Cholesterol Education Program (NCEP III; Grundy et al., 2004) guideline. Both SDT and the VCRT are briefly described below, followed by a description of the methods for the initial pilots.
VCRTs
A health avatar (e.g. physician or dietitian) presented standard treatment information provided in face-to-face SDT-based interventions in a series of virtual encounters that participants accessed online using a personal computer to develop their plan for addressing their tobacco use (eight encounters) or high LDL cholesterol (three encounters). The number of encounters for each series was similar to that for live interventions (Williams et al., 2006b). The avatars interact with participants to assess and inform them of their cardiovascular risk by calculating their 10-year Framingham Risk Score for developing heart disease, the potential benefits of lowering LDL cholesterol through diet and medication changes, and for those who smoke, by stopping smoking. The VCRT provided support for subject psychological needs for autonomy (i.e. volition) and relatedness, by providing information (e.g. CVD risk estimate), and then asking how the subject felt about hearing the information. The subject was provided four response options. The avatar then voiced a prewritten acknowledgement to the subject’s response. The avatar supported autonomy and competence by providing a list of effective options the subject could add to their treatment plan that reduced that risk. Participants reviewed their treatment plan with their actual clinician and to receive any medication prescriptions that are needed.
The first aim was to create the VCRTs and test to see whether they could be reliably rated (using Cronbach’s alpha) for their autonomy supportiveness on the modified Health Care Climate Questionnaire (mHCCQ) and to compare the participants’ mean mHCCQ ratings for the avatar to that for their real doctor. The second aim was to estimate the mean changes in motivation variables and to correlate the avatars’ autonomy supportiveness with participants’ change in autonomous self-regulation, perceived competence, abstinence from tobacco, or lower LDL cholesterol.
Method
Recruitment
Participants were enrolled in the tobacco pilot if they smoked five or more cigarettes per day or in the cholesterol pilot if they had moderate or moderately high risk for coronary artery disease as defined by NCEP III (two or more of the following risk factors: male age 45 years or over; female age 55 years or older; high-density lipoprotein cholesterol (HDL-C) less than 40 mg/dL; active smoking; family history of coronary heart disease (CHD) in males aged 55 years or less/females aged 65 years or less; Grundy et al., 2004). To be included in the cholesterol pilot, individuals also had to have an average of two LDL cholesterol test results greater than 100 mg/dL. Participants were eligible regardless of their desire to lower their cholesterol or to stop smoking. Individuals were fluent in English. Participants also had access to a computer with Internet access to complete a series of online questionnaires, as well as, to view the VCRT.
Participants were excluded if they were pregnant or lactating, had a psychotic or mood disorder, were too sick to participate, unable to make decisions about medications for themselves, or had a life expectancy of less than 12 months (e.g. advanced cancer). Participants were excluded if they had a heart attack or a stroke, diabetes mellitus, aortic aneurysm, peripheral vascular disease, or chronic kidney disease.
Participants were recruited from primary care practices in the Rochester, NY, area and were scheduled for at least two doctor visits with one of two physicians (G.C.W. and J.F.C.) associated with the University of Rochester, plus three to eight sessions with the avatars. Eligible participants received informed consent and completed a baseline questionnaire on a computer kiosk, prior to any intervention. Participants received an honorarium of US$200 (prorated) for completing the entire study.
Data collection
Psychological measures were assessed monthly during the 2-month interventions. The participants were asked to complete modules weekly and to have their physician visits at 2 and 7 weeks.
Process measures
mHCCQ
The mHCCQ (six items, 7-point Likert scale; Williams et al., 2002) measured the perceived autonomy supportiveness of the VC on one assessment and their study doctor (SD) on a second assessment. A sample item is “My healthcare avatar provided me with choices and options for how to eat a healthy diet.”
Autonomous self-regulation
Autonomous self-regulation (ASR) for stopping smoking and reducing LDL cholesterol (six items each, 7-point Likert scale) was assessed using the Treatment Self-Regulation Questionnaire (TSRQ; Levesque et al., 2007) at baseline and 2 months. A sample item is “The reason I will eat a healthy diet is that I feel that it is important for my health.”
Perceived competence
The Perceived Competence Scale (PCS; Williams et al., 2002) measured feelings of efficacy concerning diet to lower cholesterol and concerning stopping smoking (five items each, 7-point Likert scale). These were assessed at baseline and 2 months. Sample item is “I feel capable of stopping smoking completely.”
End of study assessment
Two fasting lipid profiles were drawn 7 days apart at 3 months, and tobacco participants were called at 3 months to determine their 7-day point prevalence abstinence and the number of days since their last cigarette.
Data analysis
Cronbach’s alpha was used to determine the internal consistency of the mHCCQ for the Study Doctor (HCCQ-SD) and Virtual Clinician (HCCQ-VC). Correlations and multiple regressions were used to determine the relations between the measure of need supportiveness, motivation variables, and health outcomes. Comparison of continuous measures between baseline and 2-month follow-up was performed using a Student’s t-test. Statistical tests that significantly different are indicated by p < 0.05 or p < 0.01; otherwise, they are not significant.
Results
A total of 33 participants enrolled in the virtual clinician (VC) interventions: tobacco cessation (n = 15) and cholesterol (n = 18). Participants were mostly White and had more than a high school education (Table 1). The distribution of the variables of interest was explored and found that HCCQ, ASR, and perceived competence were skewed to the right. In comparison, the fasting lipids were normally distributed and longest time of not smoking was skewed to the left. Three of the 15 smokers had stopped smoking (20% 7-day point prevalence abstinence), and there was a small decrease in LDL cholesterol from 136 to 133 mg/dL.
Demographics, motivation, and outcome variables for the VCRT avatars.
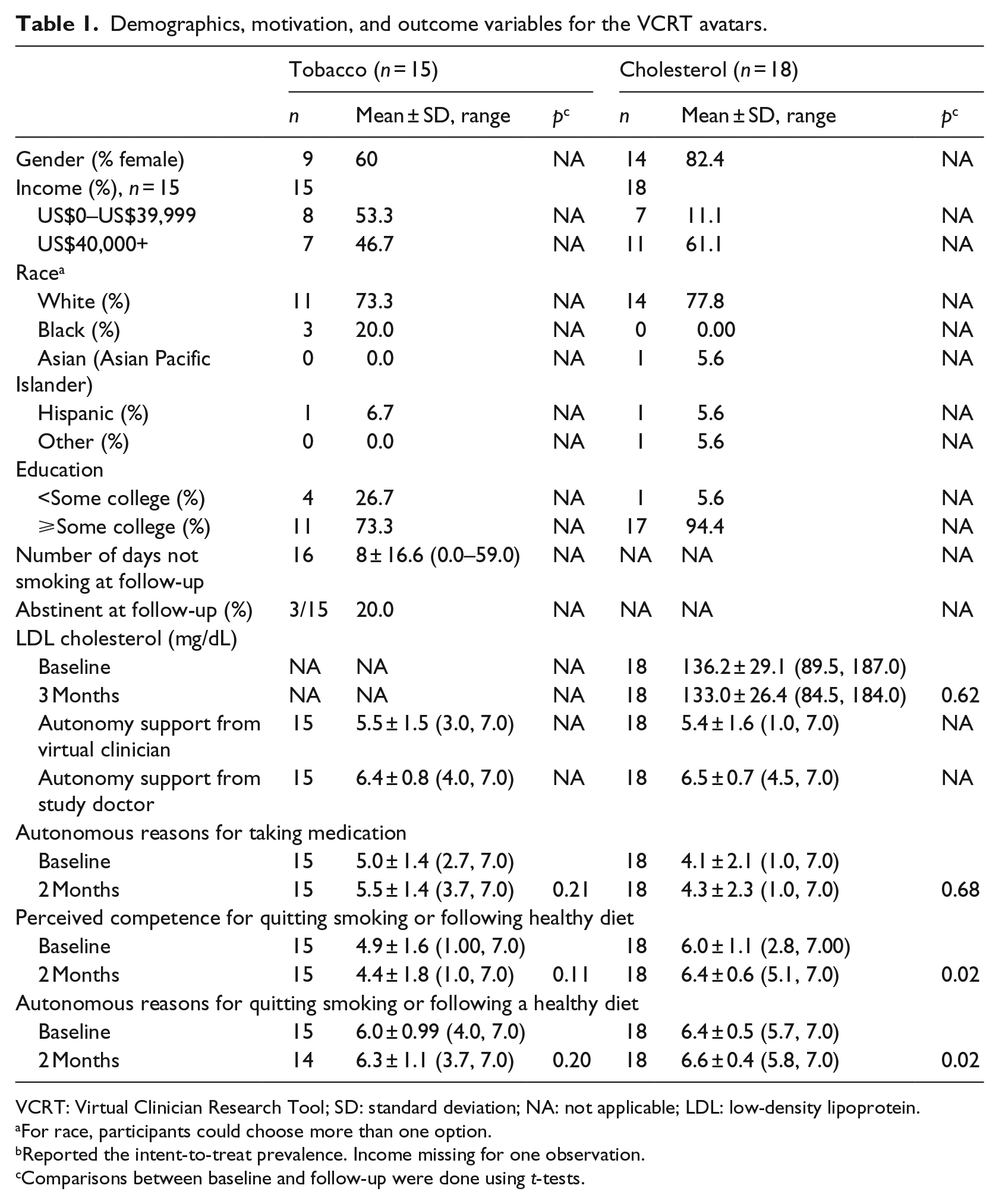
VCRT: Virtual Clinician Research Tool; SD: standard deviation; NA: not applicable; LDL: low-density lipoprotein.
For race, participants could choose more than one option.
Reported the intent-to-treat prevalence. Income missing for one observation.
Comparisons between baseline and follow-up were done using t-tests.
Aim 1
The HCCQ-VC had strong internal reliability for both the participants rating avatars in the tobacco (0.95) and cholesterol (0.94) dataset. Overall, participants found the standard deviation (SD) significantly more autonomy supportive than their VC (M = 5.5 vs 6.4, p < 0.05, Cohen’s d = 0.77 tobacco; M = 5.4 vs 6.4, p < 0.01, Cohen’s d = 0.72 cholesterol).
Aim 2
The mean need support (HCCQ-VC) experienced during the study by participants from the VC was positively correlated with ASR for cessation (r = 0.16) and for diet to lower LDL (r = 0.30) during the study. HCCQ-VC was positively correlated with perceived competence for following a healthy diet to lower LDL (r = 0.39), but negatively correlated with perceived competence for cessation (r = −0.27).
The standardized β between the change in ASR (average during the study controlling for baseline) and HCCQ-VC was positive for cessation (β = 0.33) and for healthy diet (β = 0.19). Similarly, residual change in perceived competence for cessation was regressed onto HCCQ-VC and showed a negative relation (β = −0.20), but showed a positive trend in predicting the change in perceived competence for healthy diet (β = 0.37). The mean perceived competence for cessation fell (4.9 to 4.4, p = not significant (ns)) from baseline to 2 months. The mean ASR around tobacco (6.0–6.3, p = ns) and cholesterol (6.4–6.6, p < 0.05) and the mean perceived competence for cholesterol (6.0–6.4, p < 0.05) all increased from baseline to 2 months.
Discussion
The pilot tests of a virtual avatar delivering tobacco and lipid guideline-based counseling demonstrated mixed results. Both were successful in that the avatars were able to deliver relevant health information in a relatively autonomy supportive manner, based on the mean levels of the HCCQ-VC, and the increase in ASR and perceived competence, with the exception of the fall in perceived competence around abstinence. However, the effect sizes of the standardized coefficients between the autonomy supportiveness of the avatars, subject motivation, and health outcomes are difficult to interpret because of the small sample sizes, but most went in the predicted direction. They may serve as initial estimates for sample size calculations for future studies.
Not surprisingly, the VCRTs’ autonomy supportiveness ratings were significantly lower than those for the physicians. This was a moderate to large effect (Cohen, 1988). If confirmed in larger studies, this supports pairing the VC with brief contacts with the healthcare practitioner, to be sure that the autonomy supportiveness of the healthcare practitioner is not lost.
The health behavior change literature has demonstrated strong relations between amounts of contact time, number of intervention sessions, and the changes in health behaviors over the long-term (Stone et al., 2013; Fiore et al., 2008). However, there is little time for physicians to deliver these interventions with the needed intensity (Yarnall et al., 2003). Tobacco and lipid interventions involve motivating lifestyle change as well as motivating the use of medications to be most effective. Virtual systems may help fill in this “contact time” gap and have better reach into the population. For example, these might support primary care in delivering nutrition and physical activity recommendations to a population of patients around cholesterol, weight, or hypertension without dramatically increasing the contact time with the clinician. They also may allow us to better identify effective aspects of an intervention by the systematic comparison of intervention components to increase autonomy supportiveness and motivation.
Although not specifically tested here, the nature of the technology behind these two research tools is that they can be altered systematically with respect to the information provided, contact time, delivery platform, aspects of need supportiveness of the avatar, racial, gender, and cultural characteristics of the avatar. This allows for opportunity to evaluate how these factors influence motivational and health improvement qualities and the potential to identify optimal levels of tailoring and patient-avatar matching across diverse patient populations.
The limitations of these pilots include the small number of participants included, the rapidly changing electronic platforms that limit the time that a particular tool can be used, and lack of universal patient access to the Internet. However, the VCRTs may also be delivered on mobile phones in the future which may have greater reach into the low-income and low literacy populations. More research is needed to determine the efficacy and cost-effectiveness of these systems. Most, but not all, relations between the VC and SDT mediators were positive and similar to those in SDT health research, but a few were unexpectedly negative. Further research with larger, more diverse samples will determine the effect these systems have on health.
Conclusion
In summary, two VCRTs were created that delivered interventions for tobacco dependence and elevated LDL cholesterol integrated with SDT. These VCs can be systematically altered to study the variations in style of presentation, information content, and VC characteristics to determine optimal effects on health and well-being. Behavior change counseling is time intensive. Use of a virtual, interactive tool to assist in delivering health behavior change interventions in conjunction with real clinicians may be comparatively more effective for population health than systems that do not utilize these. This report describes development of a tool that can be used in controlled, randomized trials to augment effective interventions and to test new ones.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by grants from NIDA (DA024262) awarded to G.C.W, MD, PhD; National Center for Research Resources (M01-RR0044) awarded to the University of Rochester’s General Clinical Research Center; and UL1RR024160 awarded to the University of Rochester’s Clinical and Translational Science Institute.