
Abstract
The complex linguistic profile of South Africa has the potential to limit the efficiency of emergency calls. Emergency services depend on rapid resolution of a call, dispatch of an ambulance and response at scene. Resolving language mismatches is a critical feature of everyday practice in such a setting. This study examined accommodation to language shifts in a call centre using conversation analysis methods. Three main call trajectories were identified and the analysis suggested marked differences in responsivity, reflecting attitudinal and societal stratification. Conversation analysis provided insight into communication barriers and contextual features, which have implications for training.
Introduction
Getting help quickly is of paramount importance in an emergency situation. A call to an emergency number must result in the rapid dispatch of emergency services to the scene. In order to achieve this goal, the caller and call taker must engage in a process of efficient information exchange. This process may involve negotiating language choices and/or using interactive strategies to manage language mismatches between the caller and call taker. This study examines how language mismatches are managed in calls to an emergency call centre in South Africa.
The South African health care system faces a number of inherent challenges linked to factors such as historical inequities, resource constraints, the vast distinction between private and public care, and on-going systemic inefficiencies (Coovadia et al., 2009; Mayosi et al., 2012). In many areas, high rates of unemployment, crime and poverty have contributed to an increase in communicable and non-communicable diseases. Trauma incident rates are much higher than in more developed countries (Hardcastle et al., 2013; Sun et al., 2014; Wallis et al., 2008). South Africa experiences a large number of traffic-related incidents, including motor and pedestrian vehicle accidents (Parkinson et al., 2013).
Emergency medical services are coordinated on a provincial basis in the public sector. In the Western Cape, the site of this study, emergency calls are handled by a central call centre in the province’s capital that organises the dispatch of ambulatory emergency care throughout the province for a population of almost 6 million people. This province covers a large surface area that includes both dense urban and sparse rural regions (Statistics South Africa, 2012). There are pockets of great wealth and also areas of profound poverty characterised by high levels of unemployment, disease, gangsterism and violence, alcohol abuse, and xenophobia (Boulle, 2014; Charman and Piper, 2012; Gossage et al., 2014; Matzopoulos and Myers, 2014).
The South African linguistic profile is complex and diverse. Aside from the 11 official languages, a number of other African languages are encountered in everyday health practice. The South African Constitution specifies that patients have a right to treatment in the language of their choice (LANGTAG, 1996). A Pan South African Language Board was established to advance the use of indigenous or local languages of South Africa (LANGTAG, 1996) and a policy on language services for the National Department of Health (2015) reinforces the recommendation for multilingual language services. Most health care professionals are not fluent in local African languages. English and Afrikaans remain the two most prominent languages spoken in the health care sector although the majority of the population is not fully proficient in these languages. Even when health care professionals and patients are culturally and linguistically matched, interactions may take place in a language that is not the patient’s home language. Therefore, for the most part (at least in the public sector), there is a lack of concordance between the languages and cultures of health professionals and their clients. The lack of available interpreters (Lesch and Saulse, 2014), as well as the presence of asymmetries and hierarchies in health care contexts (Gillespie et al., 2014; Meeuwesen et al., 2007; Reader et al., 2014), may confound language negotiation as callers to an emergency health care service may not feel able to make a request to speak the language of their choice.
The Western Cape has a unique language profile. Around 50 per cent of the population are first language Afrikaans speakers (the highest percentage in the country), followed by approximately 25 per cent isiXhosa speakers, 20 per cent English speakers and the remaining 5 per cent are speakers of other languages (Statistics South Africa, 2012). Given the high number of immigrants and refugees residing in the Cape Metropole, there is a strong likelihood that language barriers will be present when callers telephone the call centre in an emergency situation. Deumert (2010) comments on language barriers present in the health care system in this context and the fact that ‘linguistic barriers between English/Afrikaans-speaking providers and isiXhosa-speaking patients are a deeply entrenched structural feature of the public health system, and significantly impede the provision of equitable and effective health care’ (p. 53).
The management of language interactions in a multilingual context reflects social rules and attitudes, and switching between languages may be considered a highly significant social act (Wei, 2005). Factors such as power and hierarchy determine these switches, particularly in institutional contexts. Central to this is the notion of accommodation (Giles et al., 1973) or responsiveness in a conversation (Schegloff, 1986).
The manner in which language mismatches or barriers are handled by conversational partners has been the subject of a number of studies of telephone calls in various contexts. Language choices in interactions may be negotiated or worked out interactively between the two parties (Gafaranga and i Calvo, 2001; Zhang, 2005). Language choices and shifts in calls are social actions related directly to the sequential context of the interaction and there is a routinisation of language choice (Rasmussen and Wagner, 2002; Wei, 2005). In telephone calls, the caller may follow the language used by the call taker or may attempt to change the language. Social structure often determines language choice and results in sequential implications for such language choice (Rasmussen and Wagner, 2002).
Some communities are more stable when it comes to multilingualism, which means that both parties are easily able to agree on the language of choice in a particular situation, the language choice is made with little need for negotiation and the language shifts happen seamlessly (Haberland, 2007). Ideally, both speakers should be committed to achieving coherence in the interaction through mutually agreeable language choices (Wei, 2005).
This study describes a context in which less stability appears to be present. In a complex multilingual society, the negotiation of language usage in a call centre has important implications for organisational efficiency and training. We were interested in emerging practices and how call takers accommodate the diversity of the languages used by callers. The study of language shifting provides an opportunity to look at how people adapt to linguistic diversity as well as the degree of accountability in institutional talk (Haugh, 2013). The efficiency of such accommodation assumes particular relevance within the context of an emergency call centre.
Our research questions were thus as follows: How are language mismatches handled in emergency calls? What influences code switching behaviour in a multilingual context?
Methods
The study was conducted at a call centre in the Western Cape. Ethical clearance for the study was obtained from the University’s Medical Ethics Committee and permission was received from the call centre.
Our methods incorporated regular visits, ethnographic studies and interviews with team members. Call takers at the centre are matched with the provincial demographic profile and most are bilingual in English and Afrikaans. English is the official language of the centre but call takers are trained to deal with callers who have multilingual communicative needs. There is always an isiXhosa-speaking person on the call centre floor, and call takers are urged to transfer isiXhosa callers when language difficulties are recognised.
The data set for this study included approximately 180 audio-recordings of calls made to the call centre between 2010 and 2013, in the following categories: trauma, maternity, patient unresponsive, call backs and teenage pregnancies. In 2012–2013, the centre facilitated the transport of almost 500,000 patients. The centre aims to ensure optimal response times to medical emergencies and incident scenes and it has set a number of targets in this regard.
We used a qualitative analytic framework based on conversation analysis (CA) principles, as has been used in the analysis of calls to emergency services in other countries (e.g. Cromdal et al., 2012; Whalen and Zimmerman, 1998). CA identifies and describes the sequential elements of conversation and interaction and highlights how particular activities are achieved by examining the detail of talk (Sidnell and Stivers, 2013). This method also focuses on evidence of communication success or failure in the conversational context and responses of each interactional participant. A CA analysis enables us to see how things such as ‘identity, attitude and relationship are presented, understood, accepted, rejected, or changed in the process of interaction’ (Wei, 2005: 382).
We identified a subset of 21 calls in which a language mismatch or switch was evident. An examination of the opening sequences of these calls revealed a number of possible trajectories of calls in which language mismatches occur and we categorised them into the patterns described below. All authors engaged in this process simultaneously to ensure reliability and group consensus. Later, we revisited the calls and looked at whether language mismatches or switches were present throughout the call or only in the initial sequence.
We present five extracts in this article, transcribed by a research assistant (using Jefferson’s (2004) transcription notations) and checked by the authors. The isiXhosa sections of talk were translated and checked by a first language speaker.
Results
Although the official language of the call centre is English, most of the call takers (CTs) and the callers (Cs) in the sample we studied were not first language English speakers.
Of the 21 calls analysed in detail, we found three main trajectories as illustrated in Figure 1.
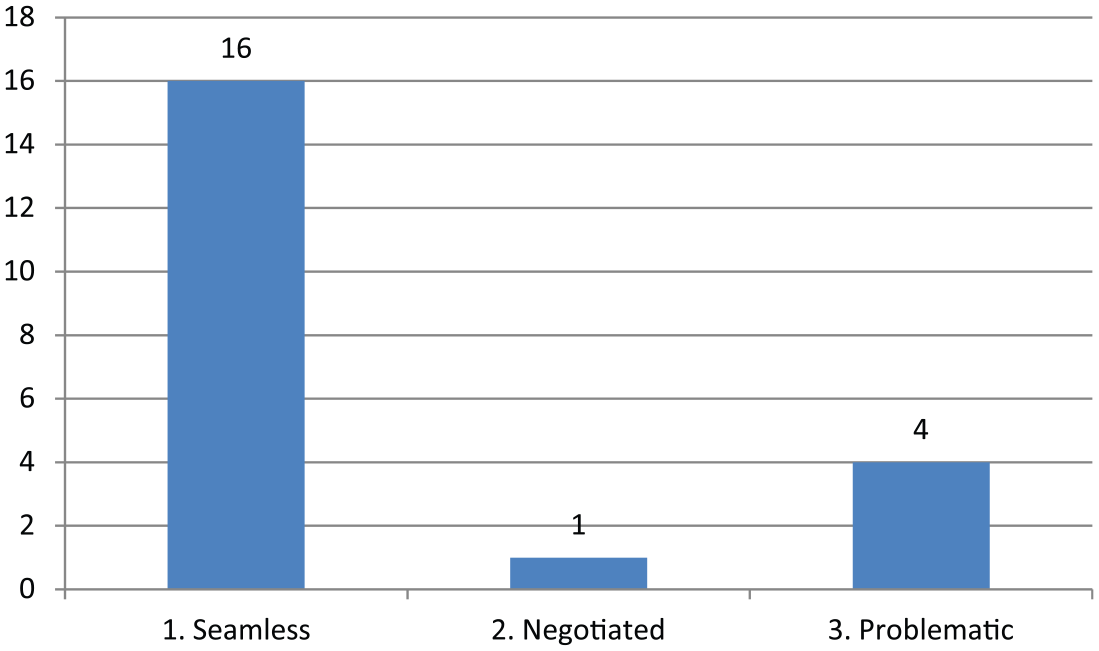
Caller and call taker language mismatch trajectories.
The first and most common is a trajectory in which the language mismatch is handled smoothly and the whole call reflects accommodation. This occurred in 16 of the 21 calls analysed. Typically, the CT answers the call in English, the C responds in another language (usually Afrikaans), and the CT then switches to the C’s preferred language and continues the call. In some of these cases, CTs demonstrate the ability to recognise a C’s language preference based on only a minimal voice sample that may not include any recognisably non-English words. In three of the calls, the C responded in another language but when the CT continued in English, the C accommodated this with English responses without any need for further negotiation. Calls with this type of trajectory are able to progress smoothly and the language mismatch does not cause any disruption.
In the second trajectory, the CT answers the call in English and the C requests permission in their first turn to speak a preferred language. Thus, the issue of language choice becomes the topic of the turn. This only occurred in one of the calls and it appears that typically the C expects the CT to accommodate for language.
A third trajectory is one in which the language issues clearly delay and complicate call progression, and interactional accommodation and accountability seem to be compromised. For example, Cs may speak their preferred language in their first turn and CTs respond by instructing the Cs to speak English. This occurred in four of the calls analysed. Three of these four cases involved languages other than English and Afrikaans.
In the following extracts, which are anonymised, examples of each type of trajectory are presented.
Extract 1 is taken from an interaction that showed a good language match and no communication difficulties throughout. The CT opens the call in English. The C however responds in Afrikaans, thus indicating that this is the language of preference for this call. Although there are two possibilities here – (1) the C recognises the CT’s accent as someone who would be able to converse in Afrikaans, or (2) the C can only speak Afrikaans so begins to speak it in the hope that the CT can also converse in Afrikaans – the former seems more plausible given the communicative attunement of the participants during this call. The CT accommodates to the C’s language preference and the call continues without difficulty in Afrikaans.
Thus, the pattern can be schematised as follows:
CT answers in English → C responds in Afrikaans → CT switches to Afrikaans Extract 1: Teenage pregnancy
In some cases, the trajectory differed. In Extract 2, the CT opens the call in English. Based on the C’s one-word response of ‘hello’, the CT immediately switches into Afrikaans and the call continues seamlessly in this language. In this example, the CT shows accountability and recognises the C’s cues regarding what is needed for this interaction to proceed smoothly. As described by Zhang (2005), in this instance, the language used by the C in their first turn determines the language used for the entire call. Merely by hearing the word ‘hello’ and interpreting the pauses and hesitant ‘… hh’, the CT interprets that they need to perform an action (i.e. change to Afrikaans) and they initiate this swap. There is uptake of the C’s request without a direct request by the C to switch into Afrikaans. The interaction proceeds smoothly which confirms that the CT’s interpretation and subsequent action was appropriate.
The pattern is as follows:
CT answers in English → C responds (minimally) → CT switches to Afrikaans Extract 2: Sexual assault
In one instance, we noted that the language choice became the topic of the turn, as exemplified in Extract 3. The C specifically asks if she may speak Afrikaans. The CT authorises the C’s request to use her preferred language. Gafaranga and i Calvo (2001) argue that such an example indicates that the C is concerned about order and there is a need to negotiate a norm regarding language choices in the interaction. Again, this call proceeds smoothly with no communication difficulties noted.
The pattern is thus as follows:
CT answers in English → C asks to speak preferred language → call interrupted to negotiate language or deal with mismatch → call continues in C’s preferred language Extract 3: Trauma
The trajectories described above all resulted in successful language switches or negotiations. Significantly, however, we noted a few potentially problematic or actually problematic scenarios in our data set, as evidenced in the following two examples.
In Extract 4, we see a completely different pattern and the presence of significant communicative difficulties. There is an early request by the C for an ambulance and a language switch in line 6, which is repeated in line 9. The CT responds by admonishing the C and telling them to speak English (line 7). There is evidence of impatience in the repetition of ‘no’ (line 7) and ‘hamba’ (line 9).
The pattern is as follows:
CT answers in English → C speaks preferred language → CT instructs C to speak English → call interrupted to deal with language mismatch Extract 4: Call back
Extract 5 is of interest in several ways and a longer passage has been selected to reflect the complexities in the interaction. It involves a language mismatch and also an interaction between a CT and a C who is not South African. As the call unfolds, it is eventually transferred by the CT to an isiXhosa-speaking CT. The call proceeds in isiXhosa, but remains problematic in several aspects. In addition to the lengthy delay in the transfer to an isiXhosa-speaking CT (which only happens in line 70 after several conversational turns in which a location is unsuccessfully negotiated), once that issue is resolved there is a sense that this C is being treated in a different way to local Cs. The difficulties extend beyond the language mismatch (because clearly the C is struggling with the local language) and again seem to reflect impatience (e.g. lines 92 and 97) and a lack of accommodation. The tone of the interaction appears terse, rude and irritated – there are repetitions (e.g. line 128), sharp instructions (e.g. line 92) and some discussion about ethnic origin (lines 137–140). The C appears overwhelmed and the interaction is characterised by delays and asides.
The pattern is thus as follows:
CT answers in English → C attempts to speak English → CT eventually switches to isiXhosa → call proceeds in isiXhosa but takes a long time to resolve Extract 5: Teenage pregnancy
Discussion
The analysis of the management of language mismatches in our data set is interesting from a number of perspectives.
The first major observation was the surprisingly low occurrence of real difficulties with language mismatches at the site. Based on our research at other health sites in South Africa (e.g. Penn, 2007), we had expected that at this site there would be parallel difficulties particularly in the context of an emergency and because there is a prescribed one-language policy at the call centre. However, in the majority of calls, we analysed (76 per cent) (and indeed observed during our ethnographic study at the site) language mismatches were managed seamlessly and efficiently and a variety of repair and preventative techniques displayed. As in other studies on international telephone conversations (e.g. Rasmussen and Wagner, 2002; Zhang, 2005), in most of the calls, the language used by the caller becomes the language of the call. This finding suggests that there may be features of the context that enhance such fluidity. The call centre is markedly bilingual and there appears to be a cultural and linguistic match between many of the callers and the call takers in question.
On the other hand, there are examples where despite an enabling infrastructure, cross language calls were problematic. When the caller is Afrikaans speaking, there are no difficulties with communication but when there is a speaker of an African language, problems sometimes occur. Contextual factors appear to be profoundly important here in that the ethnicity of callers seems to make a difference. There are distinctions or judgements being made and the call takers do not consistently show accountability and accommodate language preferences.
There is a need to question why some calls are courteous and helpful and why others are not, why accommodation occurs efficiently with some callers and not with others. In short, the challenge is to explain why some callers face greater obstacles even in the face of policies advocating equitable language services.
The role of ethnicity is of course not surprising nor uniquely South African. For example, in the United Kingdom, helplines now include queries about ethnicity (described as ‘ethnic monitoring’ by Wilkinson, 2011). However, as Wilkinson (2011) has found, explicit questioning about ethnicity has proven awkward for volunteer call takers in a UK setting. In South Africa, with its complex past, ethnicity questions may often be viewed as similarly awkward or even offensive. This probably accounts for the fact that in this study there are no explicit language questions although our evidence suggests that this monitoring is implicit and happens more indirectly through language dialectal features and conversational cues like hesitations, and possibly also with other markers as well (such as the location of the caller and nature of the incident).
The evidence seems to suggest that historical divisions and suspicions which existed between racial and language groups linger and there remain linguistic and dialectal divisions which are markers of social class. Furthermore, there is documented presence of xenophobia in this context (Charman and Piper, 2012; Crush and Tawodzera, 2014), which is suggested in Extract 5. The evidence points to differences in call taker behaviour and management of the calls which seems to reflect the on-going stratification of society, attitudinal issues and most importantly the potential inadequacies of a system for the disempowered (Durrheim et al., 2011).
There thus appears to be a disjunction between the duties of the call takers and the realities of everyday practice. As Haugh (2013) points out there is a deontological element to interaction. The call takers in this instance should be accountable and committed to the business at hand – resolution of the call. Haberland (2007) notes that in stable multilingual communities, speakers in an interaction normally make language choices spontaneously without much negotiation. Our data suggest that the South African community may be less stable.
Language shift is an act with intention. The intention in this context should be call progression and the rapid despatch of an ambulance, but clearly obstacles exist. Responsiveness (Schegloff, 1986) is sometimes endangered and the implications of a delay in such resolution are serious and may have consequences for the caller and the entire system. While an emergency call can certainly not be construed as an everyday occurrence, there is a general expectation of collaboration in linguistic interaction that is missing in some of the calls, creating a mismatch between rights and responsibilities on the one hand and the realities of behaviour on the other.
These findings reinforce the work of Whitehead (2012) on racism in South Africa, who suggests from his data that race is recurrently reproduced as a taken for granted resource:
… it is evident that the participants are not setting out specifically to reproduce race. Instead, they are simply engaging in the business of everyday life, doing the sorts of ordinary things that people do (assessing, complaining, agreeing and disagreeing, and so on), and treating racial category membership as relevant for how they do things, and even for what they are doing. In this sense, race comes to be reproduced not as a result of participants’ active efforts to reproduce it, but instead as a ‘by-product’ of whatever actions they happen to be engaged in … (p. 1262)
Thus, what we appear to be seeing in some of these calls reflects the complexity of relations between groups of South African people. Microanalysis enables insight into macro-features of the context (Zhang, 2005) particularly given the unique demographic and identity issues of the Western Cape (Brown, 2000; Erasmus, 2001). As Zhang (2005) found in relation to Cantonese and Putonghua, the social structures relevant to the macro-sociolinguistics setting are validated by a microanalysis.
The methodology also enables implications for call centre training, which should focus not just on systems or even on certain linguistic features but also on attitudinal aspects, especially in what purports to be a non-racial society and a health care system governed by Batho Pele principles (Khoza and Du Toit, 2011). Analysis of such calls can be used to help improve language services in this centre and others.
It is hoped that such an attention to microanalysis can be turned into an effective framework for training. As Stokoe (2014) and others have done, this opens up the possibility of using applied CA as a mediation and intervention tool, utilising, for example, extracts such as the ones presented in this article as discursive material for training approaches. This research also highlights the need for further research into topics such as how language alignment builds trust in calls. The study has obvious application to other countries in Africa in which there are issues of linguistic diversity and large migrant populations.
Footnotes
Acknowledgements
This paper was originally presented at the European Association for Communication in Healthcare (EACH) Conference held in Amsterdam in 2014. The authors are grateful to Prof Kevin Whitehead for his insights and Ms Tshegofatso Seabi for assistance with transcription and translation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.