
Abstract
Identifying psychological factors associated with engagement in healthy behaviors in later life is a key to effective behavior interventions. In all, 204 adults (Mage = 80) took a questionnaire assessing objective and perceived health, positive affect and negative affect, aging attitudes, and three classes of health behaviors: eating/nutrition, exercise, and general health behavior. Regression models found better eating behavior was best explained by older age, more exercise was best explained by more positive affect, and better general lifestyle behavior was best explained by worse perceived health. Programs promoting health behaviors in older adults can utilize the findings to tailor interventions to the health behavior of interest.
Engaging in healthy behaviors such as being physically active and consuming a healthy diet is important across the lifespan, but can be especially potent in the context of the physical decline that accompanies aging. Recent work in the area has noted that although there is some clustering of such health behaviors—for example, where people are likely to engage in healthy behaviors across multiple domains or none—there is evidence for considerable variability when it comes to which health behavior(s) a given person will adhere to (Pruchno and Wilson-Genderson, 2012). It is important, therefore, to identify factors that encourage or hinder engagement in different classes of health behaviors in high-functioning older adults, and to use this information to more successfully promote healthy lifestyle choices in this group.
The biopsychosocial model is a broad conceptual framework which acknowledges the reality that biological factors (e.g. age, physical health), psychological factors (e.g. emotions, perceptions, attitudes), and social factors (e.g. social support and community resources) all contribute to the development of a given characteristic or engagement in a given behavior. In the present context—health behavior in older adults—primary emphasis is placed on psychological factors because research indicates that older adults tend to prioritize emotional goals and psychological experience as they age (Carstensen and Mikels, 2005), which makes psychological factors potential targets for intervention even for those who are experiencing age-related declines in the biological and social arenas (e.g. physical morbidity, passing of partner or peers). Because previous research has found poorer perceived health and perceived health competence (Burton et al., 1999; Dogra and Stathokostas, 2014), as well as more negative affect tendencies and more negative attitudes toward aging (Chaves and Park, 2015; Chen, 2010; Lees et al., 2005; Levy and Myers, 2004) to be associated with reduced engagement in healthy behaviors known to reduce morbidity and mortality risk, we have chosen to test which of these factors—positive and negative affect (PA/NA), perceived health, and aging attitudes—is the best predictor of different classes of health behaviors. In recognition of the importance of the other components of the model, the biological factors of age and health, which have been found to influence the extent which an individual will exercise (Burton et al., 1999; Chen, 2010) and eat healthfully (Dijkstra et al., 2014), along with the social factor of living situation (community-dwelling vs in senior living facilities), are accounted for in the analytic models.
As noted above, the primary aim here is to investigate whether there are differential effects of the predictors, or if the associations are uniform regardless of behavior type. The three health behavior outcomes of interest are eating behavior/nutrition, exercise behavior, and general lifestyle behavior (e.g. smoking, flossing, and seatbelt use). This breakdown not only fits with intuitive categories of health behaviors in the popular realm (e.g. Mendes, 2009), but also aligns with the majority of the literature on health behaviors, which tends to focus on either physical activity, diet/nutrition, or health behaviors in general (as evidenced, for example, in the review by Lee et al., 2010). This differential analysis will contribute to the existing literature by identifying whether there are certain psychological targets that will be effective for promoting one class of health behaviors in older adults but perhaps not another. Based on the evidence cited above, hypotheses are that more PA, less NA, better perceived health, and more positive aging attitudes will be associated with more engagement in healthy behaviors.
Methods
Participants and procedure
Participants were 204 adults aged 60–98 years (M = 80.02, standard deviation (SD) = 8.97) recruited in person from five senior centers (N = 104) and two senior living facilities (N = 100). The majority of the sample is female (74.5%) and Caucasian (91%), and income is fairly normally distributed: 4 percent earn ⩽$10k annually, 27.5 percent make >$10k and ⩽$25k, 42 percent make >$25k and ⩽$50k, 17 percent earn >$50k and ⩽$75k, and 9.5 percent bring in more than $75k. All participants had at least a high school education, and 42.5 percent had a college degree. Considering marital status, 48 percent were widowed, 32 percent were married or partnered, and 20 percent identified as divorced or single.
Participants completed a 14-page questionnaire at their convenience and returned it in a postage-paid return envelope. The return rate was 55 % three returned surveys were not included in the analysis due to indicators of cognitive impairment demonstrated during the in-person recruitment or through inappropriate responding on the survey indicating a lack of understanding. All participants who returned a survey were entered into a drawing to win one of five $100 universal gift cards. Informed consent was obtained from all participants and procedures were approved by the Institutional Review Board at the University of Michigan–Dearborn.
Measures
Objective health
Objective health was assessed using a checklist of diagnoses (nine conditions and an “other” option) coded as a count variable so that individuals received a score equal to the number of conditions checked (0–10). Higher scores indicate poorer objective health (M = 1.69, SD = 1.71).
Perceived health
Perceived health was measured using four items. The items In general, how would you rate your overall health? and Compared to others your age, how would you rate your overall health? were rated on a 5-point scale (excellent to very poor); participants then marked whether or not (yes/no) they felt their health had improved or declined over the past year. These four items were standardized (M = 0, SD = 1) and summed to form a composite perceived health variable; all items were coded so that higher scores indicate worse perceived health (M = −0.02, SD = 2.96).
Affect
The original Positive and Negative Affect Scale (PANAS; Watson et al., 1988) assessed PA and NA; 10 negative (e.g. afraid, irritable) and 10 positive (e.g. inspired, enthusiastic) terms were rated on a 5-point scale (1 = not at all, 5 = extremely) indicating the extent that participants felt each emotion in general. Higher scores indicate higher NA (M = 14.52, SD = 4.91) and PA (M = 37.62, SD = 6.98). Reliability in our sample was high: αPA = .91, αNA = .87.
Aging attitudes
Participants’ attitudes toward their own aging were assessed via the Attitudes Toward Own Aging scale (ATOA; Liang and Bollen, 1983). The scale consists of five items such as Things keep getting worse as I get older and I am as happy now as when I was younger; respondents note whether they agree or disagree with each statement. Three of the five items are reverse-scored so that higher scores indicate more positive aging attitudes (M = 8.07, SD = 1.66; α = .71).
Health behaviors
All health behavior items were rated on a 5-point scale (never to daily), standardized (M = 0, SD = 1), and summed to form the three composite health behavior variables so that higher scores indicate more healthy behaviors. Eating behavior/nutrition (M = −0.03, SD = 1.92) was assessed using three items: I eat healthfully, I drink about 8 cups of water in a day, and I take vitamins. Exercise behavior (M = 7, SD = 3.16) was assessed using three items: I do exercises intended to improve muscle strength, I do exercises intended to improve aerobic capacity, and I do exercises intended to improve flexibility or balance. General lifestyle behavior (M = −0.02, SD = 2.04) items assessed smoking, alcohol consumption, sleep, flossing, and seatbelt use.
Results
Descriptive statistics
The only correlation among the dependent variables was between eating/nutrition and exercise behavior (r = .3), indicating that they represent largely independent outcomes. The psychological variables were all moderately correlated with one another (p < .01). Those living independently in the community tended to be younger than those in a senior living facility.
Analytic results
Multiple regression was used to test the hypotheses; regression models were run in two phases for each dependent variable: Model 1 included the covariates (age, objective health, and living situation), and Model 2 added the four subjective predictors (perceived health, PA, NA, and aging attitudes). Table 1 shows results.
Regression models on health behavior variables.
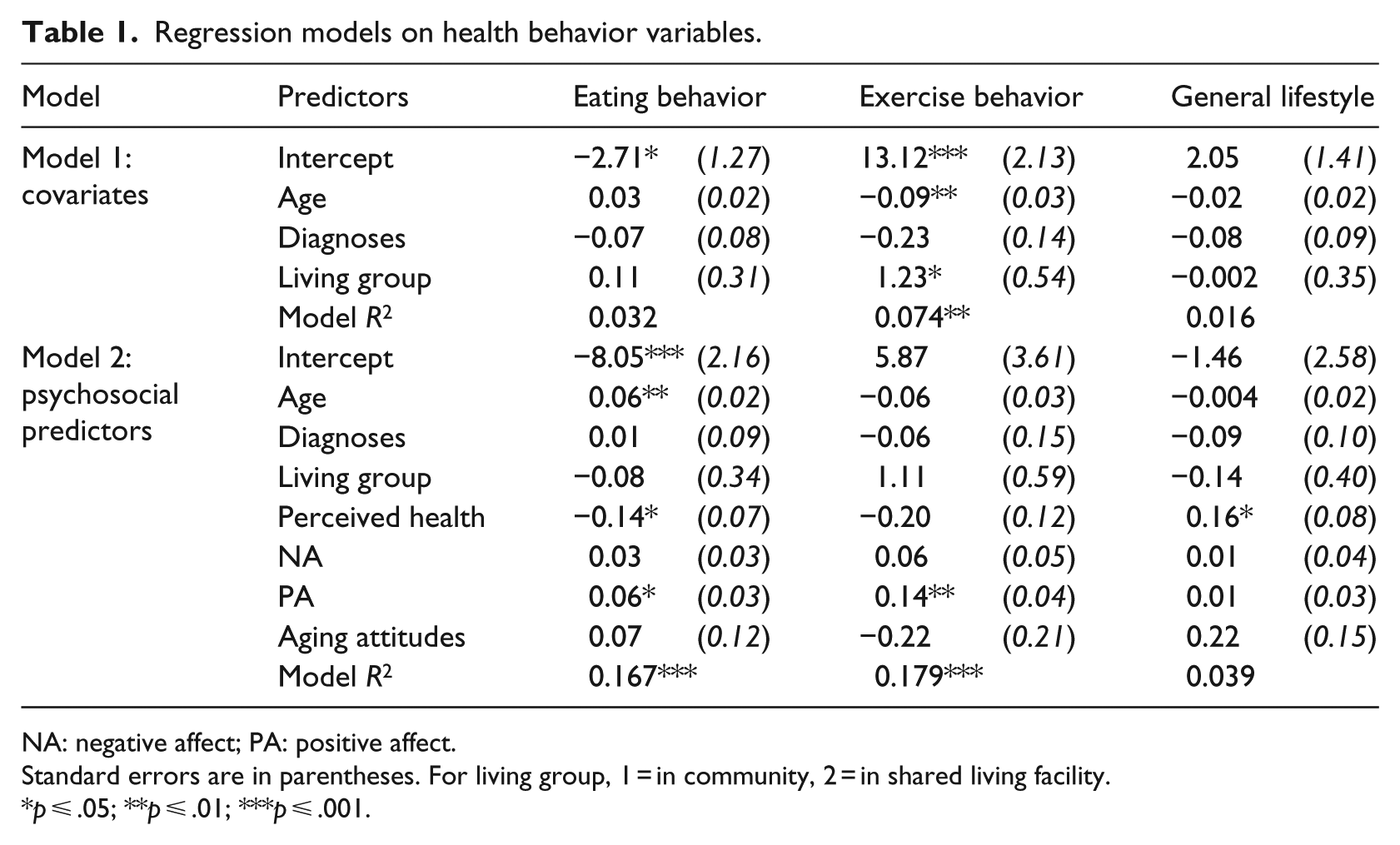
NA: negative affect; PA: positive affect.
Standard errors are in parentheses. For living group, 1 = in community, 2 = in shared living facility.
p ⩽ .05; **p ⩽ .01; ***p ⩽ .001.
Model 1 on eating/nutrition reveals no significant effects for the covariates; however, a significant effect emerges for age (p = .002) in Model 2 so that those who are older tend to report healthier eating habits. This aligns with the positive correlation between age and eating/nutrition (r = .17, p = .02). The effects of perceived health (p = .04) and PA (p = .026) are also significant so that seeing oneself as healthier and experiencing more PA are both associated with healthier eating habits.
Model 1 on exercise behavior shows significant effects for age (older individuals report less physical activity; p = .002) and living situation (those in shared living facilities report more physical activity; p = .024). Once the psychosocial predictors are added in Model 2, however, the significant covariate effects that existed in Model 1 become non-significant, and the effect of PA comes to the fore (p = .001).
The only significant effect that emerged in either model predicting general lifestyle behavior was that for perceived health (p = .038) so that seeing oneself as less healthy was associated with better general health behaviors such as flossing and seatbelt use.
Neither NA nor ATOA had significant effects on any of the health behavior outcomes. The lack of ATOA effects is likely a result of its high correlation with perceived health (r = .59).
Discussion
Overall, results align with previous research, and provide evidence for differential associations among the subjective predictors and the behavior outcomes: exercise behavior was best explained by PA, eating/nutrition was best explained by age (although PA and perceived health also had effects), and general lifestyle behavior was best explained by perceived health. Referring back to the biopsychosocial model, the results highlight that although biological factors such as age and social factors such as living situation do affect adherence to healthy behaviors, factors in the psychological domain tend to emerge as the strongest contributors in high-functioning older adults. Presuming directionality can be established by future studies utilizing longitudinal methods, these results provide a potential guideline for those developing programs or interventions aimed at increasing health behaviors in high-functioning older adults, identifying targets depending on the health behavior of interest.
For exercise behavior, we find evidence that PA serves to mediate, or explain, the initial effects of age and living situation; considering the correlations, it appears that it is not being older that best explains exercise behavior, but rather the fact that PA declines with age in this sample, and that higher PA is associated with more physical activity. In the case of eating/nutrition, the fact that age had the greatest effect suggests that younger seniors (<75 years) may be more in need of education or intervention in the area of healthy eating than are “old-old” seniors (75+ years). This effect may be mirroring the finding of Dijkstra et al. (2014) that older adults with poorer health tend to be motivated to eat healthier by their disease state. PA and perceived health are also potential intervention targets for improving eating behaviors, as having higher levels of each of these was linked with healthier eating.
These findings can be applied in order to promote senior engagement in exercise and healthy eating. In the case of PA, perhaps older adults could be asked to consider what they most enjoy about their lives right now (being grandparents? having time for hobbies?), and reminded that eating more healthfully and remaining physically active will likely enable them to enjoy those things for longer. Or for perceived health, seniors could be asked to take stock of all that they can do physically (thereby improving their perceived health), rather than focusing on limitations they may be experiencing; the program could then emphasize that engaging in healthy behaviors is one of the best ways to maintain these abilities and delay physical decline.
The results for the general lifestyle behavior outcome—that perceiving one’s health as worse is linked with more healthy lifestyle behaviors—is opposite of what has been found previously for other health behaviors (e.g. Burton et al., 1999; Dogra and Stathokostas, 2014). Because of this and the fact that there was no significant correlation between these two variables, the effect must be interpreted with caution until it has been replicated. However, should the finding be valid, it would suggest that these general health practices—which arguably require less mental effort, fewer financial resources, and less physical capability than maintaining a healthy diet or engaging in physical exercise—are even more salient to older adults who perceive themselves to be less healthy. That is, perhaps when an individual no longer feels they can successfully engage in or benefit from healthy diet or exercise behaviors, they are more motivated to engage in more general (and more accessible) health behaviors such as flossing and wearing a seatbelt. Considering this from an applied perspective, facilitating engagement in these general lifestyle health behaviors in older adults who are limited by mental or physical health may improve self-efficacy and make them feel healthier, thereby improving overall well-being.
There are naturally limitations to these findings. First, the at-home survey completion approach is more error-prone than interviews or surveys completed in the presence of the researcher; in order to limit error in the data, all returned surveys were checked for compliance with instructions. Second, generalizability is limited based on the convenience nature of recruitment and the resulting high-functioning sample; however, the participants are fairly normally distributed on income, and the makeup in terms of gender and race is reflective of the older population in the United States, which is primarily female and Caucasian. This study therefore provides a significant addition to the literature in the area by demonstrating how important the psychological domain is when it comes to engagement in healthy behaviors in high-functioning older adults, as well as how different dimensions of health behaviors may be associated with different psychological factors in this group. Future work utilizing more varied samples, a broader range of specific health behaviors, and longitudinal methods will build on the current findings and establish more precise targets for programs aimed at promoting health behaviors and long-term quality of life in older adults.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.