
Abstract
This study examined gender differences in how internalizing and externalizing symptoms affect adolescents’ decisions about smoking in Chile, where girls smoke at some of the highest rates in the world. In multivariate logistic regression analyses with 607 adolescents, internalizing symptoms, such as depressed mood and anxiety, predicted smoking among girls more than boys, with girls who were low in internalizing symptoms being more likely to smoke than those who were high in internalizing symptoms. In Chile’s high-risk context, internalizing symptoms may be indirectly protective for girls by decreasing their exposure to peer pressure and related influences that encourage cigarette use.
Introduction
Although cigarette smoking rates are on the decline among US teens (Johnston et al., 2014), youth smoking remains a global problem (Eriksen et al., 2015). Nowhere more so than in Chile, where smoking among 13–15 year olds ranks among the highest in the world (Eriksen et al., 2015). Even compared to other Latin American countries, youth in Chile are at particularly high risk, with over half of Chilean youth reporting smoking at least once (CICAD, 2015). Earlier onset of smoking is associated with increased risk of later cigarette use (Everett et al., 1999), elevated nicotine dependence levels (Kendler et al., 2014), and numerous serious health and mental health consequences (US Department of Health and Human Services (DHHS), 2014).
In addition, smoking patterns in Chile are somewhat unusual in that a greater percentage of Chilean girls (42%) than boys (34%) report smoking in the past year (CICAD, 2015). These gender differences are particularly interesting because a behavior that was once more common among men is no longer, perhaps as a result of tobacco companies’ aggressive targeting of women and girls (American Lung Association, 2009) and populations in low- to middle-income countries (Borzekowski and Cohen, 2013). In response to calls for research examining gender differences in the factors underlying smoking decisions (Amos et al., 2011), this study takes advantage of this unique context to explore gender differences in the relationship between smoking decisions and internalizing and externalizing problems, the base rates of which vary systematically by gender (Leadbeater et al., 1999). Internalizing and externalizing problem clusters reflect a broad and frequently used categorization of adolescents’ emotional and behavioral disturbances as either overcontrolled or undercontrolled problems (Achenbach and Edelbrock, 1978). More specifically, internalizing problems are depression, anxiety, and withdrawal; externalizing problems are uncontrolled, undesirable behaviors such as delinquency and aggression (Achenbach, 1991). Although a substantial body of research has linked substance use to childhood internalizing and externalizing symptoms (e.g. Brook et al., 2006; King et al., 2004; Patton et al., 1998), questions remain as to whether the nature of these relationships varies by gender (Miettunen et al., 2014). In addition, the high rates of Chilean girls’ smoking raise the possibility that, in this context, gender may impact the relationship between these psychological symptoms and smoking in unexpected, important ways.
Internalizing and externalizing symptoms and substance use
While numerous studies link internalizing symptoms to substance use, there is little consensus about the nature of that relationship. One possibility is that internalizing symptoms are related to higher rates of smoking among adolescents. Research supporting this link finds positive relationships between smoking and depression or depressive symptoms (e.g. Brook et al., 1998; Goodman and Capitman, 2000) and anxiety disorders (e.g. Jamal et al., 2011). A potential mechanism for this relationship is self-medication, the use of cigarettes to cope with negative mood (Khantzian, 1997). For instance, longitudinal work finds that depression in adolescence predicts smoking initiation (Brook et al., 2006). Similarly, depressive and anxious symptoms predict smoking experimentation, but only among youth reporting having peers who smoke (Patton et al., 1998), suggesting that self-medication may be learned from peers. At the same time, there is also evidence for the alternate pathway—smoking increasing internalizing symptoms (Miettunen et al., 2014; Wu and Anthony, 1999).
Although many studies find a positive relationship between internalizing symptoms and substance use, some studies find the opposite. In a study of high school seniors, students reporting more internalizing symptoms were less likely to initiate drinking by the end of the year (Stice et al., 1998). Another study found that social anxiety was related to drinking smaller quantities and less frequently among middle school students (Tomlinson and Brown, 2012). Most of these studies focused on alcohol, but anxiety has also been linked to delayed onset of smoking (Costello et al., 1999). A potential explanation is that internalizing symptoms are protective because withdrawn youth avoid peer influences that encourage substance use, suggesting that internalizing’s protective effect is limited to use initiation and will not extend to later use decisions (Hussong et al., 2011).
In contrast to internalizing problems, the positive relationship between externalizing problems and substance use is more robust and consistent (e.g. Brook et al., 2006; King et al., 2004). Propensity toward behavioral disinhibition may underlie these associations (Iacono et al., 2008), thus the risky behaviors captured by externalizing measures may be motivated by the same factors that increase risk of smoking.
Gender, internalizing and externalizing symptoms, and smoking
Base rates of internalizing and externalizing problems often reveal that female adolescents experience more internalizing problems while male adolescents have more externalizing problems (Costello et al., 2003; Zahn-Waxler et al., 2008). However, gender differences in symptoms may not translate to gender differences in how symptoms affect substance use. In the case of externalizing symptoms, studies have not found evidence that gender moderates the positive relationship between externalizing and smoking (Dierker et al., 2007; King et al., 2004; Schwinn et al., 2010).
The evidence for internalizing is more mixed. Some studies find no gender differences in the link between smoking and internalizing symptoms among adolescents (e.g. Brook et al., 1998; Schwinn et al., 2010). However, substantial evidence indicates, in contrast, that internalizing problems influence smoking more strongly among girls or, in some cases, only among girls (Crone and Reijneveld, 2007; Fleming et al., 2008; Poulin et al., 2005). Similar patterns have been uncovered relating depression and anxiety disorders to smoking in girls but not boys (Dierker et al., 2007). The nature of these relationships can also vary, as in work that finds social phobia and smoking to be positively related among boys, yet negatively related among girls (Wu et al., 2009).
Aims of this study
In this study, we use childhood internalizing and externalizing symptoms at age 10, reported by the children’s parents, to predict smoking in adolescence. In addition, we consider effects on decisions to smoke when first offered a cigarette and current smoking given evidence that many factors of interest differentially influence these two outcomes (e.g. Tucker et al., 2003; West et al., 1999). The majority of research reviewed above was conducted in US and European contexts; Chile offers a useful counterpoint to these results, particularly for studying gender. Furthermore, this study moves beyond gender differences to consider how gender may affect the relationship between these symptoms and smoking (e.g. Schwinn et al., 2010). Examining how internalizing and externalizing symptoms may predict smoking in Chile, and whether these pathways differ by gender, will expand knowledge of these pathways into new contexts while also offering insight for much needed smoking prevention approaches in Chile.
Methods
Santiago Longitudinal Study design and study sample
Data for this study are from the Santiago Longitudinal Study (SLS), a collaborative project between US and Chilean institutions. Participants for this study are urban adolescents from working-class communities in the southern part of Santiago who at infancy (N = 1657) participated in a study of iron supplementation in 1991–1996 (Lozoff et al., 2003). Approximately 1100 of these individuals were successfully followed and re-interviewed at age 10 (Lozoff et al., 2012). Of the families who were re-contacted, 1076 participated again in 2007–2010 when youth were 12–17 years old. For this study, data from two timepoints were used (ages 10 and 12–17).
SLS interviews were conducted in Spanish in private rooms at the Chilean institution by clinical psychologists trained to administer the questionnaires. Some instruments already existed in Spanish and had been used in studies with Chilean populations (e.g. demographic questions and cigarette use questions). Other instruments were translated by the US research team and then modified for comprehension, language, and conceptual equivalence based on pilot testing and feedback from the Chilean research team. This study was approved by the University of Michigan’s Institutional Review Board, and parental consent and child assent were collected from all participants.
In the sample of 1076 adolescents, 1041 responded to questions about their first opportunity to smoke. Of the 1041 respondents, 83.3 percent (n = 867) had been offered a cigarette at some point in their lives. Given that baseline data were collected at age 10, we examined only those who had been offered their first cigarette after age 10. As a result, of those adolescents who had ever been offered a cigarette, we limited our sample to the 79.9 percent (n = 693) who reported being offered a cigarette at age 11 or later. After listwise deletion to retain the 87.6 percent of participants with full data across all predictor and outcome measures in our model, our final analytic sample of 607 (51.4% male) is an average of 14.8 (standard deviation (SD) = 1.41) years old (age range, 12–17). Their first cigarette offer occurred on average at age 12.6 (SD = 1.15). Comparisons between the analytic and the total sample indicate that our analytic sample is slightly older (14.8 vs 14.2, t(1074) = 6.63, p < .001) and more likely to be current smokers (27.2% vs 16.2%, χ2(1, N = 1076) = 18.35, p < .001), but there were no significant differences on the predictor variables (internalizing or externalizing symptoms) or other demographics (gender or socioeconomic status).
Measures
Timepoint 1: age 10
Internalizing and externalizing symptoms
At time 1, when children were 10 years old, parents completed the Spanish version of the child behavior checklist (Achenbach, 1991), in which they rated a series of behaviors as 0 = not true, 1 = somewhat or sometimes true, or 2 = very true or often true for their child. A composite internalizing symptoms score (α = .85) was created by summing responses to items about their child’s withdrawn behaviors, somatic complaints, and anxious or depressive symptoms (e.g. “Feels worthless or inferior” and “Would rather be alone than with others”). A composite externalizing symptoms score (α = .89) was derived from responses to items assessing delinquent problem behaviors and aggression (e.g. “Steals at home” and “Vandalism”).
Timepoint 2: adolescence
First use decision
At time 2, when the children were 12–17 years old, they were asked, “Have you ever had an opportunity to try cigarettes?” and responded either yes or no. Those responding yes were asked, “At what age did you have the first opportunity?” and answered within the truncated range of 6 (any age younger than 7) to 17. We used these variables to limit our sample (described above) in order to examine responses to first cigarette offers, measured by response to: “When you had this opportunity, did you smoke cigarettes at that time?” (0 = No, 1 = Yes).
Current smoker status
We operationalized current smokers as youth who reported smoking in the past 30 days. Adolescents answered the question: “Have you ever smoked all or part of a cigarette?” (0 = No, 1 = Yes). Adolescents who answered yes were asked, “When was the last time you smoked cigarettes?” (1 = in the past 30 days, 2 = more than a month ago but within the past year, 3 = more than a year ago). Reponses were recoded into a binary measure in which those having smoked in the past 30 days were coded as 1, and those smoking more than a month ago or never having smoked were coded as 0.
Demographic variables
Adolescents self-reported their gender and age. Parents reported on mother’s and father’s completed years of education, family income, and mother and father’s combined educational prestige, which were combined into a composite socioeconomic status score (SES; α = .81).
Analytic plan
Before conducting the main set of analyses, we mean-centered the continuous predictor variables to aid interpretation of interaction effects. The dichotomous dependent variables, response to first cigarette offer and current smoker status, were both examined by logistic regression. In logistic regression, we tested for the interactions of interest between gender and internalizing symptoms, and gender and externalizing symptoms. There was no significant interaction between externalizing symptoms and gender (this was true in all three regression models), so it has been removed from the model for parsimony. Including the externalizing symptoms by gender interaction in the model presents a similar pattern of effects in all three models.
Results
Preliminary analysis
We first tested for gender differences across our dependent and independent variables. Boys (n = 312) and girls (n = 295) did not differ in age, SES, internalizing symptoms, or age at first cigarette offer. Boys (M = 16.43) had higher mean levels of externalizing symptoms than girls (M = 14.69, t(605) = 2.55, p < .05). Consistent with data from recent national surveys in Chile (CICAD, 2015), a slightly higher percentage of girls than boys (29.2% vs 25.3%) reported smoking in the past month, although this difference was not statistically significant (p = .29). Girls were more likely to smoke the first cigarette they were offered than boys (50.2% vs 42.6%), an effect that approached significance (χ2(1, 605) = 3.47, p = .06).
Predicting decision to smoke when first offered a cigarette
We next considered the influence of childhood mental health on the decision of whether or not to smoke when a child received his or her first cigarette offer. The regression model included the childhood mental health variables (internalizing and externalizing symptoms), the interaction of interest between gender and internalizing symptoms, and controls for demographic characteristics. As shown in Table 1, female adolescents had higher odds than males of accepting their first cigarette offer (odds ratio (OR) = 1.43, p < .05). Among the other demographic variables, older youth (OR = 1.34, p < .001) and lower SES youth (OR = 0.81, p < .05) had higher odds of smoking at first offer. Youth with more externalizing symptoms were more likely to accept their first cigarette offer (OR = 1.04, p < .01), which did not differ by gender. There was, however, a significant interaction between gender and internalizing symptoms (OR = 0.95, p < .01).
Odds of youth smoking at first cigarette offer and current smoker status (past 30 days): results of logistic regression.
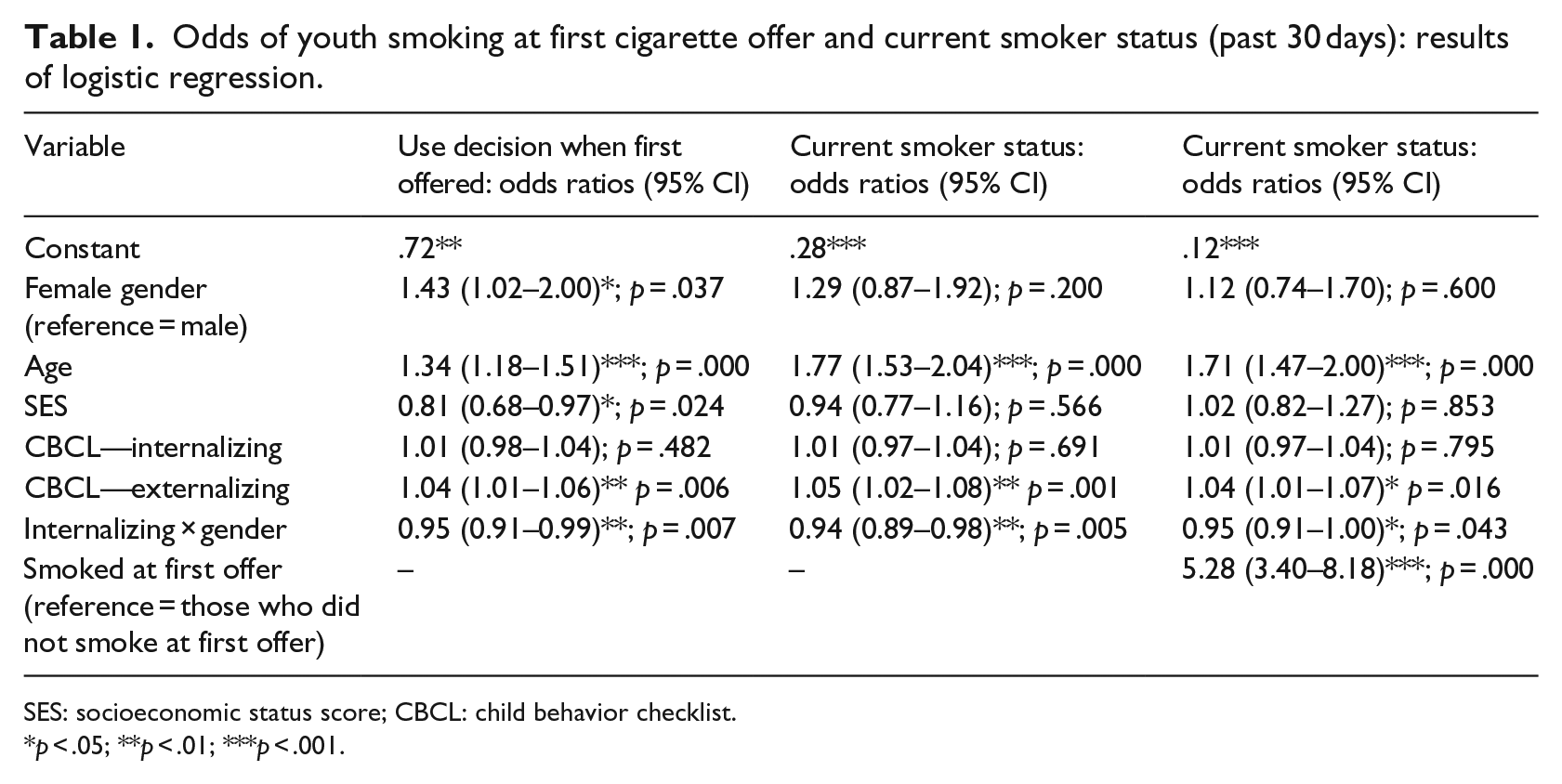
SES: socioeconomic status score; CBCL: child behavior checklist.
p < .05; **p < .01; ***p < .001.
In order to understand this interaction, we followed Jaccard’s (2001) recommendation to use a series of logistic regressions centered at 1SD above and below the mean level of internalizing symptoms (and controlling for SES, age, and externalizing symptoms). This approach allowed us to calculate the probabilities that boys and girls at each level of internalizing symptoms would accept their first cigarette offer, illustrated in Figure 1. There was no significant difference in the predicted probability of accepting a first cigarette offer between boys and girls (.44 vs .42) who were high in internalizing symptoms (+1SD). In contrast, among those low in internalizing symptoms (−1SD), girls had a significantly higher probability of smoking at first offer than boys (.60 vs .40), as indicated by the significant ratio of predicted odds for boys to girls (OR = 0.44, p < .01). Analysis of simple slopes indicated that internalizing symptoms had a significant effect among girls (OR = 0.96, p < .01) but not boys (OR = 1.01, p > .4). This suggests that the significant interaction was driven by girls who were low in internalizing symptoms being more likely to smoke than those who were high in internalizing symptoms.
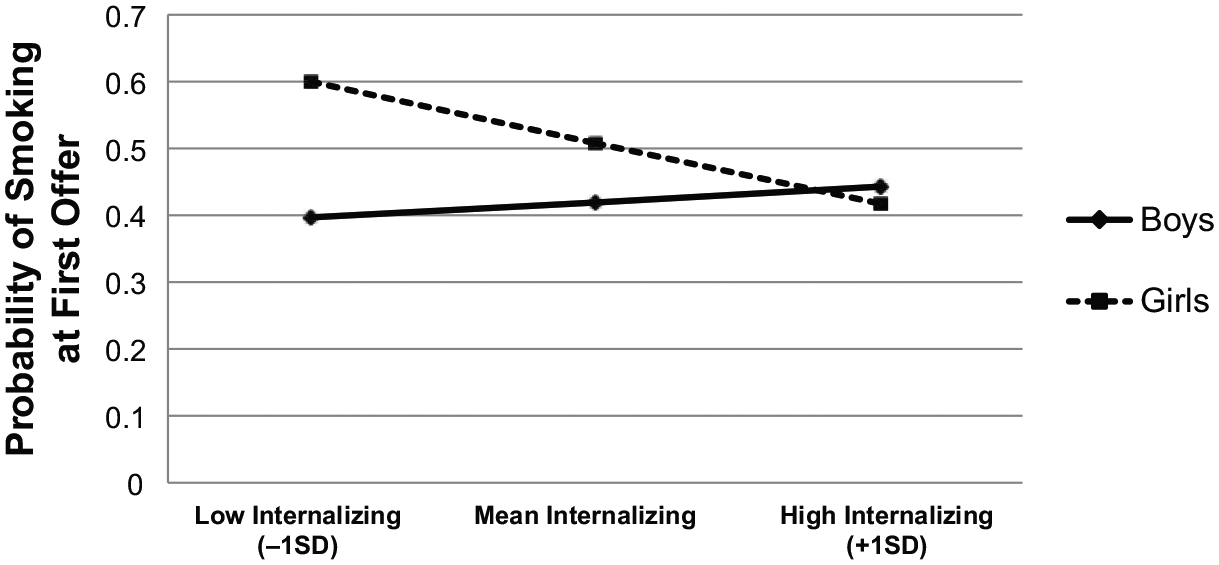
Interaction of internalizing symptoms and gender predicting probability of smoking at first offer. Graph depicts predicted probabilities of smoking when offered a cigarette for the first time. Gender moderates the relationship between internalizing symptoms and smoking at first offer. Low internalizing refers to responses at 1SD below the mean and high internalizing refers to responses at 1SD above the mean.
Predicting current smoker status
Next, we used the same model to predict the likelihood that adolescents in our sample were current smokers, measured as smoking within the past 30 days, reported in Table 1. Among our demographic covariates, only age was significant; older adolescents were more likely to be past-month smokers (OR = 1.77, p < .001). Externalizing symptoms increased youths’ odds of being past-month smokers (OR = 1.05, p < .01), an effect that was not moderated by gender. As in the model predicting first offer decisions, there was a significant gender by internalizing symptoms interaction predicting current smoker status (OR = 0.94, p < .01).
Following the same procedure as before, we assessed this interaction further across the three levels of internalizing, ranging from 1SD below to 1SD above the mean level of internalizing symptoms (this figure can be found in the supplemental materials). There was no difference in the probability of boys versus girls (.23 vs .18) being a past-month smoker among those high in internalizing symptoms, but for those low in internalizing, girls had a significantly higher probability of being past-month smokers than boys (.38 vs .21) (OR = 0.44, p < .01). Again, these effects were driven by a significant simple slope for girls; girls were more likely to be past-month smokers if low rather than high in internalizing symptoms (OR = 0.94, p < .01). Among boys, the odds of being a past-month smoker did not vary by internalizing symptoms (OR = 1.01, p > .6).
Finally, we tested a logistic regression model predicting current smoker status that included youths’ decisions to smoke when first offered a cigarette (Table 1). This model emphasized the importance of adolescents’ smoking decisions when first offered a cigarette. In this final model, first use decisions (OR = 5.28, p < .001) were quite consequential, with youth who accepted their first cigarette offer being much more likely to be past-month smokers. Even with the inclusion of this covariate, the model again revealed a significant gender by internalizing interaction (OR = 0.95, p < .05) that was driven by females having a higher predicted probability of being smokers when they reported low rather than high internalizing symptoms (.20 vs .08), OR = 0.96, p < .05.
Discussion
This study of a large sample of Chilean youth examined gender differences in the relationship between internalizing and externalizing symptoms and the decision to smoke when first offered a cigarette and the odds of being a current smoker. The results offer support for previously established patterns of use and influence, while contributing new evidence for the presence of gender differences in the relationship between internalizing symptoms and decision making about smoking.
Cigarette use patterns in our sample reflected findings from population studies in Chile showing slightly higher smoking rates among girls (CICAD, 2015), with girls in our sample being more likely than boys to accept their first cigarette offer. Also replicating previously established associations, externalizing symptoms at age 10 were related to increased odds for smoking at first offer and smoking in the past month among boys and girls in early adolescence. In contrast, the relationship between internalizing symptoms and later smoking decisions differed between boys and girls. The smoking decisions of boys and girls who were high in internalizing symptoms look quite similar, but as the amount of internalizing experienced by girls decreased, their odds of accepting their first cigarette offer and being a past-month smoker increased. Experiencing a higher number of internalizing symptoms may be protective for girls, but not boys.
Externalizing and internalizing problems and smoking decisions
Within our sample, female adolescents with relatively low levels of internalizing were at highest risk of being smokers. Many studies in North American and European contexts have found that internalizing symptoms increased the risk of being a smoker (Goodman and Capitman, 2000; Jamal et al., 2011), but there are examples of higher levels of internalizing symptoms being associated with lower risk of substance use (Costello et al., 1999; Stice et al., 1998).
One explanation points to social learning as a mechanism that increases substance use among youth engaging normally with peers (Tomlinson and Brown, 2012). Support for this interpretation comes primarily from research in the United States on alcohol use, which is often discussed as a normative teen activity (Fergusson and Horwood, 1999). It is possible that girls suffering from more anxious and depressed symptoms are less likely to engage in social interactions with peers, both normative and non-normative, during which smoking may occur. In addition, the cultural meaning of smoking may differ between girls and boys in Chile. For example, smoking may communicate messages of female empowerment that could appeal to young women (Hitchman and Fong, 2011), although perhaps not to those who are socially withdrawn.
The externalizing results reproduced patterns frequently observed in North American and European samples (e.g. Costello et al., 1999; Iacono et al., 2008)—externalizing symptoms were related to greater likelihood of accepting a first cigarette offer and being a current smoker. There were no gender differences in the relationship between externalizing and substance use, although the effects of this relationship may be more consequential for boys given their higher externalizing symptom levels.
The similarity of the results for adolescents’ first cigarette offer decision and past-month smoker status is noteworthy. Some work suggests that internalizing symptoms can have a protective effect for smoking initiation at younger ages but that this protection may not extend to later use (Hussong et al., 2011). However, we found this association for girls’ first use decisions and later smoking status. One contributing explanation may be that escalation to regular smoking is predicted by peer use in particular (West et al., 1999). In this way, the presence of these associations for both smoking outcomes is supported by the hypothesis that girls who are anxious and depressed are less impacted by peer use.
Limitations and future directions
There are several limitations to this study. One important limitation is that our results do not come from a nationally representative sample. One must exercise caution in generalizing these results; however, it is encouraging that the smoking rates in our sample look similar to recent national surveys (CICAD, 2015). In addition, youth were asked to recall their response to their first cigarette offers, and this recall may be biased to align with more recent smoking decisions. Another limitation is that this study focused only on youth who have been offered a cigarette at some point. In light of the possibility that girls with more internalizing symptoms may circumvent smoking risks by avoiding social situations more generally, youth who have avoided being offered a cigarette may share characteristics with these girls. Finally, we used symptoms measured at age 10 to predict later smoking decisions, but investigating these potentially bidirectional effects as they unfold over time is left to future work. The challenge will be to understand how these psychological variables affect smoking experimentation, escalation, and frequency across developmental periods and cultural contexts.
Implications for smoking prevention in Chile
Boys may have previously been at greater risk than girls, but these patterns appear to be shifting among younger cohorts and particularly in nations with higher smoking prevalence (Eriksen et al., 2015). Examining the factors that influence smoking using gender as a moderator offers insight for intervention approaches that may work for boys, girls, or both. Our results point to externalizing problems, such as aggression and self-control, as potential targets of intervention for both boys and girls. Efforts to encourage the development of impulse control skills may have beneficial downstream effects on smoking initiation. Alternatively, assessments of these symptoms may offer criteria to target prevention efforts on youth who are at greater risk.
Based on our findings, social norms may also be a useful prevention focus in Chile. In a context where smoking is slightly more prevalent among girls, our results suggest that normative mental health is linked to smoking for girls. Among our sample, the girls choosing to smoke were not depressed, anxious, and withdrawn. Rather than smoking to relieve anxiety or treat negative mood, it seems more likely that these girls were motivated to smoke by the desire to affiliate with peers. Preventive interventions that frame smoking as non-normative and highlight healthier ways to connect with peers may be critical for reversing the rising smoking trends among young women in Chile.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the U.S. National Institute on Drug Abuse (Grant R01-DA-022720).