
Abstract
This qualitative study aimed to explore home haemodialysis and in-centre haemodialysis patients’ experience, to illuminate barriers and facilitators in the uptake and maintenance of home haemodialysis. Thirty-two semi-structured interviews with patients receiving home haemodialysis or in-centre haemodialysis were analysed using framework analysis. Four themes emerged: ‘perceptions of self’; ‘impact of haemodialysis on family’; ‘perceived advantages and disadvantages of home haemodialysis and in-centre haemodialysis’ and ‘practical issues and negotiating haemodialysis’. The lived experience of home haemodialysis was in contrast to the lived experience of in-centre haemodialysis and to the anticipated experience of home haemodialysis, highlighting patient factors that contributed to under-usage of home haemodialysis.
Introduction
Chronic kidney disease (CKD) is a progressive condition and global public health concern (Levey et al., 2007; Obrador et al., 2011). The stages of CKD are based on the level of kidney function; the fifth and final stage of CKD, also known as end stage renal disease (ESRD), requires renal replacement therapy (RRT) to sustain life. Haemodialysis is the most commonly employed RRT, with 43 per cent of UK ESRD patients (Shaw et al., 2013). Haemodialysis may take place at home, hospital or another medical centre.
Extended haemodialysis at home has been shown to deliver the best clinical outcomes and survival rates (Lorenzen et al., 2012; Pauly et al., 2010). Home haemodialysis (HHD) is also more cost-effective than in-centre haemodialysis (ICHD) (Mowatt et al., 2003). However, 12 years after the UK National Institute for Health and Care Excellence (NICE) guidelines on haemodialysis, the target of providing HHD to 10–15 per cent of the dialysis cohort remains unmet; the median percentage of dialysis patients using HHD in the United Kingdom is 2.9 per cent (Castledine et al., 2011). Instead, there has been a gradual decline in the uptake of HHD in the United Kingdom, largely in favour of ICHD. Therefore, it is imperative that potential barriers to the uptake of HHD are identified and addressed to ensure more patients benefit from the advantages of HHD.
Studies have focused on institutional reasons for the low uptake of HHD, including clinician biases against home dialysis therapies (Durand-Zaleski et al., 2007; Mehrotra et al., 2005; Nesrallah and Mendelssohn, 2006; Thamer et al., 2000); limited exposure to home dialysis in clinician training (Golper et al., 2011); limited resources to devote to motivating patients to self-care at home (Ledebo, 2008); insufficient pre-dialysis education (Goovaerts et al., 2005; Little et al., 2001); insufficient physical infrastructure to support the patient dialysing at home (Ludlow et al., 2011; Marrón et al., 2005) and payor issues (McFarlane and Komenda, 2011).
However, patient-related factors also contribute to the under-usage of home dialysis. The rise of co-morbidities among patients has been suggested to have reduced the uptake of home dialysis (MacGregor et al., 2006). A survey of ICHD patients suggested fear of change, fear of social isolation, time constraints and needle phobias prevented HHD (McLaughlin et al., 2003).
To date, qualitative research on this topic has largely focused on the views of small numbers of HHD patients (Cases et al., 2011; Xi et al., 2012). Studies analysing qualitative data from patients on different modalities are few, and are limited either by presenting data for each modality independently (Cafazzo et al., 2009) or by not differentiating their findings according to modality (Polaschek, 2007). To our knowledge, there has not been a study which has compared and contrasted data from patients using HHD and ICHD. By exploring HHD and ICHD patients’ experiences of their chosen modality as well as their perceptions of the modality they did not select, this study can provide further insights concerning barriers and facilitators to the uptake and maintenance of HHD. The HHD and ICHD dataset will complement and supplement one another, thereby producing a more comprehensive understanding of the complex issues under study.
Methods
Participant selection and study setting
Eligible patients undertook haemodialysis, were aged 18 years or over and were English or Urdu speaking. Participants with severe mental health or learning difficulties, as defined from their medical notes, were excluded due to lacking capacity to give informed consent. Purposive sampling was used to capture a range of patient demographics namely age, ethnicity and gender. All participants were recruited from one hospital with approximately 150 ICHD and 60 HHD patients. Having obtained ethical approval from the Greater Manchester West Health Research Authority National Research Ethics Service (Reference 12/NW/0170), eligible ICHD patients were approached in-person during their hospital visit while HHD patients were posted a letter inviting them to participate. All patients were told of their right to refuse to participate or withdraw from the study without giving any reason and without their standard of care being affected.
Data collection
Drawing on the literature (Cafazzo et al., 2009; Cases et al., 2011; Polaschek, 2007; Xi et al., 2012) and expert opinion, an interview topic guide was designed to investigate patients experiences of the modalities they had undertaken and views of the modalities they had not. The topic guide is provided in Table 1. The topic guide was translated into Urdu, to facilitate the recruitment of non-English-speaking South-Asian patients. This group is under-represented in the UK literature despite the high incidence and prevalence of ESRD in South-Asian communities (Shaw et al., 2013).
Interview topic guide.

HHD: home haemodialysis; ICHD: in-centre haemodialysis.
After successful piloting, face-to-face digitally audio-recorded semi-structured interviews were conducted between December 2012 and April 2013. Recruitment was terminated when theoretical saturation had been achieved, that is, no new themes emerged from subsequent interviews (Legard et al., 2003). Patients chose where interviews took place; all of the ICHD patients’ interviews took place in the hospital while all but four of the HHD patients were interviewed at home. The hospital patients chose to have their interview undertaken while dialysing so as to utilise time, whereas only four of the home participants were dialysing when interviewed. Due to the temporal effects of dialysis on patients’ cognition, interviews began 30–60 minutes into the dialysis session and patients were not interviewed after their 2-day dialysis break (Williams et al., 2004). Interviews lasted from 30 to 150 minutes.
The interviews were conducted by RM and CM. Three of the interviews were undertaken in Urdu, the remainder were conducted in English. The English language audio-recordings were transcribed verbatim. The Urdu ones were translated and transcribed into English by RM. A second researcher, AJ, listened to the Urdu recording alongside reading the English language translated transcription to verify them. No amendments were advised as a result of this.
Data analysis
After each interview, field notes were made and a reflexive diary was maintained. Interview transcripts were uploaded into NVivo10, to facilitate storage, management and coding of the data. A framework analysis approach was employed (Ritchie and Spencer, 1993); and this is an emerging descriptive qualitative approach. Framework analysis is a structured data analysis method as opposed to a research paradigm such as grounded theory. Framework analysis is increasingly used in healthcare settings (Swallow et al., 2011; Tierney et al., 2011) as it is particularly suited to research that focuses on addressing specific questions in an applied way that is useful for informing policy and practice (Ward et al., 2013).
Initially, RM familiarised herself with the data by reading and re-reading each transcript and the associated field notes for context. Subsequently, transcripts were split into codes that would get indexed and charted. AW coded 20 per cent of the interviews to test inter-rater reliability (Malterud, 2001). There were no significant discrepancies in the codes. In the next stage, recurring themes were organised into a draft theoretical framework. This process was repeated several times, addressing the study aims to begin with, however, becoming increasingly conceptual. In the third stage of ‘indexing’, this theoretical framework was applied to each transcript and themes were combined, refined and developed. Throughout the next stage of ‘charting’, indexed data in the framework was examined and summarised using the constant comparison process (Glaser and Strauss, 1967). In the final stage of ‘synthesising the data’, data from both samples that had been analysed separately were reanalysed as a whole. Themes were compared with the original transcripts. By comparing more abstract analyses with the original raw data, discrepancies and overstatements were minimised, thereby ensuring rigour (Ezzy, 2002). Regular discussions with the multi-disciplinary team throughout analysis enhanced transparency (Dixon-Woods, 2011).
Findings
In all, 37 participants were approached, of these 32 agreed to take part. Of the five that did not want to take part, three ICHD patients reported lacking energy and two HHD patients stated time pressures. Demographic characteristics of the 32 study participants are in Table 2. Each modality sample was representative of the cohorts they were drawn from with respect to age, based on information from hospital records.
Demographic characteristics of sample.
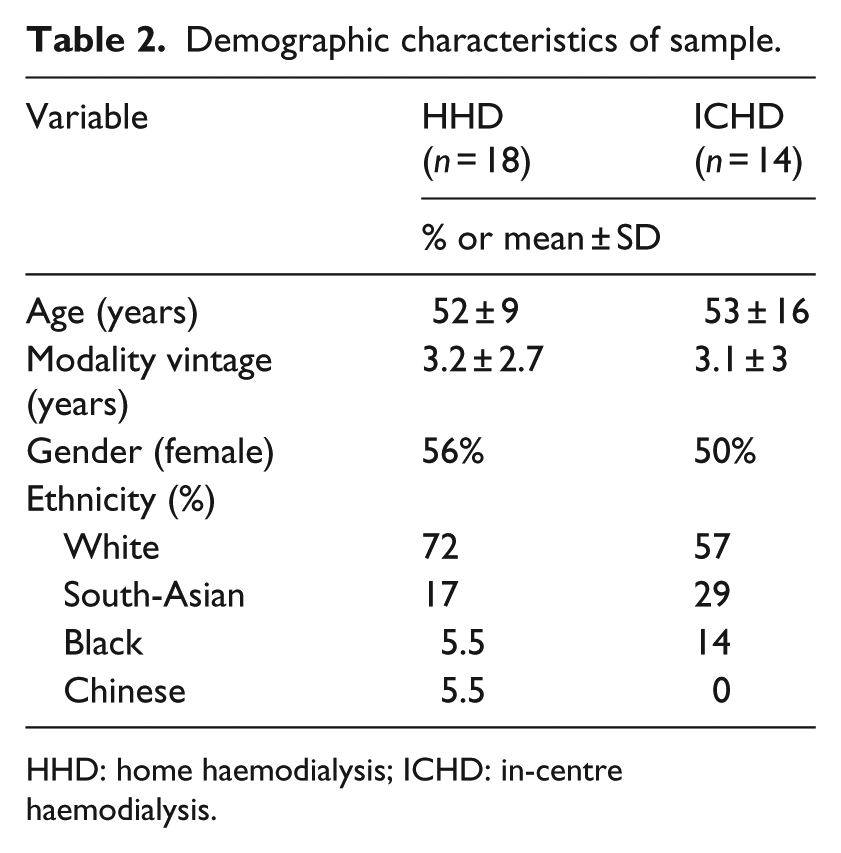
HHD: home haemodialysis; ICHD: in-centre haemodialysis.
Four main themes emerged from the data regarding patient-related factors surrounding the barriers and facilitators to the uptake and maintenance of HHD. These are presented below.
Perceptions of self
Beginning haemodialysis treatment changed patient’s lives, as having to attend dialysis sessions and following a diet resulted in restrictions of personal freedom. Regardless of modality, patients distinguished between their lives on a dialysis day versus a non-dialysis day, causing them to view their lives in a compartmentalised way: My friends and family know that on dialysis day you don’t talk to me about any problem you have or about any problem I have or anything, you know, just how are you, how are you, bye, you know. There’s no discussion, there’s no serious decisions made on dialysis day because one thing I’ve learnt is on dialysis day I’m not myself. (Joyce, age 52, ICHD)
Patients talked about altered perceptions of their own mental and physical health since the onset of dialysis. HHD patients talked about pushing themselves to self-manage in spite of experiencing disorientating changes and thereby building confidence. In contrast, ICHD patients spoke of low self-efficacy preventing them from managing dialysis at home: It was quite difficult sometimes because it blew quite a lot early on and that tends to make you a bit apprehensive … the first week, couple of weeks, when I was at home on my own there was the odd problem but for months there’s been no real problem because then you get more confidence. (Andrew, age 69, HHD) I don’t think I’d be confident enough to do myself at home. I think I could pick it up, I’ve seen enough done here, I’m sure I could pick it up, but I’m not confident enough to do it at home. (Helen, age 60, ICHD)
The impact of haemodialysis on family
As well as noting the influence of haemodialysis on the self, both groups talked about the influence it had on family members. ICHD patients remarked on how their modality meant they spent time away from the family, but the overall impact on the family was low because they need not be concerned by the treatment: There has been no impact on my family because praise to God I am still capable enough that the transport comes, takes me and drops me off. So there is no headache as a result of this on my family. (Khadijah, age 56, ICHD)
The majority of the HHD patients considered their modality of treatment to be of benefit to their family because it increased contact with them, whereas ICHD patients were inclined to say that doing HHD would burden the family, causing them to worry and take on extra caring duties: It’s an opportunity to sit and talk to my mum when I go on, she sits with me for about an hour and we talk about the day … probably have a closer relationship with them because of it. (Emma, age 38, HHD) I think they’d (parents) be panicking if the machine gets alarming and stuff like that … they’re getting on a little bit now, you know, to mess about with a new room. (Neil, age 46, ICHD)
Patients spoke about feeling supported in practical ways by their families. Partners tended to be the primary source of support for HHD patients although the level of support patients sought and received varied greatly. While caring partners were a facilitator to undertaking HHD, there were examples of women and men preferring to dialyse when home alone: She (wife) is very, very helpful … sets up all the table … prepares every box for every day … cleans the machine … helps with needling as well, every time she puts the tapes. (Jamal, age 56, HHD) I used to dialyse when (John) was at work on my own, you know, and if there was an emergency you do tend to cope with it on your own because you know what you’re doing, whereas if it’s a family member they sort of say ‘what do you want me do, what do you want me to do’, and they don’t really know what they’re doing. (Joanne, age 53, HHD)
Perceived advantages and disadvantages of HHD and ICHD
Individuals’ perceptions of advantages and disadvantages of each modality varied. All participants agreed: HHD has beneficial effects on health; that it allows independence and that it saved time or allowed time to be used more flexibly. All participants also agreed that ICHD enabled interaction with other patients. However, while most of the hospital samples considered this to be an advantage, the home sample had a more mixed view: Other people don’t know anything about it. We’re a little community here like Martians; it’s all alien to other people. (Joseph, age 75, ICHD) I understand why people go on maintenance in a way, because it’s company. I think if you were living on your own and do it on your own, then going to maintenance where you meet other people would be quite good. (Andrew, age 69, HHD) I felt I am not doing it (dialysis) in the hospital … You can be sat with somebody in exactly the same position as you but their outlook is just very grim, very grim and I just didn’t want that because that in itself can drag you down. (Julie, age 30, HHD)
ICHD and HHD patients perceived ICHD to afford patients with greater access to professional care. For ICHD patients, the lack of professional care at home was a barrier to doing HHD: If my health worsens then the children can’t do anything at home. Like when my breathing stops or if some other problem occurs. Here there are doctors and nurses. (Yusuf, age 56, ICHD)
Home patients, on the other hand, expressed mixed views on this issue. While some favoured the independence and control offered by HHD, others felt isolated at home. Others still, talked about lacking professional support as a challenge only in the context of an emergency situation: I’d rather be at home and be independent and do it myself instead of having to wait around, you know, that part of it just it’s just not me … I don’t like the hospital environment; I don’t like having to rely on people; I don’t like doing things to other people’s times. (Fatima, age 52, HHD) I don’t see a lot of people. I see the nurse, I think, every three months and my home haemo clinic appointments are every six months … yes, I’m probably a good patient, I do look after myself, I don’t have any problems, but you do feel and become very isolated. (Julie, age 30, HHD) The stress of being in control when it’s going wrong and the only one who understands the machine, the only one who can try and work it out … and its beeping and you’re panicking, and you’re trying not to panic and trying to stay calm and you’ve got to do stuff and you can’t … your arm’s immobilised because you’ve got your needles in so you try and do everything at a stretch – I hate that, hate it. (Emma, age 38, HHD)
While both samples acknowledged and weighed up disadvantages of their current modality and advantages of the other modality, they emphasised the basic principle that the modality should match the individual: If you’re an independent person it’s perfect for you. If you feel very needy and don’t feel confident in yourself then it’s probably not for you. (Anna, age 56, HHD) It may help … to mentally test people when they first come into the clinic. To then find out if they are more suited for HHD … sort of screening questions. (Andrew, age 69, HHD)
Practical issues and negotiating haemodialysis
Patients from both samples remarked that dialysis was not a choice since it was a life-saving treatment and as such there needed to be compromise. The compromise patients made depended on what they perceived as most important to them. Of note, both samples highlighted that the HHD machine and its paraphernalia medicalised the home and consumed space: She (wife) was scared of everyone seeing it (dialysis machine). That’s why we don’t invite friends over. (Lee, age 46, HHD) This is a ruthless machine in a home which will give me more stress than here (hospital) … I’m not going to treat you but I’m going to bite you and I will take all your personal life … I will take all your freedom because I am here. Look at me and just start thinking all the time that you are a patient. (Ibrahim, age 36, ICHD)
In contrast to ICHD patients, HHD patients talked about how they overcame barriers: I’ve been fortunate because of where I lived and I’ve been able to create a space which is a dialysis space. I’ve not had it intruding on anything else. (Sarah, age 55, HHD)
Moreover, HHD patients considered disadvantages of their modality to be outweighed by its advantages such as independence and flexibility. This suggests that for some the responsibilities associated with HHD can be offset by the freedom it allows: It’s a pain in the neck because like I’ve got that stuff here that arrived yesterday that’s got to be put away. I’ve got a shed full of stuff outside, I’ve got a room full of stuff there, you know, but I’d rather that than go to the hospital. (Fatima, age 52, HHD)
Discussion and conclusion
Differences in experiences of and views about haemodialysis were observed both within the samples and between them. All patients talked about altered perceptions of self as a result of undertaking haemodialysis. However, the home sample unlike the hospital sample, talked of pushing themselves to manage their condition despite disorientating changes in their identities. The impact of the chosen modality on family and friends was also important.
When talking about perceived advantages and disadvantages of HHD and ICHD, patients acknowledged barriers and facilitators of each modality in contrast to the alternative and were involved in complex cost–benefit analyses. In spite of acknowledging the challenges associated with HHD, for example, personal responsibility and the advantages of ICHD, for example, professional support, the home sample selected HHD as the modality which best suited them. For ICHD patients, the advantages of HHD, for example, the better prognosis were outweighed by their lack of confidence and motivation to take on HHD.
These findings lend support and depth to the findings of a previous survey which had considered barriers to the uptake of HHD and peritoneal dialysis (McLaughlin et al., 2003). That survey noted concerns surrounding the interference with home life brought about by self-care. ICHD participants in this study were conscious of the impact of their modality choice on others. Our work also emphasised the importance of confidence and motivation when making decisions regarding HHD; this reinforced the survey findings of McLaughlin et al. (2003) that a lack of self-efficacy to train and self-care were barriers to home dialysis. Another barrier to HHD reported by the survey was time constraints preventing self-care training and performance of self-care; in contrast, both samples in this study agreed that an advantage of HHD was that it saved time (particularly travel and waiting times) as well as allowing time to be used more flexibly (since they did not need to comply to dialysis slots as in ICHD).
Walker et al. (2015) undertook a recent systematic review of qualitative studies to understand what aspects of HHD deter patients from the treatment despite its association with better survival as compared with ICHD. Two of their three themes were largely confirmed by the HHD patients in this study, that is, ‘vulnerability of dialysing independently’ and ‘fear of being alone’. The theme ‘concern of family burden’ was demonstrated to be a misconception by this study. By emphasising the disconnect (and the similarity) between the lived and the anticipated experience in this way can help inform interventions that approach ‘real’ and ‘perceived’ concerns in different ways.
The discrepancy between challenges experienced by this study’s home sample and the challenges anticipated by the hospital sample reinforce a need for an educational intervention. Peer-led education delivered by expert patients may be one appropriate route, as expert patients would be well placed to share their first-hand experience of HHD. Similar interventions have been successful in other long-term conditions where contact with positive role models has had an additional beneficial effect (Deakin and Whitham, 2009). This is in keeping with the principles of social cognitive theory, which states an individual can acquire knowledge and improve self-efficacy from observing others (Bandura, 2004). However, it is essential to maintain a balanced perspective, so more studies investigating peer-led education in the context of CKD are needed to establish the effectiveness and appropriateness of this approach. The reasons for the lack of confidence and motivation exhibited by ICHD patients are unclear, it may be due to unhelpful beliefs about renal disease and haemodialysis (Theofilou, 2012) or a result of contact with other patients dialysing in-centre; typically, some of whom have more complex needs, for example, due to co-morbidities or old age. It would be useful to pursue this question in future research.
Patients also noted social restrictions resulting from the dialysis regime. In light of this, it may be advantageous to deliver the educational intervention in a group setting which would provide an additional supportive element (Deakin and Whitham, 2009). This would have the potential of providing on-going informal support among familiar group members. The option of including family members would also mean both patients and families would be better equipped to support one another. The important role of families and carers in the context of CKD decision-making has been acknowledged in the wider literature (NHS Kidney Care, 2014).
Health professionals could help patients appraise their situation to decipher which modality least impacts their lifestyle and thereby suits them and their loved ones best. Informed decision-making could be supported by helping the patient explore their reservations. For example, if a patient is concerned about being a burden to the family, the health professional could draw upon this work to highlight that many patients believe it gives an opportunity to strengthen bonds at home. On the other hand, the health professional could also mention ‘real’ barriers, such as feeling isolated at times. This would allow patients to have a clear picture of how the experience of doing HHD would be in practice and which of their concerns are warranted and which might not be.
The major strength of this study was the collection of data from a diverse population of HHD and ICHD patients and the use of framework analysis to systematically map and compare the data from both samples. Each dataset complemented and supplemented the other, thereby producing a comprehensive understanding of the complex issues underpinning the barriers to the uptake and maintenance of HHD.
A limitation was that all ICHD patients were interviewed at hospital, mostly during dialysis and this may have made some patients reluctant to talk frankly about their experiences. However, as patients noted, the nature of their treatment meant they were a time pressured group who found it difficult to participate outside of dialysis time. This limitation was compounded by the fact that despite efforts to sample purposively, the entire study sample was recruited from a single inner-city centre that may not be representative of the dialysis population as a whole.
Conclusion
The disconnect between the lived experience of the home sample and the anticipated experience of the hospital sample suggests that a structured educational intervention could potentially help patients to make informed decisions when choosing a RRT. A suitable way to deliver an educational intervention could be via expert patients sharing both positive and negative personal experiences. The purpose has to be to portray HHD as it is with all the advantages and disadvantages attached so that patients can form a realistic picture of what HHD might entail for them. Delivering an intervention in this way would have the advantage of empowering patients to make informed, individualised decisions about which modality best suits them.
Practical implications
As a robust qualitative CKD study, this work can inform clinical practice (Tong et al., 2014). This research demonstrates that patients choose their RRT by weighing up the pros and cons of the different modalities. The findings also noted a lacking focus on the medical advantages of HHD coupled with a lack of confidence as barriers to HHD. This suggests a need for an intervention that both educates and motivates patients. Existing pre-dialysis education programmes in the United Kingdom vary from trust to trust (O’Donnell and Tucker, 1999). Promoting standardised and individualised education will enable a more informed decision when selecting a RRT, which itself is anticipated to facilitate the uptake and maintenance of HHD.
I confirm all patient/personal identifiers have been removed or disguised, so the patient/person(s) described are not identifiable and cannot be identified through the details of the study.
Footnotes
Acknowledgements
Currie Moore is due our grateful thanks for her invaluable support in collecting data and her considerable help in proof-reading earlier versions of this paper.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by research grants from the Collaboration for Leadership in Allied Health Care Research and Care (CLAHRC) Greater Manchester, UK and the British charity Kidneys for Life.