
Abstract
Many women with gynecological cancer report psychosocial distress, and clarification of the risks, vulnerabilities, and protective factors is required. The aim of this study was to investigate the lived experience of gynecological cancer patients and to understand the factors that underlie psychosocial distress. Semi-structured interviews with seven women diagnosed with gynecological cancer revealed the role of social support, or its absence, selective withholding of information, and existential loneliness in women’s experience of distress. Social support provided a buffer against distress, while feelings of alienation and being alone exacerbated distress. Interventions to address these concerns may lead to improved quality of life for this patient group.
Gynecological cancers account for one in six female cancer cases globally (Ferlay et al., 2013) and include malignant tumors of the vulva, vagina, cervix, uterus, ovaries, and fallopian tubes. In Australia, approximately 1 in 23 women will be diagnosed with a gynecological cancer by the age of 85 years, with the 5-year relative survival rate at 67 percent (Australian Institute of Health and Welfare & Cancer Australia, 2012). As well as the threat to life such a diagnosis can represent, these women may undergo invasive treatments resulting in scarring, treatment-induced menopause, and infertility (Poluszny et al., 2011). Despite advances in disease control, and apart from the physical impact of gynecological cancers, there are generally negative emotional consequences of such a diagnosis for both patients and their families (Bultz and Holland, 2006). Gaining a deeper understanding of this and developing supportive care strategies for patients and their families has become increasingly important as diagnosis rates increase, and women live longer following diagnosis (Australian Institute of Health and Welfare & Cancer Australia, 2012).
Several correlates of distress in gynecological cancer patients have been identified. The impact of gynecological cancers on sexual functioning appears to be a risk factor for distress (Goncalves et al., 2008). The reasons for this are unclear but concerns about altered appearance have been associated with distress in this patient group (Johnson et al., 2010), and self-perceptions of femininity may be negatively altered by treatment. Furthermore, in a qualitative study, Ekwall, Ternestedt, and Sorbe (2007) found that some women feared rejection or abandonment and experienced feelings of isolation and vulnerability.
Such feelings of distress may be associated with the cancer site. The diagnosis and treatment of cancer of the reproductive organs can pose particular challenges for women. For example, as the female genitals are considered “private,” using their anatomical names in conversation is generally considered taboo (Wray et al., 2007). For some women, sexual connotations of the cause of their cancer made disclosure to others challenging and discussion of treatments embarrassing (Wray et al., 2007).
Poor perceived social support is also associated with increased distress for women with gynecological cancer (Hipkins et al., 2004). Their relatively low prevalence means few support groups exist and, as there have been few public stories about celebrities with gynecological cancers, little public discussion about these diseases has occurred (Pistrang et al., 2012). In fact, some affected women have described gynecological cancer as a “forgotten cancer” (Wray et al., 2007). Feeling unable to disclose their cancer story may contribute to the psychosocial distress experienced by some women, who reported not sharing their fear of dying and sadness with others (Ekwall et al., 2007). Furthermore, women have described concern for the wellbeing of those close to them, conveying sadness and feeling responsible, in part for developing the disease, and later for disseminating or withholding information to protect others (Ekwall et al., 2007; Johnson et al., 2010; Steele and Fitch, 2008).
As many of the physical and demographic correlates of distress in women with gynecological cancer are not amenable to intervention, more clarity on the modifiable risks, vulnerabilities, and protective factors is required to improve supportive services. Accordingly, the aim of this study was to gain a deeper understanding of the psychosocial factors that contribute to or assist in alleviating the distress that women experienced as associated with their gynecological cancer diagnosis and treatment.
Method
An iterative thematic analysis (Braun and Clarke, 2013) qualitative research design was thus employed to elicit and interpret women’s narratives of gynecological cancer.
Participants
Women were eligible to participate if they had been diagnosed with a gynecological cancer (first or subsequent diagnosis) within the previous 5 years, were over 18 years of age, and spoke English; the preceding are inclusion criteria and no additional criteria were used. A total of 10 women volunteered to participate in the study; 2 did not take part due to health reasons and 1 withdrew prior to interview for unspecified reasons.
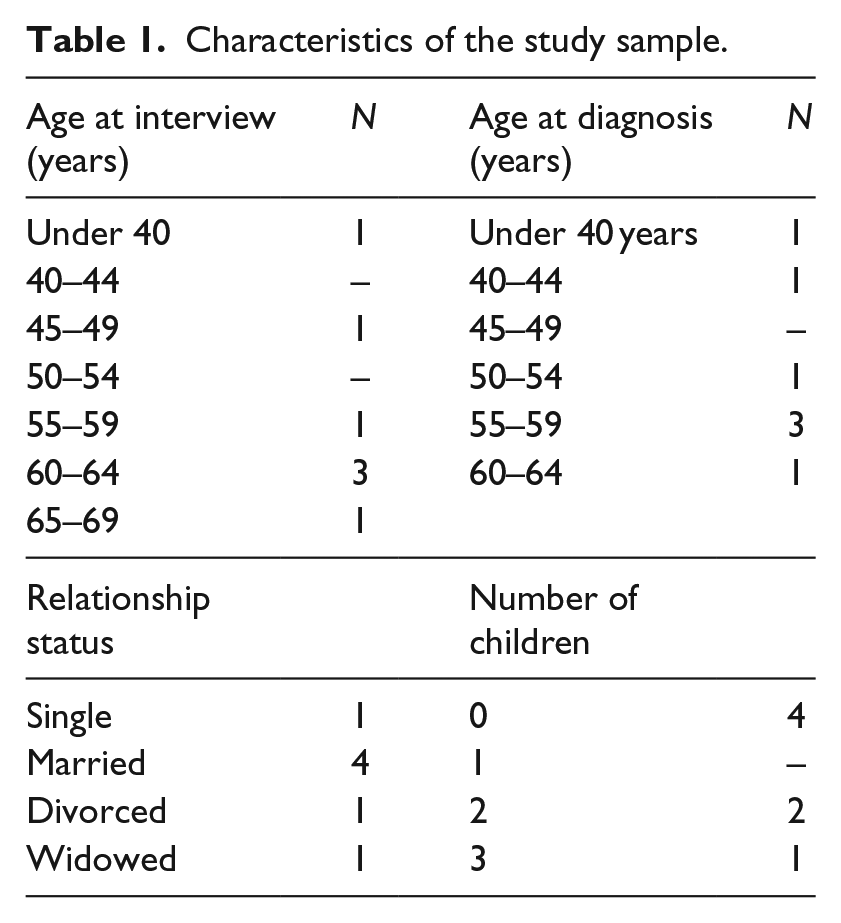
Seven women aged 35–65 years (mean age: 55.3 years; standard deviation (SD) = 10.3) participated (see Table 1). Five were peri-menopausal at the time of their diagnosis (mean: 51.7 years; range: 33–61 years). Participants were all Caucasian, and all identified as heterosexual. Two participants were employed, and five had obtained post-secondary qualifications. Six had received their first gynecological cancer diagnosis within the previous 5 years; the remaining woman had first been diagnosed 10 years prior, with a subsequent diagnosis occurring within the 5-year timeframe (mean duration: 46 months; range: 12–124 months). Our sample included four women with ovarian cancer: two with cervical and one with endometrial cancer. One reported her cancer as stage I, four as stage III or IV, and two were unsure of the current stage. All had received at least one form of treatment, most commonly surgery (n = 7), followed by chemotherapy (n = 6) and/or radiotherapy (n = 4).
Characteristics of the study sample.
Procedure
The study was approved by one Hospital and one University Human Research Ethics Committee. Cancer consumer organizations placed recruitment notices in their offices, print media, and on electronic media; interested women contacted D.M.M. directly, at which time they were given information about the research. Prior to their one-off individual face-to-face interviews (with D.M.M.; mean duration: 69 minutes; range: 52–96 minutes), participants provided informed consent. A semi-structured interview schedule was developed based on a comprehensive literature review and the clinical insights of the research team. All seven interviews, conducted in participants’ homes, were recorded and transcribed verbatim. No compensation was offered to participants.
Data analysis
Data analysis followed Braun and Clarke’s (2013) six-stage thematic analysis approach. Interview questions iteratively evolved over time, allowing the inclusion of new issues in the question schedule as they were introduced by participants. For example, as women described the significant negative effects of breast cancer awareness-raising, we added relevant questions to the interview schedule.
Data coding was conducted by D.M.M., through extensive consultation with N.W. throughout each stage of analysis. Stage I, data familiarization (stage I), occurred through transcription and repeated readings of transcripts. Initial (unstructured) coding (stage II) was undertaken following each interview, to further facilitate iteration. In this, transcripts were analyzed and examined for patterns and recurrent themes. The third stage involved systematic coding, where recurrent themes were identified. Codes were then refined (stage IV), and redundant codes were removed from the code dictionary. To this point, all coding was cross-checked by the first two authors (N.W. and D.M.M.). We agreed on all but approximately 10 percent of codes; the differences led to discussion and a subsequent adjustment of the definitions of approximately 10 percent of codes. Codes were then discussed by the whole research team and grouped under conceptual ideas (stage V); the four predominant themes were identified (reported below, stage VI). Because of the relative homogeneity of the sample in terms of sociodemographic factors, informational redundancy occurred when no new data were revealed in subsequent interview text (Guest et al., 2006) and recruitment ceased. NVivo software (QSR International, 2012) was used to manage the interview text. To maintain privacy, participants were assigned a pseudonym.
Results
Overwhelmingly women spoke of the importance of social factors in their experiences of gynecological cancer, both around the time of diagnosis and through treatment.
Social support through social networks and via organized support groups was important to each participant. In particular, family and friends (which we term “social network support” here) were integral to participants’ experiences with cancer. Many of the women recalled the response from others following their diagnosis as very positive and giving rise to a perception of being “supported” and “carried.” When women spoke of this type of support, they emphasized their experience of feeling included and remembered. One obvious demonstration of this was the beneficial nature of actual physical closeness and the company of friends and family. For instance, after Julia was advised of her diagnosis, she sent out a text message:
[It said] “I’m going to the pub” and … probably about 30 people came down … It was like this massive instant reaction [of] “we’re surrounding you and we’re going to be with you through this,” so that’s pretty amazing.
Similar instances of beneficial physical proximity were recalled by other women, particularly after telling others of their diagnosis. Linda described how her sister arrived the following day from interstate, “which was lovely because she spent Christmas with us, and we normally don’t get to spend Christmas together.” Similarly, for Charlotte, “as soon as I was diagnosed, within a week we had a girls’ night, and we as a group stay in very close contact now.”
This social support was reported as being positive and affirming. However, other participants recalled such demonstrations of affection with mixed emotions. For instance, Evelyn described how everyone she knew came to see her, so she received a visitor every day for 6 months. Concern and “an enhanced honesty” marked these encounters; although a “tremendous support,” she found these encounters were bittersweet as it “makes you want to live all the more, of course.”
For all participants, ongoing connection with and inclusion by their social network was demonstrated through the provision by others of practical support. Food seemed to be the universal token of social support: “We had pots of soup arrive every day. I think everyone that gets cancer gets a lot of soup. Lots of soup” (Evelyn).
Such support extended to other chores, particularly when women were feeling unwell during treatment—“I relied on people to do shopping for me” (Anne)—and extended to assisting with household duties, as Dorothy explained: “So [my friend] came over and did the house, and her husband came over and did my lawn.” Many relied upon others to drive them to appointments. Gestures of practical social support were usually unsolicited and were sometimes resisted at first, as Julia described:
I’ve always known I’ve got great friends, but you always kind of wonder “why does [he or she do] this?” but I stopped wondering why, and just accepted that these people just loved me, you know, for the same reasons I love all of them I suppose. But it was just so nice.
All participants reported that they eventually came to accept and welcome most of the interaction with their social network. In some instances, however, the support was unwelcome:
When I first was diagnosed, [my friend] heard about (it) and she called me and she said, “don’t go to the surgery, chemotherapy will kill you … If you’re doing chemotherapy you’re going to die, if you go to radiotherapy, it’s definitely a death sentence.” (Helena)
Social support was not always something that participants received out of the blue, and some women spoke of actively seeking social support. For instance, Charlotte told others of her diagnosis so that she might receive support, “if people don’t know what’s going on for me then … they can’t support me.” Others had no choice but to reach out for assistance from friends. Dorothy, who lived in a regional country town where formal support—modes of support that are administered by funded health or medical services and agencies, which may be delivered by paid professionals or volunteers—was limited, supplemented the transport services provided by the Red Cross by “[asking] people I knew around here and they ended up taking me half the time.”
Other women reported mixed experiences of accessing, utilizing, and feeling included in consumer support networks, and most had at some point contacted such groups. This type of support was perceived as invaluable: “there is a level of knowledge that you can only have when you’ve had it yourself, when you’ve had that diagnosis” (Evelyn). The sense of inclusion in a peer support group and of shared experience was, for some participants, vital to their emotional wellbeing: “I feel extremely free to talk in my support group because I know people will understand me better. They [all tell] more or less into the same story” (Helena). Despite the benefits offered by sharing their stories, not all women experienced this form of social support.
When support is not available
Several women spoke of the difficulties of finding appropriate formal support, such as with same age peers or people with the same diagnosis as their own. For younger women, this was particularly problematic. In her early 40s, Charlotte felt caught between two types of gynecological support groups: she was too old for the young adult cancer support groups, but her story was different to those of the members of gynecological cancer support groups due to her comparative youth. This left her feeling isolated:
“I was nowhere. I was in no-man’s land as far as finding a group to support me as well.”
For Julia too, a sense of otherness was apparent as she discussed her inability to identify age peers with the same diagnosis as herself,
“Well it’s not that there’s a gap in the service, there just may not be anyone [else].”
The specificity of support groups further contributed to women’s reported isolation, especially for low-prevalence or high-mortality cancers. Evelyn explained that this could be a disconcerting experience in itself:
I mean you’ve only got to go to ovarian cancer events and there’s just hardly anyone there. That’s one of the reasons why I’m happy to contribute to the research, because there’s not a lot of people around who are well enough, or still alive, to talk about it.
This highlighted a tension between some women’s accounts: although they wished for support from other women with shared experiences, they actively sought to only gain support from others with the same diagnosis in order to protect their own wellbeing. Charlotte, for example, decided to “box herself” and only seek support from those who were also diagnosed with endometrial cancer, away from those diagnosed with ovarian cancer in recognition of the different prognoses:
[T]he support groups that are out there for women with gyne[cological] cancers aren’t that strong unless you’ve got an ovarian cancer, and I didn’t have that, and the outcomes for ovarian cancer are so poor really … I kept on trying to say, “well that’s not me.”
Accordingly, for women with a gynecological cancer other than ovarian cancer, the options for what they perceived as positive peer support may be very limited.
Attempts were made by all participants to compensate for the paucity of gynecological cancer-specific services by accessing those provided for women with breast cancer, which occurred in recognition of the significant variations in the support offerings between the different cancers (noted by five participants). While they took advantage, to some extent, of the more comprehensive services provided for women with breast cancers, this led to feelings of disappointment, envy, and anger:
All that Pink Ribbon shit and all that, you know. I think it [breast cancer] definitely does get all the, all the profile. Nobody seems to care about it [ovarian cancer] because it’s a little bit rarer … but the thing is it’s a lot more dangerous. (Anne) Honestly, I’m a bit over pink. I get a bit anti-pink. Oh, it’s a joke really, because um, they get, pink gets everything we always say. (Evelyn)
Compounding the women’s difficulties with locating and accessing appropriate services for their “forgotten cancer,” this sense of experiencing the “wrong” female cancer left women feeling excluded from a broader community of support:
You see things like the groups that do dragon boat racing and things like that, and you think if I rocked up and said “I’ve had cancer, but not breast cancer, would you let me in?” You know, there’s kind of, not a closed group, but do you have to have gone through that particular experience to, to meet the criteria … I’ve had a lot of the experiences, but not the pink experience. (Charlotte)
Disclosing diagnosis and the selective withholding of information
Talking with others about their cancer diagnosis was an important element of gaining support, and all participants had freely told their family, friends, and workmates about many aspects of their cancer experience, including the site of the primary tumor. It was evident, however, that while women described being open with others, they had simultaneously engaged in a process of selective withholding of aspects of their diagnosis, treatment, and side effects from others. This occurred for several reasons.
Some women chose to withhold information about the loss of control over their bodies that occurred during the invasive procedures they endured. For example, while recalling the diagnostic process, Charlotte disclosed that a radiation technician walked into the room and inserted a barium-coated tampon into her vagina without warning or discussion and without any specific consent that she recalled. She had not told anyone about this experience prior to the research interview. Similarly, the highly invasive treatment, brachytherapy, was equated with “medieval torture,” leaving Julia to describe the experience as: “I felt as though I’d been fucked with a fishing knife.” Although open with her large friendship group about most aspects of her cancer care, Julia explained that she only disclosed this aspect of her treatment to her closest friends because “I don’t think a lot of people would handle it, to be honest.” She also had not posted anything on gynecological cancer blog sites because “I’ve never wanted to scare anyone.”
The association with female sexual and reproductive organs made it difficult for Charlotte to discuss her diagnosis with others and partially explained why she felt unable to discuss her ongoing need to use a vaginal dilator. At first, she had joked about it with friends, but no longer mentions it. As a result, Charlotte did not believe her friends were aware that she continued to need a dilator, even though she was able to discuss her other physiotherapy needs with them. Other women spoke of similar patterns of selective withholding, freely discussing the commonly experienced peripheral neuropathy with acquaintances, yet withholding more “personal” side effects such as vaginal discharge, vaginal dryness, and constipation.
Younger women found that treatment-induced infertility brought particular conundrums. Julia was unable to talk about her cancer at all for a period of time as a result of this loss. The cancer itself was “just no big deal medical problem,” but for Julia, it was not possible to “talk about one [aspect: cancer] without the other [infertility].” While she resolved her ability to discuss her cancer, the loss of fertility continued to be problematic during her social interactions. In particular, her infertility had implications for forming romantic relationships:
Another issue I have with people, and particularly dating … is do I tell people first up that I’ve had cancer? If I do tell them, when? Do I tell them I can’t have children? If I do tell them, when? Like is it better to be just right up front and tell people at the very beginning? Or do you wait until the issue comes up?
In contrast, Helena made the decision to withhold information motivated by a desire to protect others and/or self:
[T]o discuss the medical treatment with people that [have] never [had] ovarian cancer, it’s a little bit too much, I think, for them. I prefer to discuss with them about symptoms and regular checks instead of talking about … the treatment and all this personal things that happen to me.
Withholding information also appeared to have different functions at different times and was tailored according to the person being addressed. For instance, at the time of diagnosis, Helena was not experiencing physical symptoms and was grappling with the implications of gynecological cancer. As such, she chose not to tell anyone about her diagnosis: “[those] two weeks … were awful for me. I didn’t know actually what’s going on, I didn’t know what to tell them.” For some women, the choice not to discuss aspects of their experience served to protect their identity as being more than a gynecological cancer patient and also provided some relief from thinking about cancer:
I just don’t want to be defined by cancer and that’s all I ever talk about … that’s one of the reasons that I don’t go to formal support groups, “cause I don’t want to sort of wallow in it … it could be your every waking hour.” [For] some people it is, it’s almost like it’s the greatest thing that’s ever happened to them you know, and I just don’t want to be defined by it. You are anyway, every time you see somebody and they say “how are you?,” you know what they mean. (Evelyn)
For Linda, keeping her chemotherapy-induced baldness entirely private was a priority in her effort to cope with the associated distress:
I’ve always been very proud and very keen to make myself look the best that I can, so I never showed, there wasn’t another person that actually saw me without my hat or my wig on. Not even my husband. I always wore a little hat to bed, I never ever showed a soul, and I was completely bald … I could never go there.
Protecting others through withholding information was a recurring theme. The decision to withhold information was specific to certain people in their network, relationships, and contexts. Two women spoke of withholding information about their diagnosis and prognosis, but for very different reasons. Anne had advanced disease but withheld this from her siblings: “I haven’t told them how serious it is … I don’t want to upset them too much.” In contrast, Linda was diagnosed with ovarian cancer at stage I and had an excellent prognosis, so she withheld this information from other ovarian cancer patients:
It’s not something that I share readily because I’m very aware of that, that [it] is unusual and the majority of women have a much more significant diagnosis. So, I only say if I am asked directly, because I don’t want to make them feel … any worse than probably they already do feel.
When women spoke of withholding information to protect others, it was evident that, in the process, they were also protecting themselves. They withheld information which they believed may be distressing for others to hear, but this was often also upsetting to discuss. Anne chose not to discuss her prognosis with others “because it’s just upsetting to talk about, and you know I don’t want to trouble other people, or lose control in front of other people … I just say I’m okay now.” This had ramifications for her romantic relationship: “I’ve distanced myself a bit from him recently, because you know, I don’t want him to get involved in my problems.”
By withholding the negative aspects of her experience, Linda tried to make sure that others would not be too worried, and this helped with her own cancer journey:
When I would talk to others, I would just talk about the facts and talk about the positive side and um, what was happening. Yeah, so that’s how I coped, and also it worked with my family members and friends in the way that I did that.
Talking of their own mortality was an aspect of their experience that the women could not address with others. For instance, what worried Charlotte most about dying was “how it would affect the people around me, not what it was for me. It was … about the people that I was going to leave behind.” However, she had never raised this or discussed her concerns about dying with others. Charlotte was not alone in this: even when surrounded by people they love, women often felt alone with thoughts and fears they were unable, or unwilling, to share.
Existential loneliness
During times of uncertainty, prior to and following diagnosis, participants attempted to control information, one of the few things they felt they could control. However, this exercising of control sometimes burdened them with the weight of negative thoughts that they subsequently felt they must carry alone. This withholding of information could exacerbate the sense of aloneness experienced as women endured cancer treatment and associated side effects:
It’s a very … I don’t want to say lonely, because everyone’s experience is lonely regardless of your age, but it’s a very solo journey though, because I don’t feel I can … share, just to have that innate understanding of someone who knows exactly what you’re talking about. (Julia)
This sentiment was woven through many participants’ narratives. Even while reporting significant social support, many women described a sense of alienation and feeling alone. This loneliness was described by several participants:
Just being on your own, I think is … what I found the hardest. Being here, in here [inside your head] too long by yourself, it means you just think too much. (Dorothy) The whole thing about it is that I am alone. There’s nothing anyone can do for me … nothing’s going to change that. I’m totally, totally on my own, and no matter how many people are nice to me, how many friends come round and bring me shit, and talk to me, and say “let’s go for a coffee,” that’s not going to take that away … No matter … how many people say, “think positive,” “you’re alright,” “let’s do this, let’s do that,” “let’s go to a movie,” that’s not going to change anything, that’s not going to stop me feeling alone. (Anne)
It was through accepting her mortality, regardless of her cancer, that Helena found relief and peace in the face of existential loneliness: “we [are] all going to die anyway, but if there is something you may enjoy to doing by then, then do it.” Through her journey to this acceptance, she resumed living her life, as opposed to waiting for her death. This was not the case for other women. The life-limiting nature of their diagnosis was the source of much of their distress. Women’s experiences of “being given a diagnosis of death” and the uncertainty they subsequently experienced, brought “inner turmoil” (Charlotte). Indeed, Evelyn found this the most challenging aspect of her ovarian cancer diagnosis:
[The hardest part is] the mortality. It’s the fact that you might die. I say might die now, but you know it’s almost probably die at times … No one will ever, ever say to me, “Well that’s the end of that [Evelyn], it’s gone.” They will never say that, they will never say that they’ve got all the cancer, because they can’t.
Many of the women had been advised that their life may be shorter than they had expected. The co-existence of holding this knowledge and the decision to withhold it from others seemed to further exacerbate the women’s sense that ultimately they were alone.
Discussion
The participants in this study gave largely positive accounts of social support received through their existing social networks. This support appeared to ease the physical and emotional burden for the women, alleviating their experience of psychosocial distress. The notion that social support is protective against potential distress in the context of illness has been widely discussed in the psycho-oncological literature (Alferi et al., 2001; Helgeson and Cohen, 1996; Wenzel et al., 2002) and is consistent with the work of Poluszny et al. (2011), who found that a person’s knowledge that they can count on others was the most important factor in long-term wellbeing post-gynecological cancer diagnosis. In this study, participants also sought more formalized support through peer support groups; however, due to the specific support needs of women with gynecological cancers, effective peer support is dependent upon sentiments of shared experience (Pistrang et al., 2012). Where women in this study were able to locate a support service that facilitated some sense of shared story, the benefit of empathetic social support was evident. This was not unproblematic: all participants of this study reported challenges in locating services that met all of their specific needs, leaving them feeling socially isolated within the cancer community.
These findings on access to appropriate support raise concerns for women who are not able to engage in empathetic interchange around their cancer experience and also highlight the need for support services to carefully attend to the composition of support groups. This supports Pistrang et al.’s (2012) findings that when the experiences of women in a peer support relationship were not closely enough matched (particularly by treatment, treatment side effects, and personal background), the benefit gained through the reciprocity of exchanges—for both the peer support provider as well as the recipient (Pistrang et al., 2013)—was reduced when compared to pairings between women with a similar history. In particular, well-matched support was seen as increasing women’s sense of hope for the future, giving them a sense of confidence to recreate a meaningful life (Pistrang et al., 2012).
The resulting sense of alienation was exacerbated, for many women, when they became aware of the breadth and availability of services for women with breast cancer. Bell (2014) argued that successes in breast cancer advocacy have led to a widespread delegitimation of most other types of cancer, compounding the sense of psychosocial distress experienced following diagnosis and during treatment. Yet, the gendered experience of women’s cancers may have impacted here: Sekse, Gjengedal, and Raheim (2013) found that gynecological cancer survivors experienced their changed bodies in a very female way, as the cancer and its treatments were focused on the sexual and reproductive organs. Certainly, the idea of a gendered experience of cancer was embedded throughout the narratives collected in this study and was made stark by the comparison with breast cancer survivors. In light of women’s statements that they felt like outsiders within the female cancer community, it seems likely that experiencing the disparity in services may compound the sense of alienation experienced by gynecological cancer patients.
Psychosocial distress could not be predicted through a simple consideration of whether appropriate support was available or not, and a “dialectical tension” (Broom and Tovey, 2007) arose in women’s accounts. This concept highlights the ways in which social support had both buffering and impeding effects on women’s lives and requires further consideration in helping women to adapt following their gynecological cancer diagnosis. This was notable in the processes of selective information withholding that participants engaged in, as well as in their feelings of existential loneliness.
All participants in this study revealed aspects of their cancer experience that they felt they must withhold from others. This finding extends the insights of previous studies (Cullen et al., 2012; Ekwall et al., 2007; Johnson et al., 2010; Wray et al., 2007) and suggests that the decision to withhold specific information is multi-functional and dependent upon both content and context. Not only did women withhold difficult experiences, thoughts, and feelings from their friends, family, and colleagues, they also withheld information from other women with the same diagnosis. Not only does this impact the peer support relationship, but more importantly, may have consequences for managing individual women’s survivorship. For instance, an inability to discuss side effects with healthcare providers may limit their management; reinforce a sense of being alone; and limit the benefit of the shared story of peers. As such, processes of selective withholding of information may have broad implications for the psychosocial burden of women who feel they must carry the weight of this information alone.
The benefit of, and search for, social support juxtaposes diametrically with the sufferance of social isolation, alienation, and being alone. For some women, the realization of their mortality exacerbated their sense of isolation, resulting in feelings of existential loneliness. In this study, consistent with prior research, many survivors of gynecological cancers harbored existential concerns, which remained largely out of reach of current psychosocial interventions (Steele and Fitch, 2008; Urbaniec et al., 2011). The authors of earlier studies found that, of the unmet needs identified by women with gynecological cancers, those pertaining to existential survivorship, such as coping with changes to beliefs that nothing bad will happen to them and fear of recurrence, were most frequently unmet. It is reasonable to suggest that fear of recurrence and the discarded belief that nothing bad will happen are related to concerns about dying. For women living with the threat that gynecological cancer represents, the consequential psychosocial distress experienced may, at least partially, be explained by their experience of existential loneliness.
The findings of this study provide further evidence to recent literature highlighting the contribution of cancer-related and non-cancer-related factors to the experience of existential loneliness in the context of cancer. A systematic review by Deckx et al. (2014) identified the contribution of temporal (younger age at diagnosis and greater time since diagnosis) and social (unmarried and/or with limited social support) factors to heightened experiences of loneliness following cancer diagnosis. It is worth noting that while cancer-specific factors played a limited role (Deckx et al.), as our findings elucidate, access to psychosocial support was shaped by cancer-specific factors, particularly in terms of the type and site of cancer. Despite the pessimism that may accompany a discussion of existential loneliness, our findings highlight the potential for psychosocial interventions. Mayers and Svartberg (2001) explored the relevance of this concept for women infected with HIV and found that women’s expressions of existential loneliness held particular utility with regard to understanding their distress, and therefore offers opportunities for psychotherapeutic intervention. As Helena found, it was only through the acceptance of her mortality and the certainty of her death that she found peace, even in the uncertainty of her cancer prognosis. Exploration and elaboration of notions of existential loneliness may offer significant insight as to why some, but not all, women diagnosed with a gynecological cancer experience psychosocial distress.
Study limitations and future directions
The major limitation of this study was related to the small sample size, which limits the generalizability of the findings; this is compounded by the limited range of tumor streams, stages of cancer and prognoses, and the sociodemographic homogeneity of participants. As such, it is possible that studies with a larger sample including women from one gynecological tumor stream at a time may elucidate themes that were not detected in this study. Engaging in larger prospective, longitudinal qualitative studies could broaden understanding of psychosocial factors along the disease trajectory. Furthermore, the reflections regarding the disparity between formal services available to breast cancer patients and gynecological cancer patients warrant further exploration. Particular consideration of the possibility that women with gynecological cancer internalize this variance, and how this sense of alienation could possibly be addressed, may help to reduce distress experienced by this population. For example, psychotherapeutic interventions pertaining to meaning and purpose and existential survivorship could be of benefit to women living with a gynecological cancer.
The current findings demonstrate the merit of listening to women’s voices and the meaning they make of their lives within the context of a gynecological cancer diagnosis. To date, existing interventions and support services have been unable to fully mitigate the experiences of psychosocial distress within this population. The current findings hold promise for redressing this situation. An appreciation of the interplay between women’s reflections on having the “wrong” female cancer, their selective withholding of information, their sense of feeling alone, and existential concerns about dying highlight some of the more difficult aspects of human existence. By directly addressing these factors and concerns, supportive care initiatives may be more efficacious in alleviating the distress women experience.
Footnotes
Acknowledgements
The research team would like to thank each of the participants who shared their experiences.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Narelle Warren was supported by a Fellowship from the National Health and Medical Research Council, Australia.