
Abstract
This study investigated the effects of illness perceptions and coping with disease on health-related quality of life in chronic obstructive pulmonary disease. Therefore, participants (N = 444) completed online questionnaires assessing illness severity (chronic obstructive pulmonary disease stage), Illness Perceptions Questionnaire, coping with disease (Essener Coping Questionnaire), and health-related quality of life (short form-12). Hierarchical regression and moderation analyses were conducted. The results showed that health-related quality of life was predicted by illness perceptions and several aspects of coping with disease. The association between illness perceptions and health-related quality of life was mediated by the corresponding coping with disease subscales. It is concluded that in order to prevent decreasing health-related quality of life in chronic obstructive pulmonary disease, treatment may be adjusted by promoting coping with disease and functional illness perceptions.
Introduction
Chronic obstructive pulmonary disease (COPD) is a progressive disease and mainly characterized by airflow limitation that is not fully reversible (Rabe et al., 2007). Its main symptoms are dyspnea, increased mucus production, and coughing (Vogelmeier et al., 2007). Its prevalence is estimated at about 20 percent in the United States and is steadily increasing (Buist et al., 2007). COPD was on the third rank in the global statistic of disease-related deaths in 2010 (Lozano et al., 2012).
In the last decades, health-related quality of life (HRQoL) has become a major topic of research in the context of chronic illness. It is defined as a rating of the subjective state of health and quantifies the influence of the illness on daily living and well-being. Thus, it is a multifaceted phenomenon, including physical, psychological, and social dimensions (Jones, 1995; Schumacher et al., 2003). Especially in the context of chronic illness, treatment does not only aim at prolonging life expectancy or reducing symptoms, but also at promoting HRQoL (Schumacher et al., 2003). In COPD, HRQoL is substantially impaired across all stages of the disease (Jones et al., 2011, 2012). People suffering from COPD not only report lower HRQoL than those in physically healthy samples and samples from the general population similar in age (Jones et al., 2011; Kühl et al., 2008; Thöne et al., 2011), but also lower HRQoL than patients suffering from terminal lung cancer (Gore et al., 2000; Habraken et al., 2009).
In daily clinical practice, it is particularly valuable to know treatable physiological or psychological factors affecting HRQoL. One relevant factor in the prediction of HRQoL in chronic diseases is coping. According to Lazarus and Folkman (1984), coping refers to cognitive, emotional, and behavioral efforts in dealing with a stressful situation, such as (chronic) illness. While many studies exist on coping and its potential beneficial or adverse relationship with HRQoL in the context of various other chronic diseases (with results still being ambiguous; for example, see Bombardier et al., 1990; Dein and Stygall, 1997; Fritzsche et al., 2007; Kristofferzon et al., 2011; Schipper et al., 2011; Taylor et al., 2008; Wiedebusch et al., 2009), only few studies exist that deal with the influence of coping on HRQoL in COPD. An emotional or avoidant coping reaction seems to be correlated with poorer HRQoL, while a rational coping reaction seems not to be related to quality of life in COPD (Ketelaars et al., 1996). And yet, COPD differs from various other types of chronic illness not only by its severe and fear-evoking symptoms and its progressive lethal course, but above all by its unpredictable disease trajectory due to fulminant exacerbations.
A major disadvantage across studies is that measuring tools are not comparable. More to the point, various studies use instruments measuring coping with stressful events in general and not specifically measuring coping with chronic disease. However, there are differences between coping with stressful events in general and coping with chronic disease. Stressful events are mostly temporarily limited and thus have to be managed in a different way than chronic diseases. While instruments exist that are especially designed for the assessment of coping with disease (Franke et al., 2000; Muthny, 1989), they were not yet considered in the context of COPD.
Another relevant and potentially treatable factor in the prediction of HRQoL is illness perceptions, which have become of particular interest in the last years. Illness perceptions are patients’ subjective cognitions and beliefs concerning their symptoms and disease (Leventhal et al., 1980). Across a wide range of chronic physical health conditions, for example cancer and rheumatoid arthritis, illness perceptions play an important role in the explanation of distress and quality of life outcomes, both in cross-sectional and in longitudinal studies (for a meta-analysis, see Dempster et al., 2015). In COPD, illness perceptions seem to be associated with functioning, disability, depression, anxiety, and quality of life, but it remains unclear whether illness perceptions indeed influence adaptive outcomes via coping (Bonsaksen et al., 2014; Borge et al., 2014; Kaptein et al., 2008; Scharloo et al., 2007; Weldam et al., 2014, Mewes et al., 2015; Zöckler et al., 2014).
Hence, the purpose of this study was to analyze the influence of illness perceptions and coping with disease (assessed by a specially tailored questionnaire) on HRQoL in a sample suffering from COPD, and to examine whether different coping styles indeed mediate the postulated association between illness perceptions and HRQoL.
Methods
Study design and sample
Participants were assessed using an online survey promoted by a self-help organization for COPD in Germany. Participation was voluntary, no financial compensation was offered, and the survey was completed anonymously. Participants were allowed to pause and continue the survey at any time, but they could only continue to the next survey page after completion of every item. The study was approved by the local ethics committee (reference number 2013-36k) and informed consent was obtained from all participants. Data were collected between January 2014 and April 2015. In total, 534 patients with self-reported COPD, who were able to indicate their disease severity (according to the Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2014; stages ranging from I = mild to IV = very severe), took part in the study. After data screening, several participants were excluded due to the following reasons: age < 40 years and thus too young for a valid diagnosis of COPD (n = 10), repeated participation (n = 39), outliers in survey execution time (n = 36), and multivariate outliers in variables used for analyses (n = 5). Thus, the final sample consisted of N = 444 participants.
Measures
Demographics and COPD status-related variables were collected by a self-developed questionnaire including age, gender, marital status, cigarette smoking, disease severity according to GOLD, and time since initial diagnosis.
Illness perceptions were assessed using the Illness Perceptions Questionnaire in its brief version (Brief IPQ; Broadbent et al., 2006). It consists of eight items, which are rated on a Likert Scale ranging from 0 to 10. Each item assesses one dimension of illness perceptions: consequences, timeline, personal control, treatment control, identity, concern, coherence, and emotional representation. A sum score was calculated, with a higher score indicating a more threatening view of the disease. The ninth item assessing subjective causes of the disease by the help of a free text response possibility was not used within this study. To date, the Brief IPQ has been used in a variety of populations differing in age span, illness, and country, and in association with a range of psychological distress and quality of life outcomes. Reliability and validity may be considered as appropriate (Broadbent et al., 2006, 2015). In this sample, internal consistency also was appropriate (Cronbach’s α = .72).
Coping with disease was assessed using the Essener Coping Questionnaire (EFK; Franke et al., 2000). It consists of 45 items, which are rated on a 5-point Likert Scale (0 = not at all, 4 = very strongly). The items load on nine subscales, each with scores ranging from 0 to 20: problem-focused coping (“I deal with upcoming problems, step by step”); distraction and self-confidence (“I encourage myself”); looking for information (“I inform myself about the disease and everything that has to do with it”); trivializing/wishful thinking/defense of threat (“I don’t think about my disease”); depressive coping (“I start to pity myself”); readiness of accepting help (“I accept other people’s help”); looking for social inclusion (“I share quality time with others”); trust in treatment (“I follow the doctor’s instructions”); and development of inner stability (“I start to see a meaning in the disease”). Reliability and validity can be considered appropriate (Franke et al., 2000). In this sample, internal consistency mostly was appropriate (Cronbach’s α ranging from .52 to .83, with rather low scores for the three subscales trivializing/wishful thinking/defense of threat, readiness of accepting help, and development of inner stability).
HRQoL was assessed using the short form 12 (SF-12), a 12-item form of the short form health survey (SF-36; Bullinger and Kirchberger, 1998). It is easy to understand and to complete, especially in an ill and elderly population as it was used in this study. One of the further advantages is the existence of detailed norms, leading to a high comparability across studies. Sum scores of physical and mental HRQoL were calculated, ranging from 0 (worst possible quality of life) to 100 (best possible quality of life) each. Reliability and validity have extensively been confirmed, with similar results for the SF-36 and the SF-12. For the SF-36, internal consistency (Cronbach’s α) ranged from .57 to .94 for subscales (Bullinger and Kirchberger, 1998).
All measures were completed as part of the online survey.
Data analyses
Analyses were conducted with IBM SPSS Statistics for Windows, version 21, and the PROCESS macro (Hayes, 2013).
For preliminary analyses (differences in coping with disease subscales between COPD stages), a multivariate analysis of variance (MANOVA) with post-hoc tests (Games–Howell procedure due to unequal sample sizes and group variances) was conducted.
As main analyses, two hierarchical multiple regression analyses were conducted (outcomes: physical HRQoL and mental HRQoL). Age, gender, time since initial diagnosis, disease severity (first step), illness perception sum score (second step), and coping with disease subscales (third step) were entered as predictors. Assumptions of performing regression analyses were examined beforehand. Multicollinearity was ruled out; all tolerance values were >.20. The values of p used in the regression analyses were two-tailed and considered significant in the case of p < .05.
As additional analyses, two multiple mediation analyses were conducted (outcomes: physical HRQoL and mental HRQoL). The illness perception sum score served as predictor, whereas coping with disease subscales were entered as potential mediators. The analyses were conducted with 1000 bootstrap samples and bias corrected 95 percent level confidence intervals.
Results
Sample characteristics
The final sample consisted of N = 444 participants. See Table 1 for sample characteristics and descriptive results.
Sample characteristics.
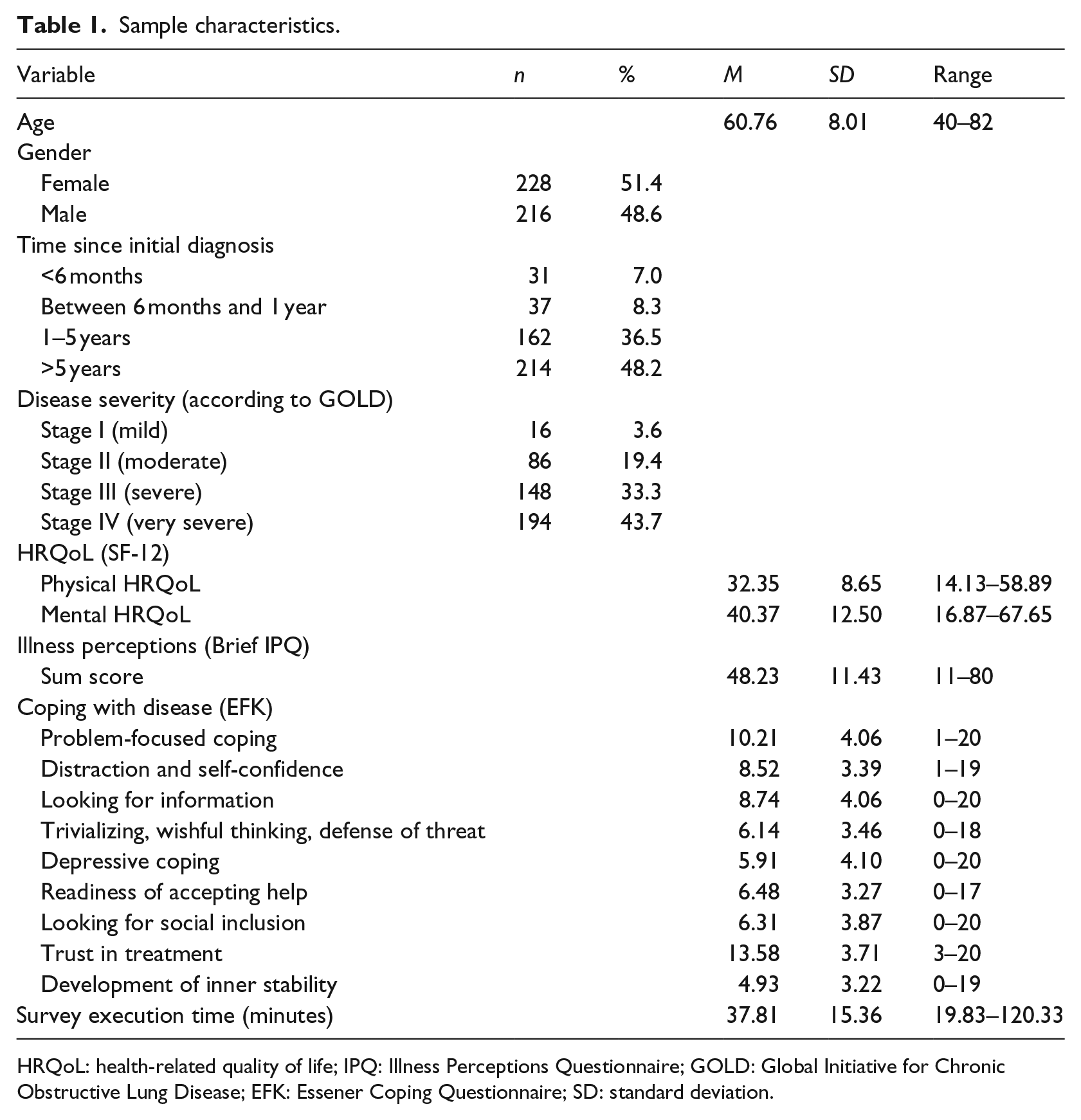
HRQoL: health-related quality of life; IPQ: Illness Perceptions Questionnaire; GOLD: Global Initiative for Chronic Obstructive Lung Disease; EFK: Essener Coping Questionnaire; SD: standard deviation.
Preliminary analyses concerning coping with disease
Differences in coping with disease subscales between COPD stages were analyzed (Figure 1). COPD stages differed only in the subscale readiness of accepting help (F(3, 440) = 2.67; p < .05). Post-hoc tests (Games–Howell procedure) showed a significant increase in readiness of accepting help between GOLD stage II and IV (p < .05; GOLD I: 6.19, GOLD II: 5.88, GOLD III: 6.24, GOLD IV: 6.96).
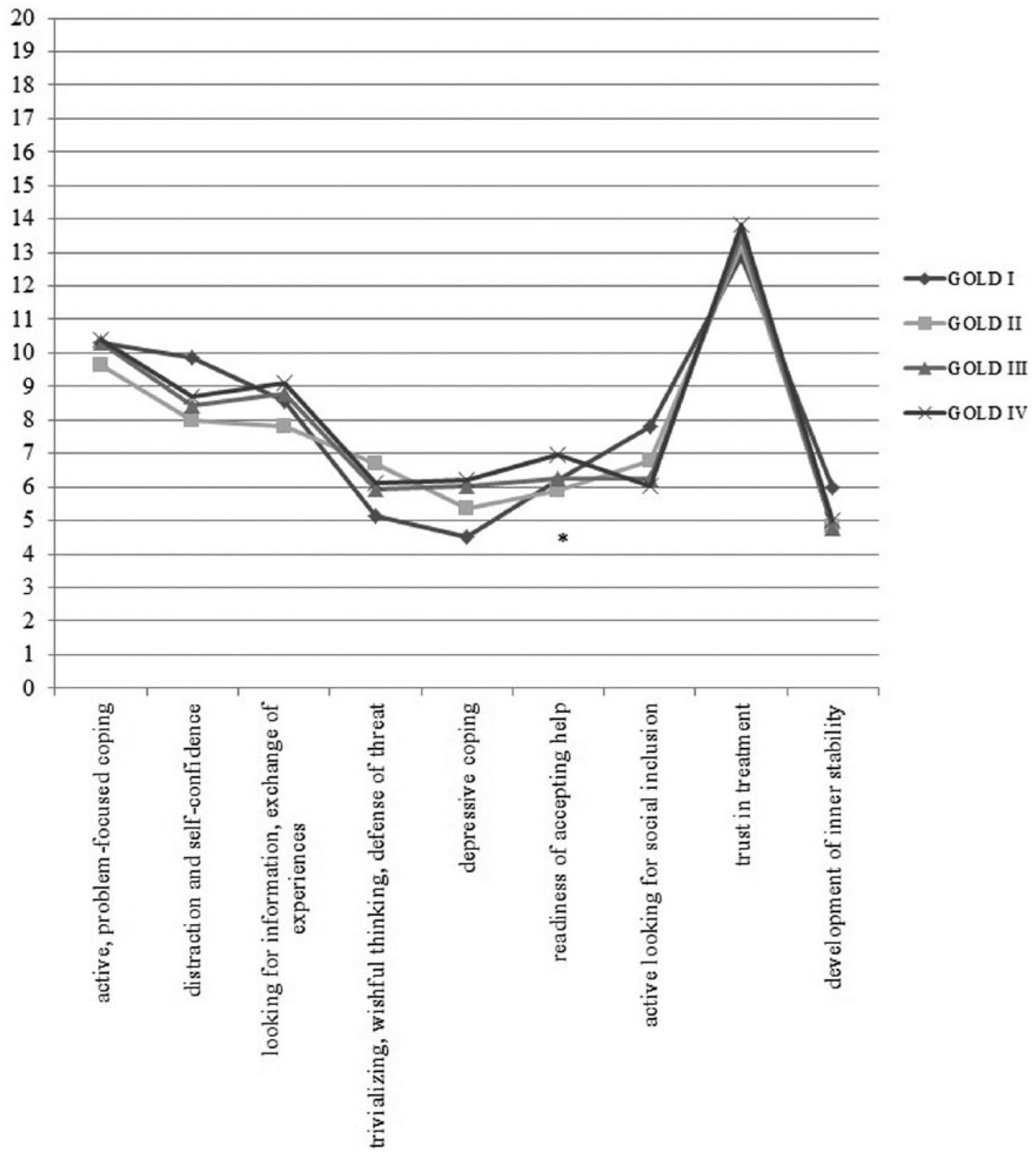
Differences in coping with disease subscales between COPD stages.
Predictors of physical HRQoL
Overall, the model analyzing illness perceptions and coping strategies as predictors of physical HRQoL explained a significant amount of variance, with significant increases in explained variance from step 1 (F(4, 439) = 27.06; R2 = .20; p < .001) to step 2 (F(5, 438) = 53.13; R2 = .38; p < .001), as well as from step 2 to step 3 (F(14, 429) = 23.85; R2 = .44; p < .001). In step 3, age, disease severity, illness perceptions, depressive coping, readiness of accepting help, looking for social inclusion, and trust in treatment were significant predictors of physical HRQoL. Time since initial diagnosis, gender and the other coping with disease subscales did not predict physical HRQoL (Table 2).
Predictors of physical and mental health-related quality of life.
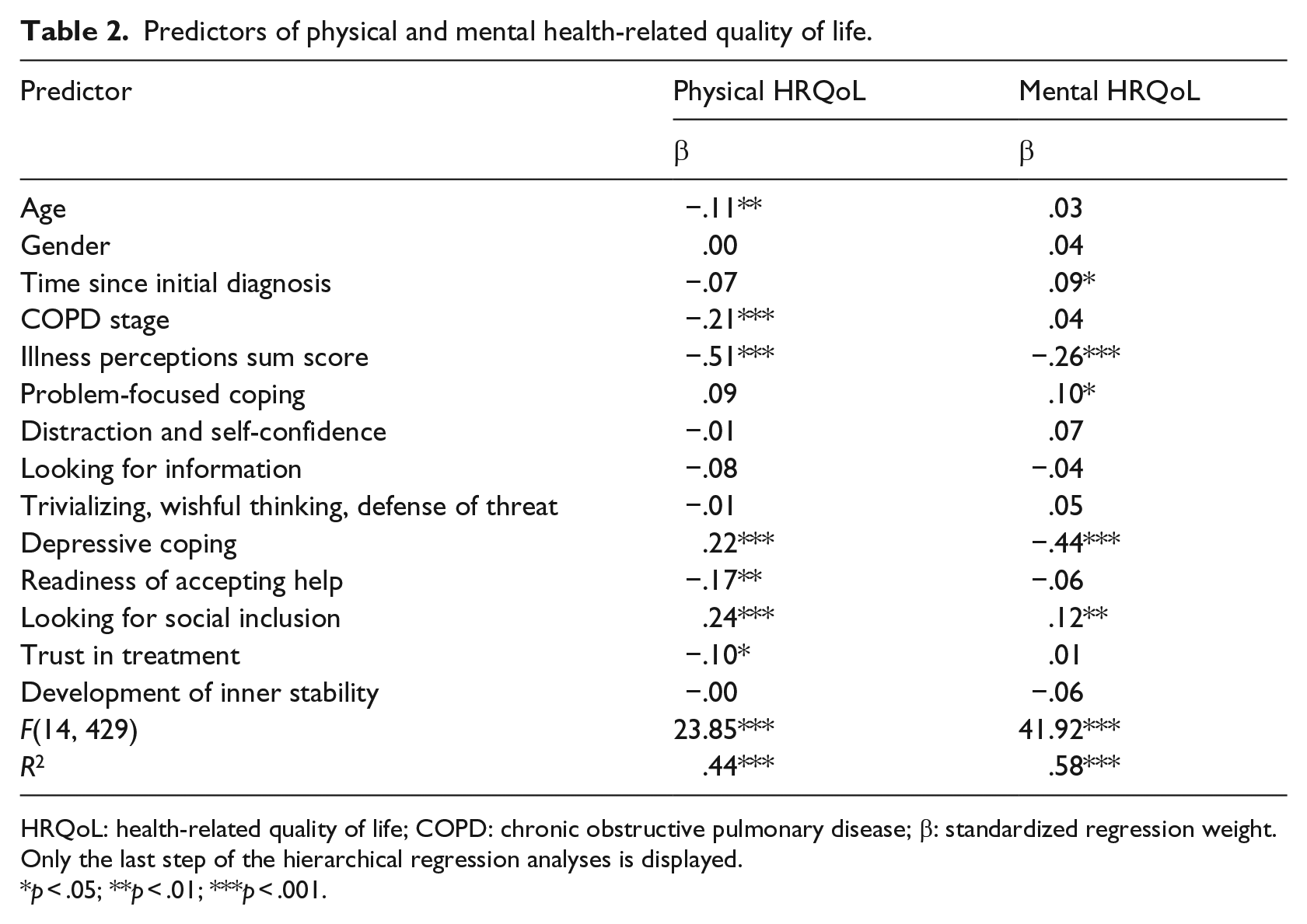
HRQoL: health-related quality of life; COPD: chronic obstructive pulmonary disease; β: standardized regression weight.
Only the last step of the hierarchical regression analyses is displayed.
p < .05; **p < .01; ***p < .001.
Predictors of mental HRQoL
Overall, the model explained a significant amount of variance in mental HRQoL, with significant increases in explained variance from step 1 (F(4, 439) = 6.79; R2 = .06; p < .001) to step 2 (F(5, 438) = 62.63; R2 = .42; p < .001), as well as from step 2 to step 3 (F(14, 429) = 41.92; R2 = .58; p < .001). In step 3, time since initial diagnosis, illness perceptions, problem-focused coping, depressive coping, and looking for social inclusion were significant predictors of mental HRQoL. Age, gender, disease severity, and the other coping with disease subscales did not predict mental HRQoL (Table 2).
Coping with disease as mediator between illness perceptions and HRQoL
Additional multiple mediation analyses showed that some of the coping with disease subscales (those being significant predictors in the hierarchical regression analyses) indeed mediated the association between illness perceptions and HRQoL.
For physical HRQoL, the mediation model explained a significant amount of variance (F(10, 433) = 25.48; R2 = .37; p < .001). Depressive coping, readiness of accepting help, looking for social inclusion, and trust in treatment were significant partially mediating variables in this model (Figure 2).

Mediation analyses concerning physical and mental HRQoL.
For mental HRQoL, the mediation model also explained a significant amount of variance (F(10, 433) = 55.79; R2 = .56; p < .001). Problem-focused coping, depressive coping, and looking for social inclusion were significant partially mediating variables in this model (Figure 2).
Discussion
In this study, differences in coping with disease between COPD stages as well as the influence of coping with disease and illness perceptions on HRQoL were investigated.
Coping with disease across GOLD stages
Differences between COPD stages were found in the coping with disease subscale readiness of accepting help, with a significant increase in readiness of accepting help between GOLD stage II to IV. The items included in this subscale may not only point to an intrinsic readiness of accepting help, but also to the heightened necessity of accepting help. In the light of the progressive course of COPD, it seems comprehensible that patients are readier to accept help or need to accept more help in the higher stages of the disease.
Illness perceptions as predictor of HRQoL
Illness perceptions predicted HRQoL, in the physical as well as in the mental domain, even when controlling for demographics and disease severity. This result is in line with previous research. It was already shown that the different domains of illness representations are associated with physical and psychological aspects of quality of life in other cross-sectional COPD samples (Borge et al., 2014; Mewes et al., 2015; Scharloo et al., 2007; Weldam et al., 2014). There is also some evidence that illness perceptions influence quality of life outcomes after a pulmonary rehabilitation program, at least in the mental domain (Zöckler et al., 2014).
Coping with disease as predictor and mediator
Coping with disease predicted physical as well as mental HRQoL. Hierarchical regression analyses showed that this is the case, even when controlling for illness perceptions. Additional mediation analyses could confirm that the same coping with disease subscales indeed served as mediating variables in the association between illness perceptions and HRQoL.
The result that a higher disease severity predicted worse physical HRQoL is in line with previous research. Jones et al. (2011, 2012) showed that physical HRQoL decreased over the stages of COPD. In this study, readiness of accepting help was also associated with worse physical HRQoL. As was already mentioned, the items of this subscale may also reflect the fact that patients in higher stages of the disease are required to accept help in activities of daily living due to severe dyspnea and the progression of the disease. Thus, it is perhaps the intensification of symptoms, health restrictions and disability that worsens physical HRQoL, and not readiness of accepting help itself. Future studies should distinguish between intrinsic readiness and necessity of accepting help in determining their influence on HRQoL, and also include a measure of activity in daily living in order to gain more detailed insight in relationships between these aspects. Furthermore, patients can be more or less satisfied with the help they receive—a fact that is not addressed in this study and should be taken into consideration in future research. Another coping aspect associated with lower physical HRQoL was trust in treatment. Supposedly, those patients having a high trust in physicians and medication are also those with a mainly somatic explanatory model of the disease, resulting in less self-responsibility and consequently less own efforts to affect their health status and their disease trajectory in a positive way. And yet, engaging in physical training despite dyspnea is a crucial aspect in the prevention of progression of COPD, explaining the result that a high trust in the medical treatment was associated with lower physical HRQoL.
Concerning mental HRQoL, disease severity did not account for a significant amount of variance. Nowadays, it is well confirmed that medical burden is not the only factor associated with functioning in daily living, psychological health, or mental quality of life. Instead, psychological characteristics such as coping also seem to play an important role (for a review, see Hynninen et al., 2005). The result that development of inner stability did not predict mental HRQoL is also in line with previous research. Development of inner stability includes aspects such as praying and looking for consolation in religious faith, accepting the disease as destiny, or recollecting oneself by prayer/meditation. Thus, it assesses positive aspects of religious and spiritual coping. Pedersen et al. (2013) could show that only negative religious coping (interpreting the illness as punishment by God) is associated with quality of life, whereas positive religious coping (looking to God for comfort and support) has no effect on quality of life. The effectiveness of positive religious coping could be due to rituals, adoption of a positive cognitive attitude toward the meaning of the disease (Dein and Stygall, 1997) or re-establishing a certain sense of control (Greenstreet, 2006), but further research in this area is still necessary.
Problem-focused coping was associated with better HRQoL in the mental domain. This result is in line with previous research among patients awaiting lung transplantation, most of them suffering from COPD (Taylor et al., 2008). Active coping includes strategies such as making plans and doing things step by step. With decreasing physical fitness, these strategies become important as activities of daily living must explicitly be planned in order to succeed without severe dyspnea. Hence, active coping is able to increase sense of achievement and mental HRQoL.
In this study, depressive coping was detrimental to physical as well as mental HRQoL. Depressive coping includes emotional reactions such as anger or self-pity, but also rumination and social withdrawal. The association between those reactions and low quality of life is already well documented in various chronic conditions (Fritzsche et al., 2007; Schipper et al., 2011; Wiedebusch et al., 2009) and could now be confirmed in a sample suffering from COPD. In contrast, looking for social inclusion had beneficial effects on both physical and mental HRQoL. This aspect of coping includes activities such as visiting or inviting friends, making new or renewing acquaintances, or helping other people. Thus, it is conceptually different from looking for or getting social support, which is also associated with quality of life, depression, anxiety, and other measures of physical and psychological functioning in COPD (Graydon and Ross, 1995; Grodner et al., 1996; Kara and Mirici, 2004; Keele-Card et al., 1993; McCathie et al., 2002).The feeling of being part of a community and of being loved seems to contribute to HRQoL, independently from the actual support this community is able to give. As the aspect of social inclusion is not yet included in well-established coping questionnaires, it is a new field open to future research.
Limitations
Some limitations of this study should be noted. First, generalizations should be made with caution. On the one hand, the sample was a severely ill one, as patients in stages III and IV according to GOLD were overrepresented. On the other hand, the online recruitment of the sample could have led to a self-selection bias since the promotion for the study took place via the website and mailing list of a support group for COPD in Germany. Nonetheless, there was no financial benefit from participation, and participation was anonymous and voluntary.
Reliability of COPD diagnoses could have been reduced as only participants’ self-ascribing diagnoses and disease severity could be realized within the study design. However, patients being members of the self-help group generally are well informed about pathology, classification, and treatment of COPD. Furthermore, the risk of incorrectly self-ascribed COPD diagnoses and stages of the disease was reduced by asking patients to refer to their physician in case of uncertainty, by adding a “status unknown” option and by excluding participants with unknown disease severity from analyses. Of course, patients did not know that their responses would be excluded from the study if they were not able to indicate their GOLD stage. Thus, their motivation to misstate their disease severity presumably was non-existent or very low.
Second, no causal conclusions can be drawn based on the present cross-sectional data. Thus, future studies should investigate the influence of coping with disease and illness perceptions on HRQoL in longitudinal designs.
Conclusion
In sum, this study illustrated that illness perceptions and coping with disease could be an essential skill for improving HRQoL in COPD. Subsequently, intervention techniques may be adopted. Illness perceptions may be discussed with the help of psychoeducational elements and cognitive reframing of dysfunctional assumptions. Physical activity (as a manifestation of active coping) could be increased by motivating patients to participate in special training programs or in a local lung sports group. Moreover, problem-solving ability could be enhanced by discussing individual treatment goals and possibilities of active cooperation from the patient’s side. Furthermore, it could be helpful to increase feelings of social inclusion, maybe by motivating patients to engage in a support group, either with regular local meetings or with an online forum. Thus, new pathways could open up for the optimization of COPD treatment.
Footnotes
Acknowledgements
We thank Lungenemphysem Deutschland (patient organization), especially Jens Lingemann, for supporting this study. He is the head of this patient organization and provided the link to the online survey on their website.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.