
Abstract
We examined the evolution of the subjective burden of romantic partners caring for women with non-metastatic breast cancer and investigated the moderating role of couple satisfaction on caring stress. Forty-seven partners filled out questionnaires 3 and 12 months after surgery. Using a stress process model, we examined caring stressors and moderating factors (couple satisfaction, coping and social support) as predictors of subjective burden. Results showed that subjective burden decreases over time and that the couple satisfaction largely explains it above and beyond other influential variables. Partners dissatisfied with their couple relationship are especially vulnerable to the stress of caregiving.
Introduction
Breast cancer is the most common cancer among women (Bray et al., 2004). An international epidemiological study showed that its incidence rose by 30%–40% worldwide from the 1970s to the 1990s (Althuis et al., 2005). The growing need for assistance and care for patients, and the impossibility for public health to face this increasing demand, has progressively shifted the burden of patient care from hospitals to informal caregivers (Feldman and Broussard, 2006). The term ‘informal caregiver’ is used in the literature to define a person from the close environment (e.g. partner, adult child or other relatives, friends and neighbours) who does not possess any training in health or psychological care and who provides unpaid care for the patient (Carretero et al., 2009). In most cases, the romantic partner is the principal relative involved in this role (Li et al., 2013).
The partners of women with breast cancer are in charge of providing emotional support and helping the woman to manage her negative emotions such as despair, fear and sadness (Bozo et al., 2009; Lethborg et al., 2003). Caregiving also implies assuming the management of the home and children (if any), while assisting the woman in the daily management of her disease and continuing to carry out work and social commitments (Bakas et al., 2001; Bigatti and Wagner, 2003). The role of informal caregiver thus includes multiple responsibilities.
In the literature, this set of care tasks was referred to as an ‘objective burden’, which is distinguished from the ‘subjective burden’, defined as the feeling of intrusiveness and disruption of the illness and caregiving in caregivers’ lives (Zarit et al., 1980, 1986). Studies showed that the subjective burden (in general measured in terms of the caregiver’s subjective perception of the impact of caregiving on his or her life in different domains) is a strong predictor of caregiver’s quality of life and psychological well-being, over and above the objective burden (in general measured in terms of the number of hours the caregiver spends on caregiving and the number and kinds of tasks he or she is in charge of) (Braun et al., 2007; Haley et al., 2003).
To date, empirical investigations on the informal caregiver of the cancer patient are still relatively rare and mostly focused on advanced, metastatic and palliative stages of cancer (e.g. Braun et al., 2007; Grunfeld et al., 2004). Existing data show that in these situations, caregiving is significantly linked with decreased psychological and physical well-being of the caregiver, with problems such as depression, anxiety, excessive fatigue, sleep disturbance and chronic pain. Between 20% and 30% of caregivers meet the criteria for a psychiatric diagnosis (Baronet, 1999; Li et al., 2013; Pitceathly and Maguire, 2003; Stenberg et al., 2010).
Few studies have so far investigated the impact of non-metastatic breast cancer on romantic partners in terms of caregiver burden (e.g. Lopez et al., 2012; Wagner et al., 2011). Moreover, the evolution over time of the caregiver burden has rarely been studied, although it is known that the care tasks, the burden felt by the caregiver and his well-being may fluctuate following possible changes in the patient’s health (Nijboer et al., 1998; Stenberg et al., 2010). Evolution over time is all the more important to consider when studying non-metastatic breast cancer, where the medical condition of the patient can rapidly change following the treatment phase and where, in most cases, patients enter a rehabilitation phase after a relatively short period. In this context, the caregiver’s subjective burden may also rapidly change in accordance with the medical condition of the patient.
In order to understand the caregiver burden, we referred to the stress process model (Pearlin et al., 1990; Yates et al., 1999), which has been widely used to identify risk and protective factors for caregivers’ well-being. According to this theoretical model, the objective burden (i.e. illness-related factors) and the background and context characteristics of the caregiver (i.e. gender, age, ethnicity, socio-economic status and biopsychosocial history) are at the origin of the subjective burden. Caregivers have personal and social resources that act as protective factors and consequently moderate the effect of the stressors on possible negative outcomes. Individual coping and social support (i.e. specific instrumental and emotional support that the caregiver may receive from his close environment in the context of the illness) are the most studied resources to explain modulations in the caregiver burden in a variety of illnesses such as cancer, dementia or spinal cord injury. Studies have shown that efficient coping and support are both related to a lower subjective burden and better psychological adjustment (Chiou et al., 2009; Papastavrou et al., 2009; Rodakowski et al., 2012). Surprisingly, the general quality of the relationship between the caregiver and the patient has rarely been taken into account. In non-cancer diseases, a few studies have nevertheless shown that the caregiver’s satisfaction with the relationship was significantly linked to the subjective burden: the higher the quality of the relationship, the lower the perception of burden (Quinn et al., 2009; Snyder, 2000; Steadman et al., 2007; Williamson and Shaffer, 2001). A recent study on caregivers of cancer patients entering home hospice care found that the relationship quality significantly predicted the spousal caregiver burden (Reblin et al., 2015). These findings strongly support taking into consideration the quality of the relationship in a model of stress and coping in caregiving for non-metastatic cancer patients.
The first aim of this study was to assess the subjective burden of partners of women with non-metastatic breast cancer and its evolution over time. We thus considered two different phases: the active treatment phase (3 months post-surgery; T1 in the research design) and the rehabilitation phase (12 months post-surgery; T2 in the research design). We hypothesized that the subjective burden would decrease when patients enter the rehabilitation phase (i.e. end of active treatment). The second aim of this study was to examine the unique contribution of couple satisfaction to the subjective burden of romantic partners of women with non-metastatic breast cancer. We hypothesized that higher couple satisfaction would be associated with a lower subjective burden at both assessment points. In accordance with the stress process model, we tested this hypothesis using the socio-demographic data of the partner as the background and context factors and using the medical and psychological conditions of the patient as the primary stressor (i.e. objective burden). We also considered individual coping, social support and couple satisfaction as resources that may moderate the effect of caregiving stress and protect the partner from the subjective burden.
Methods
Participants
Patients and their romantic partner were recruited from the Senology Unit of the University Hospital of Lausanne (Switzerland). Eligibility criteria for patients were the following: diagnosis of breast cancer, breast surgery required (mastectomy or lumpectomy), ability to speak and read French and being engaged in a couple relationship. Eligible romantic partners were aged ⩾18 years and were able to speak and read French. The study was proposed to 127 women: 97 (76.4%) agreed to participate and to ask their romantic partner to participate as well. Sixty-one partners (62.9%) agreed to enter the study. Seven partners dropped out of the study at T2 (attrition rate of 11.5%). Seven partners were then excluded from the analyses because of missing data in the main variables. In order to compute analyses on the same participants at both time points, we selected a final sample of 47 partners who completed all the questionnaires.
Concerning the socio-demographic data of the romantic partners, their mean age was 53.7 years (standard deviation (SD) = 12.3) and their socio-economic level was mainly (80.9%) middle to upper class (Hollingshead Index of Social Position). The majority of them lived with the patient (91.5%) and were married to her (63.8%). The mean length of their couple relationship was 24.7 years (SD = 16.0). Only a minority of partners (19.1%) had children younger than 18 years old in the household. Concerning the patient’s oncological diagnosis, 10 (21.3%) had been diagnosed with in situ breast cancer and 37 (78.7%) with invasive breast cancer (38.3% stage I, 29.8% stage II and 10.6% stage III). For type of surgery, 55.3% of the women underwent mastectomy, 44.7% lumpectomy and 29.8% axillary lymph node dissection (ALND). At T1 (3 months post-surgery), 27.7% were undergoing chemotherapy, 55.3% radiotherapy and 61.7% hormonal therapy. At T2 (12 months post-surgery), no women were undergoing chemotherapy, only 1 woman was undergoing radiotherapy and 80.9% of the women were undergoing hormonal therapy.
Procedure
Recruitment took place between September 2011 and December 2013. The referent nurse of the Senology Unit proposed during pre-hospital consultation (1–2 weeks before surgery) that the women take part in the research. Patients and their romantic partners received documentation on the research and signed an informed consent form. Couples were asked to complete a set of self-reported questionnaires at home at both time points. Two self-addressed stamped envelopes (one for the patient and one for the partner) were provided to participants, with the instructions to send the completed questionnaires to the referent nurse within a month. The study was approved by the Ethics Committee of the University Hospital of Lausanne in July 2011.
Measures
The Brief Symptom Inventory-18 (BSI-18; Derogatis, 2001) was used to measure the psychological distress of the patient. Eighteen items assess symptoms along three dimensions: depression, anxiety and somatization (six items by dimensions). Each item is rated on a 5-point Likert scale from 0 (not at all) to 4 (very much). A summary score of psychological distress is computed as the sum of the 18 items (α T1 = .93; α T2 = .92). This score ranges from 0 to 72: the higher the score, the higher the psychological distress.
A short-form version of the Zarit Burden Interview-12 (ZBI-12; Bédard et al., 2001) was used to measure the romantic partner’s subjective burden. This instrument consists of 12 items that are scored on a 5-point Likert scale ranging from 0 (never) to 4 (nearly always). A summary score is computed by calculating the sum of the 12 items (α T1 = .83; α T2 = .77). This score ranges from 0 to 48: the higher the score, the greater the subjective burden perceived by the romantic partner.
The revised version of the Individual Coping Questionnaire (INCOPE-2R; Bodenmann, 2000) was used to measure coping. This instrument consists of a set of 21 items that describe different cognitive, emotional and behavioural reactions that people may adopt when facing a stressful situation. Each of the 21 items is rated on a 5-point Likert scale ranging from 1 (never) to 5 (always). Items can be grouped into two main categories: functional and dysfunctional coping. A summary score is computed as the mean of the functional coping score and the inverse of the dysfunctional coping score. This score ranges from 1 to 5: the higher the score, the higher the use of functional coping and the lower the use of dysfunctional coping (α T1 = .80; α T2 = .76).
A short-form version of the Social Support Questionnaire-6 (SSQ-6; Sarason et al., 1987) was used to assess satisfaction with perceived social support. This questionnaire contains six questions about social support in diverse domains; romantic partners were asked to rate their satisfaction with the support received in each domain on 6-point Likert scales. A summary score of satisfaction was computed by calculating the mean of the six questions (α T1 = .95; α T2 = .90). This score ranges from 1 to 6: the higher the score, the more the partners were satisfied with perceived social support.
The Relationship Assessment Scale (RAS; Hendrick, 1988) was used to measure relationship satisfaction of the romantic partner. Each of the seven items is scored on a 5-point Likert scale from 1 (low satisfaction) to 5 (high satisfaction). A summary score is computed by calculating the mean of the seven items (α T1 = .91; α T2 = .92). This score ranges from 1 to 5: the higher the score, the higher the partner’s satisfaction about his couple relationship.
A questionnaire specifically designed for the study was used to collect the socio-demographic and medical data.
Results
Descriptive statistics for the study variables
Concerning the partner’s level of subjective burden, the mean total score of the ZBI-12 was 9.5 (SD = 5.3) at T1 and 8.1 (SD = 5.3) at T2.
Concerning the partner’s resources (i.e. individual coping, social support and couple satisfaction), the mean total score of the INCOPE-2R was 3.6 (SD = 0.3) at T1 and 3.7 (SD = 0.3) at T2, indicating that partners generally use more functional than dysfunctional individual coping. The mean total score of the SSQ-6 was 5.4 (SD = 0.9) at T1 and 5.4 (SD = 0.6) at T2, indicating an overall high level of satisfaction with perceived social support. Finally, the mean total score of the RAS was 4.5 (SD = 0.5) at T1 and 4.5 (SD = 0.7) at T2, indicating that couple satisfaction in our sample was fairly high.
Concerning the patient’s psychological distress, the mean total score of the BSI-18 was 14.3 (SD = 13.8) at T1 and 11.2 (SD = 9.0) at T2.
Change in subjective burden over time
In order to test our first hypothesis, we compared the mean total score of the ZBI-12 at T1 and T2. The results showed a statistically significant difference (t(46) = 2.15; p = .037; paired t test): the level of subjective burden reported by the romantic partner decreased between 3 and 12 months post-surgery.
Couple satisfaction as predictor of subjective burden
Preliminary checks
We assessed first which background and context factor (socio-demographic data of the partner) and primary stressors (medical and psychological conditions of the patient) were associated with subjective burden (see section ‘Participants’ for details about socio-demographic and medical data). The level of subjective burden at T1 was significantly correlated (Pearson’s correlation) with the romantic partner’s age (r = −.42; p = .003), whether the patient underwent ALND (r = .37; p = .012) and the patient’s psychological distress (r = .49; p < .001). These three variables were thus selected and introduced into the regression models as predictors of subjective burden at T1. At T2, no socio-demographic or medical variable was significantly correlated with the subjective burden. Accordingly, none of these variables were tested in the regression model.
Bivariate links between study variables
Results of Pearson’s correlations showed that, according to our second hypothesis, the partner’s couple satisfaction was strongly associated with the level of subjective burden at T1 (r = −.76; p < .001) and T2 (r = −.68; p < .001): the higher the couple satisfaction, the lower the subjective burden reported by the partner. At T2, but not at T1, satisfaction with perceived social support was also related to subjective burden: the higher the satisfaction with social support, the lower the subjective burden (r = −.39; p = .006). No significant association was found between subjective burden and individual coping at either T1 or T2.
Predictors of subjective burden
Two hierarchical multiple regression analyses were performed to examine the role of couple satisfaction in determining the subjective burden at T1 and T2 (see Table 1). Results at T1 showed that age, which was entered at step 1, significantly explained 18% of the variance of subjective burden: the younger the partner, the higher the subjective burden. The medical and psychological condition of the patient (i.e. ALND and psychological distress) introduced at step 2 accounted for a significant additional 26% of the variance of subjective burden: patients having undergone ALND (β = .36; p < .01) and patients having a higher level of psychological distress (β = .40; p < .01) both significantly induce a higher level of subjective burden. Couple satisfaction, individual coping and social support, introduced at step 3, added a significant additional 29% of the variance, but only the effect of couple satisfaction was significant (β = −.61; p < .001): the higher the couple satisfaction, the lower the subjective burden. The variables that stayed significant at step 3 were ALND, the patient’s psychological distress and the partner’s couple satisfaction. This final model explained 72% of the variance of subjective burden.
Hierarchical multiple regression analysis predicting romantic partner’s subjective burden at T1 and T2 (n = 47).
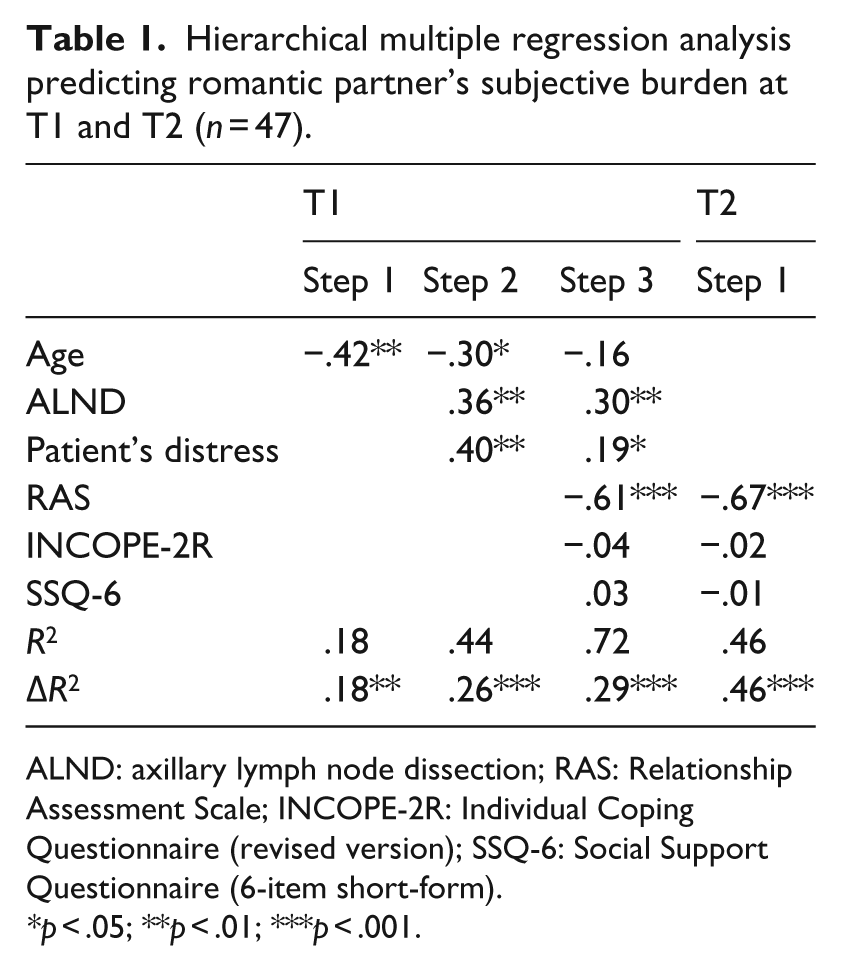
ALND: axillary lymph node dissection; RAS: Relationship Assessment Scale; INCOPE-2R: Individual Coping Questionnaire (revised version); SSQ-6: Social Support Questionnaire (6-item short-form).
p < .05; **p < .01; ***p < .001.
At T2, couple satisfaction, individual coping and social support were introduced at step 1, but only couple satisfaction was a significant predictor of subjective burden (β = −.67; p < .001): the higher the couple satisfaction, the lower the subjective burden. The model explained 46% of the variance of subjective burden.
For all regressions, residual analyses revealed no outliers, homoscedasticity and normality of residuals. Predictors were not multi-collinear.
Discussion
In this study, we assessed the subjective caregiver burden in male partners of women with non-metastatic breast cancer. The aims of the study were, on one hand, to assess the subjective burden and its change over time and, on the other, to examine the contribution of couple satisfaction in moderating the impact of caregiving stress on the partner’s subjective burden.
The majority of romantic partners reported a subjective burden 3 months (i.e. active treatment phase, T1) and 1 year (i.e. rehabilitation phase, T2) after surgery; in accordance with our hypothesis, subjective burden was significantly lower at T2. Results from multivariate analyses offer some details to better understand this decrease over time. During the active treatment phase, the patient’s medical and psychological conditions were significant predictors of subjective burden. Indeed, we found that ALND and the patient’s psychological distress explained approximately 26% of the variance of subjective burden at T1. The negative impact of ALND may be explained in terms of an increase in the patient’s physical impairment. This type of surgery may indeed induce several side effects such as pain, swelling, weakness and trouble moving the arm, but also more severe problems such as lymphoedema (Swenson et al., 2002). Patients are thus often debilitated, preventing the use of their arm, and became more dependent on the practical help of their partner. This result was in line with other studies showing that increased physical impairment in a patient is linked to greater caregiver burden (Pinquart and Sörensen, 2003). The link between the patient’s distress and the partner’s subjective burden was not surprising. The literature has indeed shown that among the many tasks that the informal caregiver must assume, providing emotional support proved to be the most time-consuming and difficult (Bakas et al., 2001; Carey et al., 1991). In contrast, at T2, no significant link was found between subjective burden and the patient’s medical and psychological condition in bivariate and multivariate analyses. This could be explained by the fact that at that time, the patients have finished chemotherapy and radiotherapy. The end of these treatments and the gradually physical recovery from surgery marked the beginning of the rehabilitation phase, which is also accompanied by a lower level of psychological distress in patients. This improvement in patient condition was probably at the origin of the decrease in subjective burden reported by the partner between T1 and T2.
Concerning the effect of couple satisfaction on subjective burden, results of multivariate analyses confirm our second hypothesis. Couple satisfaction, after the medical and psychological conditions of the patient were controlled for, explained 29% and 46% of the variance of subjective burden at 3 and 12 months post-surgery, respectively. This means that the negative impact of caregiving largely depends on the quality of the relationship between the caregiver and the care recipient, over and above the patient’s condition and regardless of the phase of treatment. This result was in line with the few studies focusing on the caregiver–patient relationship that showed that the quality of this relationship was crucial in determining subjective burden. When the quality of the relationship was good, caregivers experienced less subjective burden even though an objective burden was present (Snyder, 2000; Steadman et al., 2007). Starting with these results, we can conclude that subjective burden seems to have an important relational component. Characteristics of satisfied couples may explain this effect. First, the partners of highly satisfied couples normally reported an important sense of ‘we-ness’, namely a sense of unity (Gottman and Levenson, 1999; Reid et al., 2006). In the context of a serious illness, where the lives of both partners are likely to be affected, this translates into the perception of the illness as a shared stressor or a ‘we-disease’ (Kayser and Scott, 2008), which involves both partners and not only the patient. From this perspective, we can imagine that caregiving is not perceived by the healthy partner as an external imposition, but as the obvious consequence of the situation and the only thing to do to face the illness together. In addition, according to the equity theory (Walster et al., 1978), when a couple faces a serious illness such as breast cancer, there is a change in the balance of give-and-take between partners (Cutrona, 1996). The healthy partner must take on new caregiving roles and the exchange may become more unidirectional (Kuijer et al., 2004). In distressed couples, partners may feel inequitably treated and this feeling of inequity is generally associated with increased distress. In contrast, in satisfied couples, the imbalance is not experienced as inequitable, but only as a momentary transition (Buunk and VanYperen, 1991; Kuijer et al., 2001).
Contrary to what was assumed in the stress process model, no background and context characteristics of the partner predicted subjective burden. The effect of age, the only variable that was found to be significantly correlated with subjective burden at T1, lost its significance when couple satisfaction was entered into the regression model. In addition, no significant effect was found for individual coping and social support.
This study has several limitations. The modest sample size limits generalizability. The participation rate of romantic partners was not high but is nonetheless satisfactory, considering that participants must complete questionnaires during the acute illness phase, as well as the great difficulty in recruiting couples in psycho-oncology studies in which both the patient and the partner need to agree to participate (Fredman et al., 2009). A second limitation was that we did not have a specific measure of care demands (e.g. number of hours the partner spent on caregiving, number and kinds of tasks that the partner performed). Finally, several studies have shown that caregiving may also have a positive impact on the caregiver. Indeed, caregiving may be experienced as a challenge and may induce feelings of pride, a sense of self-worth and rewards. It may also be accompanied by increased love, affection and commitment between the caregiver and the care recipient (Carey et al., 1991; Lopez et al., 2005; Marks et al., 2002). It would thus be incorrect to consider caregiving only as a stressor linked to distress, fatigue and burden (Nijboer et al., 1998). This aspect would be interesting to integrate in further studies because it could have a protective effect on both the couple relationship and the partner’s psychological well-being.
Notwithstanding these limitations, this study has shown that couple satisfaction is the factor that most explained the subjective burden in romantic partners of non-metastatic breast cancer patients during the first year after surgery. A study of the subjective burden in the context of a loving relationship thus seems to need to take into account the quality of the relationship because it can determine the perception of caregiving. From a clinical perspective, interventions aimed at helping romantic partners to better adjust to the illness and to improve their psychological well-being need to take into account the quality of the relationship. Reducing the partner’s distress by directly acting on the objective burden, for example, by reducing caregiving tasks and providing practical support, would certainly help. In the case of an illness that enters remission such as non-metastatic breast cancer, however, the portion of subjective burden linked to the concrete (objective) caregiving burden probably would have declined naturally over time following the improvement of the medical condition of the patient, while leaving unaltered any portion of burden linked to an unsatisfactory couple relationship. It would thus be more interesting to evaluate the relationship between the caregiver and the patient to identify possible difficulties and, if any exist, to assist caregivers and care recipients in restoring, improving and cultivating their relationship. This could be done, for example, by improving communication and reciprocity and restoring the perception of equity in a give-and-take balance, while resolving and lessening couple conflicts. Acting on a dysfunctional and unsatisfactory relationship would probably have a more effective and durable effect on the subjective burden of the caregiver and consequently on his well-being.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study benefited from the support of the Swiss National Centre of Competence in Research LIVES – Overcoming vulnerability: life course perspectives, which is financed by the Swiss National Science Foundation.