
Abstract
This study explored the association between parental fear of hypoglycemia, anxiety, and subjective well-being in parents of children and adolescents with type 1 diabetes. A total of 120 mothers and 79 fathers participated. Mothers’ and fathers’ fear of hypoglycemia was significantly associated with anxiety and negative affect as well as with worse glycemic control in child. Paired-samples t-test showed that mothers were more involved in diabetes management and reported more fear and anxiety compared to fathers, but they did not differ in worries about hypoglycemia. The findings suggest screening for fear of hypoglycemia and subjective well-being in all parents regardless of whether their child experienced severe hypoglycemia.
Introduction
Type 1 diabetes mellitus (T1D) is one of the most frequent chronic endocrine disorders in childhood and adolescence. It can seriously impact a young patient’s life as well as their parents, who have an important role in (stressful) daily diabetes management. Guidelines for managing T1D recommend the lowest glycated hemoglobin (HbA1c) that can be sustained without severe hypoglycemia, hyperglycemia, or diabetes ketoacidosis (Ly et al., 2014). Although modern treatment of diabetes with continuous subcutaneous insulin infusion (CSII)—insulin pumps—and help from continuous glucose monitoring systems (CGMS) provides more flexible diabetes management (Bode and Battelino, 2015; Bratina and Battelino, 2010), the problem of acute complications such as hypoglycemia in children with T1D frequently prevents optimal glycemic control (Unger, 2012).
Hypoglycemia is a very common and serious acute complication in glycemic management of child’s T1D which can be potentially life threatening and may lead to permanent long-term complications (Rankins et al., 2005). The risk of hypoglycemia is increased when the treatment regimen is altered (more insulin, less food, more exercise), when there are frequent low blood glucose levels, or awareness of autonomic symptoms is reduced or during sleep. Pediatric hypoglycemia can be very disruptive and significantly affects child’s daily routine (e.g. school-performance, sibling and peer relationships, and activities). Fearfulness of child’s or adolescent’s hypoglycemia during the night is particularly worrisome for parents as it can lead to delayed treatment. Approximately one-third of parents reported regularly monitoring their child’s blood glucose level after their child was asleep (Monaghan et al., 2009). Studies show that frequent blood glucose monitoring and increased responsibility especially in parents of young children are associated with increased fear of hypoglycemia (FOH) in parents (Barnard et al., 2010; Ly et al., 2014; Streisand et al., 2005). Parents of adolescents on the other hand are less involved in diabetes management but may as well experience stress in response to adolescent’s mood fluctuations, developmental issues, and adolescent’s decline in diabetes control and adherence (Braun et al., 2008).
The stress that parents experience in caring for a child and adolescent with T1D puts them at risk of poorer psychological adjustment and subjective well-being (Cousino and Hazen, 2013; Pate et al., 2015). Higher parental worries about hypoglycemia were associated with higher level of trait anxiety (Nyer, 2010). Studies show that parental feelings of anxiety and FOH may impede parents’ ability to understand the importance of diabetes regimen and might lead to a worsening of the child’s glycemic control (Barnard et al., 2010; Butler et al., 2008; Cameron et al., 2007). In both fathers and mothers of children with diabetes, lower parental self-efficacy about diabetes management and greater fears of hypoglycemia were associated with greater disease-related parenting stress (e.g. Klemenčič et al., 2015; Monaghan et al., 2009; Patton et al., 2011). Mothers in particular bear more responsibility for child’s diabetes management, monitoring efforts, and are much more emotionally involved (Jaser et al., 2009; Stallwood, 2005; Sullivan-Bolyai et al., 2006). Although father’s role seems to be important in child’s adjustment to diabetes (Dashiff et al., 2008), there is still little known about fathers’ FOH and their psychological well-being. To our knowledge, recent studies showed inconsistent and limited results regarding maternal and paternal FOH, anxiety, and their subjective well-being (Gonder-Frederick et al., 2006, 2009; Nyer, 2010; Patton et al., 2007). The first aim of this study was to analyze the association between parental FOH and anxiety, subjective well-being, and child’s diabetes-related characteristics, and the second aim was to explore whether mothers experience more FOH, more anxiety, and lower subjective well-being than fathers. It was hypothesized that higher level of FOH in parents would be associated with higher glycated hemoglobin, lower age, and longer duration of T1D in the child as well as with higher anxiety and lower subjective well-being in parents. Mothers would engage frequent monitoring and involvement in child’s diabetes management and would have higher FOH, anxiety, and lower subjective well-being compared to fathers.
Methods
Participants and study design
The cross-sectional study started in 2014 at the Department of Endocrinology, Diabetes and Metabolic Diseases at University Children’s Hospital (UCH) Ljubljana. UCH Ljubljana is the only center for childhood diabetes in Slovenia. From June to September 2014, the outpatient clinic for diabetes treated 201 children and adolescents from 7 to 17 years old with T1D duration ⩾1 year. Mothers and fathers of these 201 children and adolescents with T1D were invited to participate in the cross-sectional study at their regular diabetes outpatient clinic visit. The identical questionnaires for mothers and fathers with information sheet were distributed to these parents and the value of child’s HbA1c was obtained at the same time. Returned surveys were considered as informed consent. The study protocol was approved by the National Medical Ethics Committee (Approval No. 122/04/10) and registered at ClinicalTrials.gov (No. NCT02010528).
Measurements
The Hypoglycemia Fear Survey–Parent version (HFS-P) was used to assess the degree of fear experienced with respect to hypoglycemia in parents of children with T1D (Clarke et al., 1998). The questionnaire consists of 26 items and is resulting in a total score and subscale scores obtained by summing the items for, respectively, behavior subscale (range, 10–50), the worry subscale (range, 15–75), and HFS-P total (range, 26–130). Behavior subscale is related to parent’s management behaviors preventing hypoglycemia in his or her child. Worry subscale measures the parent’s anxiety that his or her child might be experiencing hypoglycemia. Higher scores indicate greater FOH in parents. Despite a good internal consistency (Clarke et al., 1998; Gonder-Frederick et al., 2006; Haugstvedt et al., 2010), the instrument still lacks a manual for interpreting the scores and cutoff points to indicate concerning levels of fear (Haugstvedt et al., 2010). The measure was translated into Slovenian language; the back-translated version was approved by the author. Cronbach’s alpha coefficient of reliability for the Slovenian version for the HFS-P-Total score is .89, for the behavior subscale is .78, and for the worry subscale is .90. These results are comparable with the Cronbach’s alpha values reported by several studies for the total scale ranging from .84 to .89, the behavior subscale from .69 to .89, and for the worry subscale from .88 to .91 (Clarke et al., 1998; Gonder-Frederick et al., 2006; Haugstvedt et al., 2010). In this study, HFS-P-Total score was significantly associated with the State Trait Anxiety Inventory (STAI) that additionally confirmed good construct validity (r = .33, p = .000).
STAI was used to determine the anxiety in parents of children and adolescents with T1D (Spielberger et al., 1983 in Lamovec, 1988). The STAI differentiates state and trait anxiety. For the purpose of the study, only trait anxiety was used. Participants evaluate on a 20-item scale as to how they usually feel (1—never, 4—often). A higher score indicates a greater level of anxiety. Cronbach’s alpha coefficient of the STAI trait scale in the study was .90.
Subjective well-being was measured by the Positive and Negative Affect Schedule (PANAS) (Watson et al., 1988) and the Satisfaction with Life Scale (SWLS) (Pavot and Diener, 1993 in Avsec, 2000). PANAS is a 20-item measure to assess dimensions of positive affect (PA) and negative affect (NA). Participants rate on a scale from 1 to 5 on how often they experience a particular emotion in general. Internal consistencies for the NA scale (αs from .84 to .87) and for the PA scale (αs from .90 to .96) are good to excellent (Watson et al., 1988); in the study sample, for the NA scale α = .87 and for the PA scale α = .84. SWLS is a 5-item instrument designed to assess respondent’s cognitive evaluation of overall life. It has adequate criterion validity, good convergent and discriminant validity, and good reliability, demonstrated in terms of high internal consistency with a value of α = .87 and stability overtime with a test–retest coefficient of α = .82 (Pavot and Diener, 1993), in the study sample α = .88.
Sociodemographic data such as parent’s education level, employment status, and marital status were collected. Additional information related to child’s T1D such as the most recent HbA1c value, current type of insulin administration, illness duration, and experience of severe hypoglycemic episodes were collected from patients’ files in UCH. Next, parents provided additional information about their own perceptions of their involvement in the child’s daily diabetes management, frequency of blood glucose monitoring, general satisfaction with glycemic control, and an evaluation of self-perceived knowledge about the child’s diabetes.
Statistical analyses
Frequencies, means, standard deviation (SD), range, and percentage distribution were calculated to describe the study sample. Bivariate correlations (for mothers and fathers separately) were calculated to examine associations between measured variables. Paired-samples t-tests were carried out for comparisons between mother–father dyads. The level of significance was set at .05. Statistical analyses were performed using the statistical software package SPSS 21.0 (IBM Corp., 2012).
Results
Demographics
Questionnaires from 125 (62.2%) families (199 parents, 120 mothers, and 79 fathers) were returned. In 74 cases both parents participated in the study, in 5 cases only the father, and in 46 only the mother. Mothers’ mean age was 41.7 years (SD = 5.7), ranging from 31 to 58 years, and fathers’ mean age was 44.9 years (SD = 6.7), ranging from 33 to 65 years.
Table 1 presents descriptive statistics for parents and their children with T1D (59 girls and 66 boys) with duration of diabetes from 1 to 14 years. Most children were on CSII therapy and 8.8 percent of these used CGMS as well. The sample’s mean HbA1c was 7.6 percent (SD = .9) (59.6 mmol/mol, SD = 9.8), ranging from 5.5 to 9.4 percent (36.6–79.2 mmol/mol). The normal HbA1c range is 4.5–6.1 percent (25.7–43.2 mmol/mol). The recommended value for children and adolescents with T1D is lower than 7.5 percent (58.5 mmol/mol) (Rewers et al., 2014). For 69 children, neither the mother nor the father responded to the questionnaire. Children of these non-responding parents had significantly higher mean HbA1c (8.3% vs 7.6%) (67.2 vs 59.6 mmol/mol) compared with the children of parents who did respond. The children of parents who participated in the study had a significantly lower current HbA1c compared to non-respondents (M-W = 6.12, p = .00) (Dovc et al., 2014).
Descriptive statistics of children (7–17 years old) with T1D and their parents.

n: numerous; M: mean; SD: standard deviation; T1D: type 1 diabetes mellitus; CGMS: continuous glucose monitoring systems.
FOH
The Pearson correlation coefficients between parental FOH and other variables are presented in Table 2. Maternal FOH was associated with anxiety and NA. Mothers of children with higher HbA1c were more worried about hypoglycemia. Longer duration of T1D and lower satisfaction with child’s glycemic control were as well associated with higher total FOH in mothers. More worries about hypoglycemia in mothers were associated with frequent monitoring of the child’s blood glucose at night (ρ = .22, p = .01). Additionally, mothers whose children experienced at least one severe hypoglycemic event reported significantly more preventive behaviors to avoid hypoglycemia (r = .25, p = .03). Fathers of younger children used significantly more preventive behaviors to avoid hypoglycemia, and fathers of children with higher HbA1c were more worried about hypoglycemia. Additionally, fathers who were involved in daily diabetes management used significantly less preventive behaviors to avoid hypoglycemia (r = −.24, p = .04), whereas there was no association in mothers (r = −.06, p = .64).
Correlations for fathers’ and mothers’ ratings of measured variables.
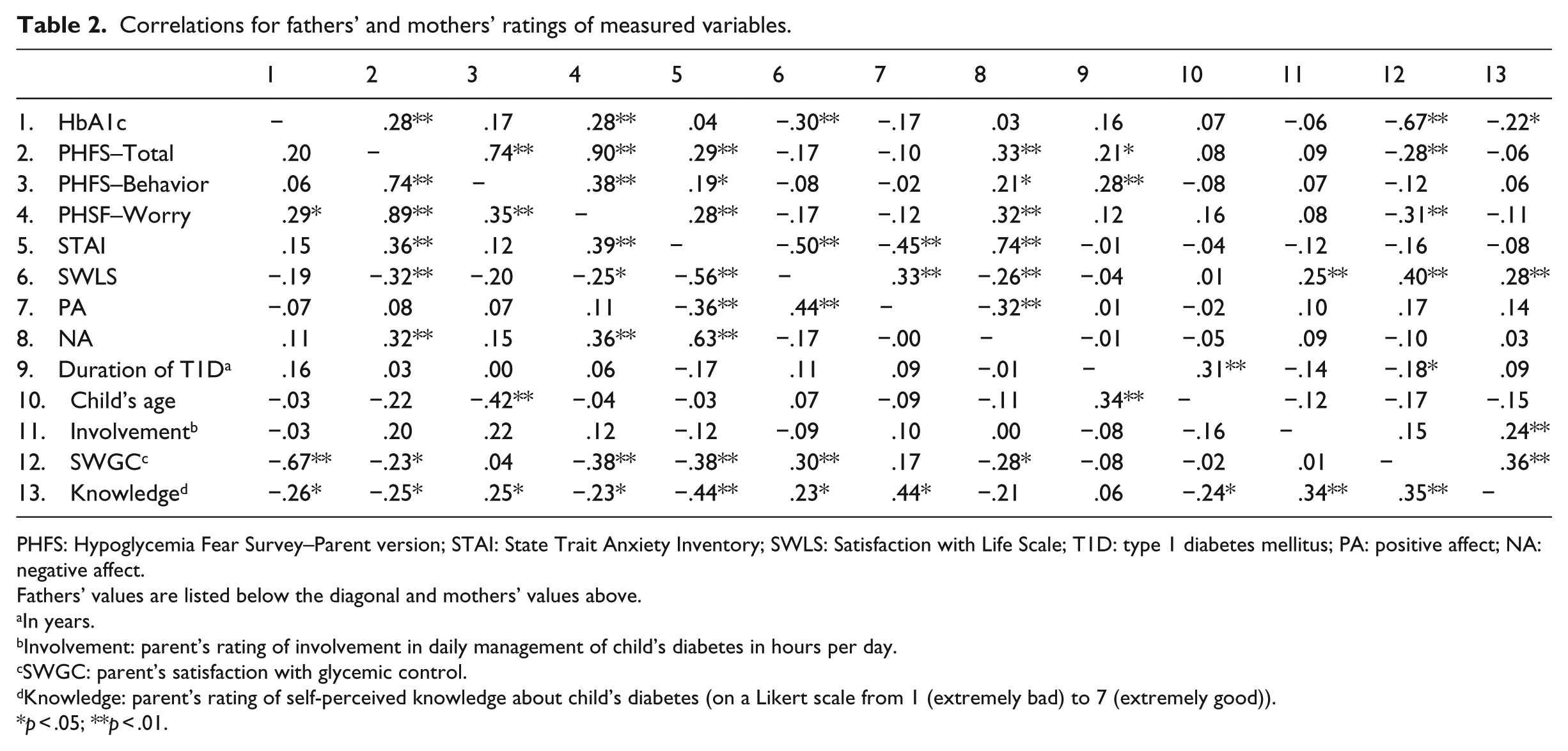
PHFS: Hypoglycemia Fear Survey–Parent version; STAI: State Trait Anxiety Inventory; SWLS: Satisfaction with Life Scale; T1D: type 1 diabetes mellitus; PA: positive affect; NA: negative affect.
Fathers’ values are listed below the diagonal and mothers’ values above.
In years.
Involvement: parent’s rating of involvement in daily management of child’s diabetes in hours per day.
SWGC: parent’s satisfaction with glycemic control.
Knowledge: parent’s rating of self-perceived knowledge about child’s diabetes (on a Likert scale from 1 (extremely bad) to 7 (extremely good)).
p < .05; **p < .01.
Descriptive statistics and differences between mothers and fathers for HFS-P and its subscales are presented in Table 3. Paired-samples t-tests showed that mothers and fathers differed in FOH total score as well as in behavior subscale; mothers were experiencing significantly higher fear and noted more preventive behaviors compared to fathers. Additionally, mothers were more engaged in daily diabetes management (3.1 vs 1.1, t(72) = 4.15, p = .00) and perceived their knowledge about child’s diabetes better compared to fathers (5.1 vs 4.5, t(74) = 3.56, p = .00).
Comparison of scale scores for mothers and fathers of children with type 1 diabetes.
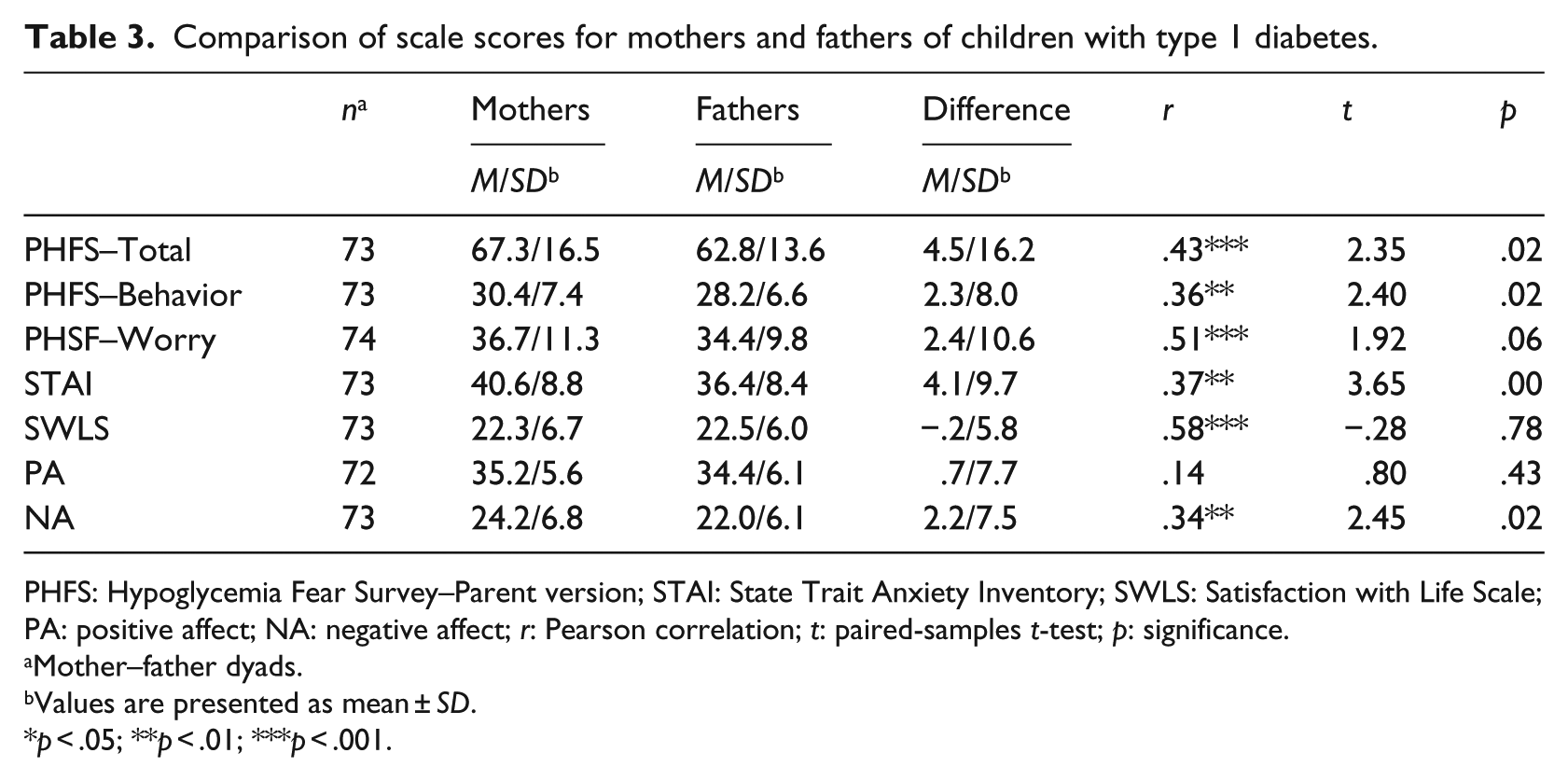
PHFS: Hypoglycemia Fear Survey–Parent version; STAI: State Trait Anxiety Inventory; SWLS: Satisfaction with Life Scale; PA: positive affect; NA: negative affect; r: Pearson correlation; t: paired-samples t-test; p: significance.
Mother–father dyads.
Values are presented as mean ± SD.
p < .05; **p < .01; ***p < .001.
Trait anxiety
Paternal anxiety was associated with lower self-perceived knowledge about child’s diabetes and lower general satisfaction with child’s glycemic control. In both fathers and mothers, more anxiety symptoms were associated with worse subjective well-being, in fathers only the anxiety significantly correlated with lower satisfaction with glycemic control and lower self-perceived knowledge about child’s T1D. Paired-samples t-test showed that mothers reported higher anxiety compared to fathers (t(72) = 3.65, p = .00).
Subjective well-being
Moderate significant correlation was found between paternal satisfaction with life and FOH. Fathers who were more satisfied with their life reported lower fear and were less worried about hypoglycemia. On the other hand, mothers who were more satisfied with their life were more involved in daily diabetes management and had children with lower HbA1c. Both fathers and mothers who were more satisfied with life, perceived their knowledge about child’s diabetes higher and were more satisfied with child’s glycemic control. Fathers who reported more positive emotions perceived their knowledge about child’s diabetes higher and those who reported more negative emotions were less satisfied with child’s glycemic control. Paired-samples t-test showed that mothers reported significantly more negative emotions compared to fathers (t(72) = 2.45, p = .02), but there were no differences in positive emotions (t(71) = .80, p = .43) as well as in satisfaction with life (t(72) = −.25, p = .78).
Discussion
The aim of this study was to analyze the relationship between the child’s diabetes-related characteristics as perceived by parents, parental FOH, anxiety, and subjective well-being and to explore whether there are differences between mothers and fathers of children with T1D in measured variables.
The results of this study showed that higher parental FOH was associated with higher HbA1c levels. The data from studies which explored the association between child’s higher HbA1c values and higher FOH in parents are inconsistent. Some studies have not found associations (Cameron et al., 2007; Gonder-Frederick et al., 2006; Jaser et al., 2009), whereas others have found important associations between mother’s FOH and higher HbA1c (Clarke et al., 1998; Haugstvedt et al., 2010). Our study showed that mothers and fathers of children with higher HbA1c values were more worried about the child’s hypoglycemia; in addition, mothers also reported higher total score in FOH. This suggests that higher levels of fear in parents might lead to deliberate maintenance of higher blood glucose levels and/or that concerns about hypoglycemia might be higher than concerns about long-term diabetes complications.
FOH may have potential risks and effects on diabetes management. In this study, mothers were more engaged in daily diabetes management than fathers. Mothers who reported history of the child’s severe hypoglycemia episode in the past used more preventive behavior to avoid hypoglycemia. This suggests that parents with experience of their child suffering from severe hypoglycemia would need additional support and assistance in dealing with this life-threatening and traumatic event. The association between parental FOH and experience of a severe hypoglycemia episode was found only in mothers, which is in contrast with previous research (Nordfeldt and Ludvigsson, 2005; Patton et al., 2008). Results from this study might suggest that the experience of severe hypoglycemia could have a stronger impact on maternal engagement and responsibility for child’s diabetes management. These results are consistent with other studies (Mitchell et al., 2009; Patton et al., 2008; Sullivan-Bolyai et al., 2003, 2006). Furthermore, maternal worries about hypoglycemia were associated with more frequent night-time blood glucose measurements. Mothers had significantly higher FOH, used more preventive behavior to avoid hypoglycemia, estimated their self-perceived knowledge about child’s diabetes better, and were more involved in daily diabetes management than fathers. This is consistent with other studies that also show lower paternal diabetes monitoring efforts and lower responsibility and involvement (Jaser et al., 2014). Furthermore, fathers who worried about hypoglycemia were less satisfied with their life, reported more negative emotions, and estimated their self-perceived knowledge about the child’s diabetes poorly. This suggests that fathers as well experience some type of stress, but on the other hand underestimate the importance of diabetes management tasks and thus their own important role in the management of child’s diabetes (Dashiff et al., 2008; Sullivan-Bolyai et al., 2006). Interestingly, when analyzing the parental daily involvement in diabetes management, involved fathers used less preventive behaviors to avoid hypoglycemia. This suggests that father’s involvement in diabetes management could be associated with better regulation of the FOH. Mothers and fathers may react differently to their roles in diabetes management and perceptions of their involvement may be differently associated with the child’s diabetes (Hansen et al., 2012; Swallow et al., 2012).
Parenting a child with T1D involves the complex process of assuring the child’s safety in living with a chronic illness as well as helping the child to achieve age-appropriate independence in diabetes self-control (Bratina et al., 2015).
Findings of this research study should be understood through several limitations. The sample’s mean HbA1c was significantly lower than that of the eligible population of children and adolescents with T1D. The majority of parents were employed and married or in relationships. Also we did not gather parental assessment of their satisfaction with marital or couple’s relationship and parenting stress which are likely to impact parental subjective well-being. Further research, especially longitudinal design methods and interventions, is needed to help assess appropriate and inappropriate behaviors, worries, and fear regulation in parents regarding child’s hypoglycemia and diabetes management.
Conclusion
Results from this study including both parents showed that mothers reported higher FOH and were more engaged in diabetes management compared to fathers. Our study confirmed that mothers who reported more preventive behavior had children with higher HbA1c values. Special attention should be given to all parents of children with diabetes, regardless of whether they have experienced severe hypoglycemia. The higher parental FOH, the worse child’s glycemic control, and the lower parental subjective well-being emphasize the importance of screening for FOH in parents. Annual psychological screening that is being performed in Slovenia in the last years can help to recognize families at risk in the early phase (Klemenčič et al., 2015). Continuous education and psychological support for parents with special attention to support father’s involvement in diabetes management could improve family functioning in type 1 diabetes (Klemenčič et al., 2015). Healthcare professionals must be able to recognize and assess symptoms of FOH in parents and children and to design interventions for fear and stress reduction. Psychological interventions that consider the difference in parents’ approaches in relation to their child’s diabetes management could help to recognize potential risk patterns of FOH which could have an important impact on a child’s glycemic control as well as parental well-being.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was, in part, financed by EU-CDEC project number 2013-1-GB2-LEO-05-10755 and Slovenian Research Agency Grants J3-9663, J3-2412, J3-4116, and P3-0343. This study was supported, in part, by the Department of Endocrinology Diabetes and Metabolic Diseases at University Children’s Hospital Ljubljana.