
Abstract
This study aims at examining the attachment states of mind in 50 female outpatients with eating disorders compared with 50 matched control participants using the Adult Attachment Interview. Moreover, the differences in attachment states of mind among eating-disordered women with and without borderline personality disorders’ diagnosis were explored. The results showed an over-representation of insecure-dismissing and unresolved states of mind in clinical group compared to controls. Patients with both diagnosis showed higher scores on involving anger and unresolved loss compared with those with only eating disorder. Implications for further research and clinical practice are discussed.
Introduction
Anorexia nervosa and bulimia nervosa
Anorexia nervosa (AN) and bulimia nervosa (BN) are considered the two main diagnostic categories of eating disorders (EDs). The core symptomatology of AN classified into (a) restricting and (b) binge/purging types consists of an intertwining of primary behavioral features and cognitions with mental and physical symptoms due to starvation and significantly low body weight in the context of age, sex, developmental trajectory, and physical health. There are both intense fear of gaining weight and disturbance in the way in which one’s body weight or shape is experienced (American Psychiatric Association (APA), 2013). Patients with BN display patterns of disturbances in eating behavior characterized by binge eating and inappropriate compensatory behaviors classified into (a) purging (e.g. vomiting and laxative use) and (b) non-purging types (e.g. exercising) accompanied by feelings of distress and/or concern about body weight or shape (APA, 2013). AN and BN individuals share fear of gaining weight, desire to be thin, and the level of dissatisfaction with their bodies, but while anorexic patients are underweight, bulimic ones generally have a normal weight or are moderately overweight (De Bolle et al., 2011). Although diagnostic criteria allow clinicians to detect individuals with a specific ED, many patients demonstrate a mixture of both anorexic and bulimic behaviors, or frequently, their clinical phenotype ranges from one pattern of ED to the other (Laghi et al., 2012). In a recent large European epidemiologic study, lifetime-estimated prevalence of AN and BN was 0.48 and 0.51 percent, respectively, and they were 3–8 times higher among women for both EDs (Preti et al., 2009).
As Allen and Dalton (2011) pointed out, both AN and BN are considered as a major problem with important physical and psychological consequences including limb and joint pain, headache, gastrointestinal problems, menstrual problems, shortness of breath, chest pain, role impairment, anxiety, depressive symptoms, substance abuse, increased mortality, suicide rates, perfectionism, obsessive-compulsiveness, neuroticism, negative emotionality, alexithymia, harm avoidance, low self-directedness, low cooperativeness, and low social interactions (Balottin et al., 2014; Bühren et al., 2014; Krug et al., 2013; Smink et al., 2012). Moreover, recent studies underline a moderate role of the gender in adolescents with AN, as well as negative perceptions of their family functioning and good performances in mindreading tasks, while bulimic patients revealed an impairment in their theory of mind (Laghi et al., 2014b, 2015a, 2015b).
Co-morbidity with other psychiatric disorders were highly common, including personality disorders, especially borderline personality disorder (BPD; Ramklint et al., 2010; Vrabel et al., 2010).
Attachment theory and EDs
Attachment theory is based on the theoretical proposition that early interactive experiences between the child and the caregiver are incorporated in attachment representation, defined as Internal Working Models (IWMs), which are initially relation-specific but then they generalize guiding attention, perception, emotion regulation, expectations, memory, and language of attachment-related experiences. The Adult Attachment Interview (AAI; George et al., 1985/1996) is considered as the “gold standard” measure to assess IWMs in adults, specifically defined as attachment states of mind. The core of the AAI scoring system is the construct of coherence intended as the interviewees’ ability to recount their attachment-related experiences in a believable, clear, relevant, thoughtful, and balanced way, independently whether their attachment relationships in childhood were positive or negative (Hesse, 2008).
In the last 20 years, the attachment theory and research has received increasing attention from clinicians and scholars seeking a relational understanding of several psychopathologies in adults (Steele and Steele, 2008). Dozier et al.’s (2008) hypothesis suggested that dismissing states of mind -characterized by low coherence in terms of incompleteness, lack of truthfulness, and discrepancy between semantic and episodic memory- would be expressed in disorders with an externalizing component, such as ED, conduct disorders, and hard-drug abuse, that might to be associated with a felt experience of minimization and derogation of attachment needs. According to Dozier et al. (2008), entangled states of mind—characterized by incoherence in terms of overwhelming prolixness, lack of relevance and clearness, and angry, passive, or fearful style—would be associated with internalizing disorders displayed in BPD and depression, as they share emphasis and maximization of attachment needs and experiences.
Regarding ED in the attacment perspective, 10 clinical studies, mostly with the AAI, and 4 reviews have recently been published (Cavanna et al., 2012; O’Shaughnessy and Dallos, 2009; Ward et al., 2000; Zachrisson and Skårderud, 2010). Most of them supported the Dozier’s hypothesis that females with AN and BN show dismissing states of mind (Barone and Guiducci, 2009; Cole-Detke and Kobak, 1996; Del Vecchio et al., 2014; Ward et al., 2001). However, some studies revealed that patients with ED often display both dismissing and entangled attachment states of mind or a prevalence of the latter, specifically associated with both the purging subtype of AN and BN (Candelori and Ciocca, 1998; Dias et al., 2011; Fonagy et al., 1996; Ramacciotti et al., 2001; Zachrisson and Kulbotten, 2006). Finally, a prevalence of unresolved states of mind with respect to loss and/or trauma, characterized by a collapse of monitoring of reasoning and discourse during the discussion of past loss and/or abuse, emerged among ED patients (Ringer and Crittenden, 2007). Attachment research showed that lack of resolution of past mourning and/or trauma was also highly associated with BPD diagnosis (Fonagy et al., 1996).
Understanding the quality of attachment states of mind of patients with ED can be clinically relevant, not exclusively with respect to the psychiatric diagnosis, but for providing useful information regarding the patient–psychotherapist relationship, the treatment’s outcomes, the reactions to separation during treatments, and the risks of drop-out (D’Onofrio et al., 2015; Lis et al., 2011). However, the attachment studies on ED reported some methodological and theoretical issues including very small sample size, lack of comparison between AN and BN, lack of non-clinical control samples matched for demographic variables, including mostly only inpatients with highly severe ED, considering only the AAI classifications, without paying attention to continuous AAI scales that can provide relevant clinical information. In addition to these, no studies up to now have considered the co-morbidity of ED with BPD, which is one of the most associated personality disorders.
This study is aimed at (a) replicating previous studies on attachment states of mind (AAI classifications and scales) in patients with ED using a non-clinical control sample matched for sex, age, education level, socio-economic status (SES), and comparing each ED diagnostic category (AN and BN); (b) comparing attachment states of mind in ED individuals with and without co-morbidity with BPD.
Methods
Participants
A total of 100 women were involved in this study. Participants with ED (n = 50; mean age = 20.06, mean years of education = 14.02, mean SES = 60.20) were consecutively recruited from the Eating Disorder Center (EDC) of Local Health Services 3 of Genoa, specialized for the treatment of ED. Outpatients were selected at intake from those who met Diagnostic and Statistical Manual of Mental Disorders’ (4th ed., text rev.; DSM-IV-TR; APA, 2000) criteria for AN (n = 25) or BN (n = 25), after the first interview with the clinical psychologists and/or psychiatrists at the EDC. The additional inclusion criteria were as follows: female sex, age between 16 and 25 years, and onset of ED within previous 2 years. Exclusion criteria were as follows: previous and/or current psychotherapeutic and/or medical treatments; concurrent severe psychiatric disturbance on Axis-I, such as psychosis, depression with suicidal risk, alcohol, or drug abuse.
Participants without ED (no eating disorder (NED), n = 50; mean age = 20.09, mean years of education = 13.98, mean SES = 64.20) were voluntarily recruited from community high schools and colleges and matched for all the demographic variables. The exclusion criteria for the control group were as follows: a current or past history of physical or psychiatric disorder both in participants and members of their nuclear family, previous and/or current clinical treatment for psychiatric symptoms, being over or underweight. All the participants were born and living in Liguria (Italy) with their family of origin, and none were married.
Measures
AAI
As mentioned above, the AAI is a semi-structured interview with 20 questions (George et al., 1985/1996). The AAI protocol requires the interviewees to provide both a general and specific description of the relationships with their attachment figures during childhood and following phases, with a special focus on attachment-linked experiences such as illness, being upset, hurt, separation, rejection, loss, and abuse. Moreover, AAI questions ask for reflection on their past and current attachment experiences (e.g. change in relationships, impact on adult personality, and reasons for parental behaviors). All interviews were audio-recorded and transcribed verbatim. The AAI Coding and Classification System (AAI-CCS; Main et al., 2002) is the most validated method for classifying the adult attachment states of mind, and it has been widely used with adolescent samples as well (Bakermans-Kranenburg and Van IJzendoorn, 2009). The AAI-CCS includes both scales and classifications. The nine-point scales were divided into two groups: (a) probable past experiences with each parent: loving, rejecting, involving role reversal, neglecting, and pressure to achieve; (b) current states of mind related to both parental figures (idealizing, involving anger, and derogation) and overall (overall derogation, lack of memory, meta-cognition, passivity, fear of loss, unresolved loss, unresolved trauma, coherence of transcript, and coherence of mind). Originally, the AAI-CCS assigned the transcripts to one of the three “organized” categories: free-autonomous (F), insecure-dismissing (Ds) and insecure-entangled (E). Successively, two further “not organized” categories were added: unresolved with respect to loss and trauma (U) and cannot classify (CC).
The validity of the AAI has been extensively demonstrated, showing both adequate reliability (e.g. short-term stability, inter-rater consistency) and discriminating validity with respect to possible confounds such as gender, verbal intelligence, memory, and social desirability (Bakermans-Kranenburg and Van IJzendoorn, 1993; Crowell et al., 1996).
In this study, all the AAIs were coded by a coder (VG) and for inter-rater reliability, 50 percent of randomly selected transcripts were also classified by another “blind” coder (D.C.). Both coders were trained by Debra Jacobvitz and Nino Dazzi in Rome, and they were provided with AAI’s reliability. They were unaware of the other data collected (e.g. clinical status, etc). The inter-rater agreement was 80 percent (k = .85; p < .001) across the AAI five classifications. Moreover, the scorings for the AAI scales were highly correlated, ranging from r = .54 for father’s derogation (p < .01) to r = .91 for coherence of transcript (p < .01).
Structural Clinical Interview for DSM-IV Axis I Disorders—Italian version
The Structural Clinical Interview for DSM-IV Axis I Disorders—Italian version (SCID-I) is a semi-structured diagnostic interview designed for the assessment of the primary DSM-IV Axis I disorders (mood episodes; psychotic symptoms; psychotic disorders; mood disorders; substance use disorders; and anxiety, adjustment, and other disorders) (First et al., 1994; Mazzi et al., 2000). The SCID-I was used as a diagnostic tool in order to confirm the diagnostic assessment obtained from the first interviews by EDC’s clinical psychologists and psychiatrists. Although its language and diagnostic coverage make the SCID-I particularly suited for use with adults (aged 18 years or above), its use with an adolescent population is also appropriate and only requires slight modifications (First et al., 1994). All the ED diagnoses were confirmed.
Structured Clinical Interview for DSM-IV Axis II Personality Disorders—Italian version
The Structured Clinical Interview for DSM-IV Axis II Personality Disorders—Italian version (SCID-II) is a semi-structured diagnostic interview designed for the assessment of 10 DSM-IV Axis II personality disorders, including depressive personality disorder and passive-aggressive personality disorder (found in the DSM-IV’s Appendix B, “Criteria Sets and Axes Provided for Further Study”) (First et al., 1997; Mazzi et al., 2003). As expected, 30 percent of ED outpatients (7 anorexic and 8 bulimic participants) were also diagnosed with BPD, which was the most common diagnosis on Axis II among ED females.
Symptom Checklist 90-Revised
Mental health symptoms of NED group were controlled using the Symptom Checklist 90-Revised (SCL-90-R), a 90-item standardized instrument designed to measure current symptom severity grouped in 10 main symptom dimensions (somatization, obsession-compulsion, interpersonal sensitivity, depression, anxiety, hostility, phobic anxiety, paranoid ideation, psychoticism, and other symptoms, such as problems with sleep) and a global index of psychopathology (Global Severity Index (GSI); Derogatis, 1994). This measure provides a reliable estimate of the likelihood of being diagnosed with a mental health disorder (T score above 63 for the GSI for any two symptom dimensions).
Socio-demographic questionnaire
Ad-hoc questions were developed for this research to collect personal data (age of birth, education level, etc.) and information concerning participants’ weight and height.
Procedure
All ED outpatients routinely referred to the EDC after intake could choose whether to follow the traditional consultation program or participate in the assessment procedure of our clinical research program. The assessment procedure comprised three sessions of about 90 minutes each to administer the SCID-I, the SCID-II, and the AAI by PhD students in clinical psychology. None refused to participate in the study. At the end of the assessment, we offered a report containing a synthesis of the outcome from each interviews to the outpatients.
The control group had been informed through the initial advertising that our research team needed females between 16 and 25 years old without physical or psychological pathology to participate as a control group in a clinical study. Control participants completed the SCL-90-R, the socio-demographic questionnaire, and the AAI.
The research protocol was approved by the Regional Ethics Committee of Liguria. All participants, or their parents if participants were under 18 years old, provided written informed consent to participate in the study.
Statistical analysis
All statistical analysis was performed using SPSS 21.0 software package. Descriptive statistics with means (M) and standard deviations (SDs) were calculated for continuous variables, with frequencies and percentages to describe categorical data. Given the small sample size and prevalence of ordinal (AAI scales) and categorical data (AAI classifications), we decided to use non-parametric statistics to compare attachment classifications of patients with ED and non-clinical controls, AN and BN groups, and eating-disordered women with and without BPD diagnosis (Mann–Whitney’s U, Chi square). As needed, the data analysis was carried out by categorizing the participants’ AAI classifications into the four-way system (F, Ds, E, and U/CC), forced three-way system (F, Ds, and E), and two-way system (F vs non-F, including Ds, E, U, and CC) for more powerful statistical tests. A p value of .05 was employed for all tests. Finally, regarding the AAI scales, we analyzed only those evaluating the current states of mind, because scales for inferred experience are difficult to interpret and are recommended only for use in the process of coding, not substantive analyses, given their dependence on current mood (Hesse, 2008; Pace et al., 2015a, 2015b).
Results
Descriptive variables
ED and NED groups were not different with respect to age, years of education, and SES (p values between .13 and .67, n.s.). Within the ED group, anorexic and bulimic outpatients did not differ significantly in any demographic variables (p values between .36 and .64, n.s.). As expected, groups differed in body mass index (BMI): outpatients with AN had a significantly lower BMI (M = 16.06, SD = 0.70) than outpatients with BN (M = 20.31, SD = 1.66) and healthy controls (M = 20.93, SD = 1.68) (df = 2, F = 92.80, p < .001).
The level of psychopathological symptoms of NED group by the SCL-90-R resulted highly under the 63 cut-off (M = 30.47, SD = 4.17), and none of the control participants scored above the threshold.
Attachment states of mind of ED and NED groups
Three AAI transcripts (one from AN outpatient and two from NED group) were excluded due to technical problems in the audio-recording.
AAI classifications
No significant differences were found between attachment classifications with respect to participants’ demographic variables (p value between .13 and .98).
Globally, outpatients with ED (F = 24.5%, Ds = 41%, E = 4%, U/CC = 30.5%) were more likely to be significantly classified as insecure than NED controls (F = 65%, Ds = 23%, E = 4%, U/CC = 8%, χ2 = 15.71, p < .001), and specifically they were more Ds (χ2 = 19.09, df = 2, p < .001) and U/CC (χ2 = 17.07, df = 3, p < .001) than their non-clinical peers.
No significant differences emerged between AAI classifications of AN (F = 25%, Ds = 46%, E = 4%, U/CC =25%) and BN groups (F = 24%, Ds = 36%, E = 4%, U/CC = 36%).
AAI’s current states of mind scales
As shown in Table 1, ED participants presented significantly higher derogation (mother and father) and anger toward the mother than NED participants with respect to states of mind related to parents. In addition, the ED outpatients obtained significantly higher scorings on overall derogation, lack of recall, passivity, and unresolved loss, and lower on coherence of transcript and coherence of mind compared to control group.
Means, standard deviations, and comparison of the AAI’s states of mind scales in ED and NED groups.
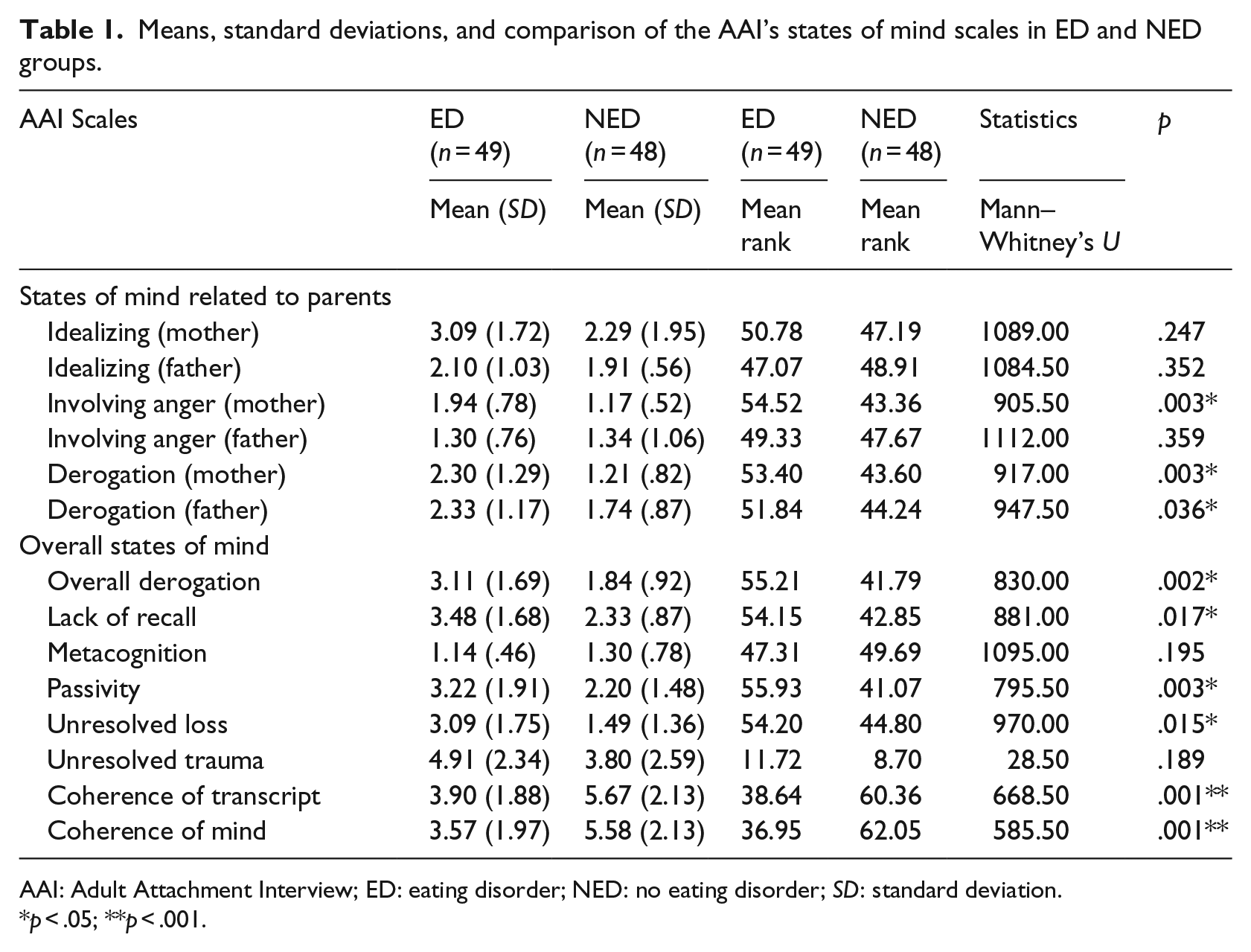
AAI: Adult Attachment Interview; ED: eating disorder; NED: no eating disorder; SD: standard deviation.
p < .05; **p < .001.
No significant differences were revealed between AN and BN groups with respect to states of mind scales (p values between .10 and .87).
Attachment states of mind of ED with and without BPD co-morbidity
As mentioned above, from the ED group, 30 percent of the outpatients (n = 15, 7 anorexic and 8 bulimic) were also diagnosed with BPD. Therefore, ED/BPD participants (n = 15) were compared with ED/non-BPD ones (n = 35) with respect to their attachment states of mind.
AAI classifications
Although outpatients with ED/BPD were more likely to be classified as insecure (F = 13%, Ds = 33%, E = 7%, and U/CC = 46%) than ED/non-BPD ones (F = 29%, Ds = 44%, E = 3%, and U/CC = 24%), no significant differences were revealed.
AAI’s current states of mind scales
The ED/BPD group showed significantly higher scorings on involving anger toward mother (mean rank = 65.37, Mann–Whitney’s U = 172.500, p = .018) and unresolved loss (mean rank = 58.97, Mann–Whitney’s U = 174.000, p = .020) scale compared with the ED/non-BPD group (mean ranks: anger mother = 49.74; unresolved Loss = 48.07).
Discussion
First, our results revealed that female outpatients with ED showed more insecure classifications, mostly dismissing and unresolved, than non-clinical controls matched for sex, age, level of education, and SES, supporting some previous findings.
The prevalence of dismissing state of mind in our clinical sample seems to be in line with Dozier et al.’s (2008) hypothesis suggesting that individuals with externalizing disorders and outward focus, like patients with ED are, would go together with a more dismissive stance to their own attachment experiences and a deactivation/minimization of the attachment needs and feelings. Specifically, ED participants in this study presented, beyond low coherence of transcript and mind, high scores on Ds-like scales of derogation (maternal and global) and lack of recall rather than idealization of mother, suggesting that they may be able to report some adverse childhood experiences without access both to episodic memory and to the negative emotions associated with them (e.g. fear and anxiety). In other words, their IWMs can sound like “Something negative is happened to me, but it is really a silly thing” and/or “Stop past memories” than “Everything was perfect in my childhood.” Furthermore, outpatients with ED showed higher scores for involving anger (mother) and passivity of thought scales, which are usually associated with E classification. Although these findings may seem contradictory, they may be consistent with a clinical approach which revealed that attachment classifications must not to be considered as mutually exclusive, as every dismissing patterns could contain an entangled subliminal stance, and vice versa (Steele and Steele, 2008).
The over-representation of unresolved states of mind with respect to loss among patients with ED supports previous studies and seems to be in line with results on clinical samples both in international and Italian meta-analyses (43% Bakermans-Kranenburg and Van IJzendoorn, 2009; 36% Cassibba et al., 2013). Furthermore, a theme of unresolved loss would be consistent with the clinical literature, which emphasizes early separation difficulties in the etiology of EDs (Ward et al., 2001).
No significant differences emerged regarding AAI classifications and scales comparing AN and BN groups. This result did not confirm the hypothesis by Candelori and Ciocca (1998) that deactivating attachment strategies should prevail among restrictive ED AN, while hyperactivating ones should be more common among purging ED subtype (BN and purging AN). Indeed, our results may support the hypothesis that despite the behavioral differences between AN and BN, their inner world – specifically their attachment states of mind or, in other words, their IWMs – could be more similar than different, consistently with studies revealing the continued oscillations between AN and BN diagnosis inside the clinical groups with ED.
The second purpose was to compare attachment states of mind in ED individuals with and without co-morbidity with BPD, although the small size of the ED/BPD group means that the results should be treated cautiously. We found that outpatients with diagnosis of ED and BPD were also characterized by higher scores on anger toward mother and unresolved loss scales than patients with exclusive ED diagnosis. These data suggest that the attachment states of mind of patients with ED/BPD move from dismissing strategies toward difficulties in affect regulation with amplificated attachment needs (E-like traits) together with an inability to integrate significant losses in a coherent representation, often revealed among BPD patients. We would suggest that taking into account not only the “traditional” categorical classifications of the AAI but also the dimensional scales assessing specific states of mind could be in line with the debate brought by the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5) which, compared to DSM-IV, moved from a categorical perspective toward a more dimensional one.
Furthermore, our results may have some clinical implications with respect to the planning of the treatments and the risk of dropout. For example, dismissing patients seem to improve better in setting like brief psychoanalytic therapy, while entangled patients would build a good therapeutic alliance in highly structured setting as transference-focused psychotherapy (TFP; Steele and Steele, 2008). Moreover, dismissing patients could be at risk of dropout because they are not able to become fully involved, attached, or committed with the therapist and/or treatment or, conversely, because they find that psychotherapy mobilizes them too emotionally. In contrast, patients with an entangled state of mind could leave the therapy whether they lived experiences felt as an abandonment, that is, the cancelation of a session for an emergency and programmed holidays (Obegi and Berant, 2009). Finally, patients with unresolved states of mind, especially if added to insecure organized classifications (Ds and E), deserve special attention because they could feel ambivalence, fear, and confusion toward a therapist able to act as a secure base (Wallin, 2007).
These results should be interpreted in the context of several methodological limitations. First, sample size was small and comparisons involving different diagnostic subgroups of participants with ED (e.g. AN, BN, ED/BPD, and ED/non-BPD) should be viewed as tentative. Second, the cross-sectional design precludes firm conclusions regarding causal relationships between attachment states of mind and ED. Third, we are not able to test the potential moderating role of BPD classification on the association between ED and AAI ratings, because a sample of BPD patients without ED was not included in our study. Fourth, we included outpatients from one ED center only, so results may not be generalizable to ED patients as a whole, for example, inpatients or non-clinical populations (Laghi et al., 2014a). And finally, a gender comparison for attachment in eating-disordered patients, with and without BPD co-morbidities, deserves further analysis in future research. In conclusion, even if our results are interesting, they are only explorative, and further studies will be required to confirm them.
Despite these limitations, Waller et al. (2015) pointed out that the strength of this study was that we used the AAI “a highly elaborated method that not only allows assessing the mere occurrence of self-reported childhood trauma experiences but also the degree to which traumatic experiences are mentally resolved” (p. 8). From a clinical perspective, it may be beneficial to consider attachment state of mind assessed by the AAI during the clinical assessment of patients with ED, with and without co-morbidity with BPD, as it may shed light on the ability to engage patients in treatment relationships and also may provide some insight into potential vulnerability for rupture of patient–therapist relationship and better specialized interventions (Dazzi and Zavattini, 2011; Pace et al., 2015a).
Footnotes
Acknowledgements
The authors are grateful to participants for getting involved in the study and for telling us about their lives, a task that was sometimes hard to complete. They are also grateful to the psychiatrists, psychologists, students, and internships for their help with data collection and for transcribing the interviews.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
All procedures followed were in accordance with ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000. Informed consent was obtained from all patients included in the study.