
Abstract
This study tested the hypotheses of irritable bowel syndrome showing (1) comorbidity with chemical and sound intolerance, other types of functionally somatic syndromes, and psychiatric disorders and (2) stronger than normal affective reactions to and behavioral disruptions from odorous/pungent chemicals and sounds in daily life. These hypotheses were tested by means of data from a large-scale population-based questionnaire study. The results showed comorbidity in irritable bowel syndrome with chemical and sound intolerance, fibromyalgia, migraine, post-traumatic stress disorder, generalized anxiety disorder, panic syndrome, and depression as well as strong reactions/disruptions from odorous/pungent chemicals and sounds in irritable bowel syndrome.
Keywords
Introduction
Irritable bowel syndrome (IBS) is a debilitating condition with considerable impact on quality of life (Mönnikes, 2011) and associated with high societal costs (Hillilä et al., 2010). A large-scale meta-analysis shows a world-wide prevalence of 9.4 percent and a 40 percent increased risk for women compared to men (Rome II criteria; Lovell and Ford, 2012a, 2012b). Based on the Rome III classification of functional gastrointestinal disorders, IBS is a functional bowel disorder in which abdominal pain or discomfort is associated with defecation or a change in bowel habit and with features of disordered defecation (Longstreth et al., 2006).
The central nervous system and the gut communicate through the brain–gut axis by means of sympathetic and parasympathetic pathways and by modulation of the enteric nervous system and hypothalamic–pituitary–adrenal axis. It has been suggested that IBS is a disorder of dysregulation of the brain–gut axis, involving abnormal function in the enteric, autonomic, and/or central nervous systems. Thus, the dysregulation can be referred to disturbed central processing of signals from the periphery as well as to the autonomic nervous system and the hypothalamic–pituitary–adrenal axis (Öhman and Simrén, 2007). Anxiety and depression may influence autonomic function in IBS (Jarrett et al., 2003), and it is well documented that psychiatric conditions of distress are associated with IBS (Chang, 2011; Hausteiner-Wiehle and Henningsen, 2014; Whitehead et al., 2003).
IBS is considered a functional somatic syndrome (FSS; Barsky and Borus, 1999), commonly defined as physical illnesses without an organic disease explanation and devoid of demonstrable structural lesion or established biochemical change (Manu, 1998). As in IBS, associations with psychiatric conditions are commonly found in other types of FSSs, such as fibromyalgia (Bernik et al., 2013) and migraine (Buse et al., 2013). As would be expected from this, high comorbidity in IBS is commonly found with these other types of FSS (Whitehead et al., 2002, 2007). Due to this comorbidity, it has been suggested, but also debated, that there may be only one FSS with underlying mechanisms shared by the conditions (Wessely and White, 2004).
Whereas the comorbidity in IBS with certain types of FSS is well documented, little is known about its comorbidity with other types of FSS. This includes environmental intolerances, in which the afflicted individual attributes several, multisystem symptoms to a specific environmental exposure that does not bother the majority of people. The two most common types of intolerances are those to odorous/pungent everyday chemicals (e.g. perfumes) and sounds (e.g. crinkling papers). In these conditions, there is no clear dose–response relation, and the exposure levels that evoke symptoms are typically far below those known to be hazardous and do not evoke symptoms in most people (Henningsen and Priebe, 2003). Common symptoms are airway, mucosal, and general symptom (e.g. fatigue) in chemical intolerance (Andersson et al., 2009b) and attentional, emotional, and general symptoms in sound intolerance (Andersson et al., 2002). The comorbidity between these two types of environmental intolerance is considerable (Nordin et al., 2013a; Palmquist et al., 2014), and chemical intolerance has shown comorbidity also with fibromyalgia (Jason et al., 2000).
The most commonly used clinical diagnosis for chemical intolerance is multiple chemical sensitivity (Multiple chemical sensitivity: A 1999 consensus, 1999), whereas a common clinical term for sound intolerance is sound hypersensitivity (Andersson et al., 2002). Since there are no generally agreed on objective methods for assessment of intolerance to chemicals and sounds, it is common to assess them with a single question as a self-report. Whereas 0.5–6.3 percent of the general population fulfill clinical criteria for chemical intolerance (Caress and Steinemann, 2003; Johansson et al., 2005; Kreutzer et al., 1999; Park and Knudson, 2007), 11–16 percent have been found to have this intolerance based on self-reports (Caress and Steinemann, 2003; Kreutzer et al., 1999; Nordin et al., 2012). The prevalence rate for self-reported sound intolerance is 8–15 percent (Andersson et al., 2002; Fabijanska et al., 1999; Nordin et al., 2012).
Neural sensitization is of particular relevance in FSS. Rather than habituating to external or internal stimuli, the afflicted person may show sensitization, thus increased rather than decreased neural activity in response to repeated stimulation. Sensitization may be present at both a cellular and psychological (sustained attention and cognitive bias) level (Eriksen and Ursin, 2004). In central sensitization, also referred to as kindling, sensitization takes place in limbic structures, and there is growing support for this mechanism underlying IBS, fibromyalgia, chronic fatigue syndrome, and migraine (Dodick and Silberstein, 2006; Eriksen and Ursin, 2004; Yunus, 2007). Repeated exposure can, due to high arousal and negative associations with the exposure, result in automated reactions in neural structures. Central sensitization can be considered a model for cross-sensitization in which a person becomes sensitized to exposures different from those to which the person is already sensitized. It has also been suggested as an explanatory concept for comorbid psychiatric disorders such as anxiety, depression, and panic disorder in somatization patients (Ursin and Eriksen, 2001). Yunus (2007) has coined the term central sensitization syndrome to which he includes a large number of FSSs. Thus, according to this reasoning, there is an overlap of similar syndromes without structural pathology and are bound by the common mechanism of central sensitization. Brain-imaging studies of IBS (Andresen et al., 2005) and fibromyalgia (Jensen et al., 2009) suggest that sensitization is due to a dysfunctional inhibition in the anterior cingulate cortex, resulting in increased activity in insula when exposed to the stimulus to which the afflicted individual is sensitive.
Central sensitization is likely to be a mechanism underlying chemical intolerance (e.g. multiple chemical sensitivity) and possibly also sound intolerance. Bell et al. (1992) early suggested an olfactory-limbic model for sensitization in multiple chemical sensitivity, and Sorg (1999) has provided further foundation for neural sensitization in multiple chemical sensitivity. However, empirical support for central sensitization in chemical intolerance in humans is in fact quite limited, but does exist (Andersson et al., 2009a; Bell, 1996; Tran et al., 2013). Regarding sound intolerance, it is of interest to note that IBS patients have shown dysfunctional inhibition in the anterior cingulate cortex in response to sound, resulting in increased activity in insula (Andresen et al., 2005). Furthermore, indirect support for central sensitization in environmental intolerance is provided by studies showing comorbidity in both chemical and sound intolerance with psychiatric disorders such as anxiety, depression, and panic disorder (Black et al., 2000; Bornschein et al., 2001; Jüris et al., 2013).
To conclude, the dysregulation of the brain–gut axis in IBS is likely to be enhanced by psychiatric conditions such as anxiety and depression and may possibly be explained by central sensitization. Sensitization of this kind has been proposed as a model for cross-sensitization, which may explain the high comorbidity in IBS with other types of FSSs as well as the comorbidity between chemical intolerance, sound intolerance, and psychiatric conditions.
The aim of this study was to better understand environmental intolerance in IBS by determining the comorbidity in IBS with intolerance to odorous/pungent chemicals and sounds as well as by quantifying affective reactions to and behavioral disruptions by odorous/pungent chemicals and sounds in daily life. The comorbidity was studied with respect to both physician-diagnosed and self-reported environmental intolerance. The two conditions are not mutually exclusive and can instead be considered to differ in strictness of criteria; physician-diagnosed environmental intolerance being stricter. Of relevance for central sensitization, comorbidity was also investigated in IBS with diagnoses of other FSSs and psychiatric disorders. It was hypothesized that (1) IBS would show comorbidity with chemical and sound intolerance, other types of FSSs, and psychiatric disorders and (2) affective reactions to and behavioral disruptions from odorous/pungent chemicals and sounds in daily life would be stronger than normal in IBS. These hypotheses were tested by means of data from a large-scale population-based study, the Västerbotten Environmental Health Study.
Methods
Study population and sample
The Västerbotten Environmental Health Study is an embracing name for different investigations regarding environmental health matters in Sweden. Data were derived from a random sample of 8520 individuals aged 18–79 years in the county of Västerbotten in Northern Sweden. The sample was stratified for age and sex according to the following age strata: 18–29, 30–39, 40–49, 50–59, 60–69, and 70–79 years. The questionnaire was sent to the sample, of which 40 percent (n = 3406) agreed to participate. The sample’s age and sex distribution is described in Palmquist et al. (2014).
Of the 3406 participants, 80 reported having received a diagnosis of IBS by a physician, constituting an IBS group. The remaining 3326 participants constituted a group without IBS for comparison, here referred to as referents. The two groups are described in Table 1 with respect to demographics, perceived general health status, and levels of distress and somatization. Compared to the referent group, the IBS group consisted of a significantly larger proportion of women and had poorer perceived general health and higher levels of anxiety, depression (Hospital Anxiety and Depression Scale; Sullivan et al., 1993; Zigmond and Snaith, 1983), stress (10-item Perceived Stress Scale; Cohen and Williamson, 1988; Nordin and Nordin, 2013), burnout (Shirom-Melamed Burnout Questionnaire; Grossi et al., 2003; Melamed et al., 1992), and somatization (Patient Health Questionnaire 15-Item Somatic Symptom Severity Scale; Kroenke et al., 2002; Nordin et al., 2013c). The latter was calculated as percentage of possible total score to enable direct comparison between women and men due to different max scores. The two groups did not differ significantly in age or education.
Participant characteristics and p values from group comparisons with t-test and χ2 analysis.

HADS: Hospital Anxiety and Depression Scale; PSS-10: 10-Item Perceived Stress Scale; SMBQ: Shirom-Melamed Burnout Questionnaire; PHQ-15: Patient Health Questionnaire 15-Item Somatic Symptom Severity Scale (% of total score); SD: standard deviation.
Questions and questionnaire instruments
Physician-based diagnoses of IBS, multiple chemical sensitivity, sound hypersensitivity, fibromyalgia, migraine, generalized anxiety disorder, depression, panic syndrome, and post-traumatic stress disorder were assessed with the question “Have you been diagnosed with this disease by a physician?” Self-reported intolerance to odorous/pungent chemicals was assessed with the question “Are you getting symptoms from odorous/pungent chemicals (not limited to certain buildings), such as perfumes and cleaning agents, in doses that you were not getting symptoms from before or that you believe most other people are not getting symptoms from?” Self-reported intolerance to sounds was assessed with the question “Do you have a hard time tolerating everyday sounds that you believe most other people can tolerate?”
The Chemical Sensitivity Scale for Sensory Hyperreactivity (CSS-SHR; Nordin et al., 2004) and the 11-item Noise Sensitivity Scale (NSS-11; Nordin et al., 2013b) were used to quantify affective reactions to and behavioral disruptions by environmental odorous/pungent chemicals and sounds, respectively. Each scale consists of 11 statements for the individual to respond to on a Likert scale, and the statements are analogous between scales. For example, the CSS-SHR statement “At movies, other persons’ perfume and aftershave disturb me” corresponds to the NSS-11 statement “At movies, whispering and crinkling candy wrappers disturb me.” Each of the two sensitivity scales range in score from 0 to 54, with high score indicating high sensitivity. The CSS-SHR and NSS-11 have good reliability, validity, and normative data (Nordin et al., 2004, 2013b). In this study, Cronbach’s α was 0.81 for the CSS-SHR and 0.77 for the NSS-11.
Procedure
The questionnaire was sent to the participants with the instruction to return it via mail with prepaid postage. Those who did not respond to the first invitation received up to two reminders. For the data on the CSS-SHR and NSS-11, missing values were estimated with multiple imputations using fully conditional Markov chain Monte Carlo methods with 10 maximum iterations by means of which five imputed datasets were created. The estimate values were obtained by pooling the five datasets. The percentage of the data being imputed was 5.46 percent for the CSS-SHR and 5.31 percent for the NSS-11. All participants responded to the questionnaire during the period March–April 2010, before the onset of the pollen season in Västerbotten. The study was conducted in accordance with the Helsinki Declaration and approved by the Umeå Regional Ethics Board (Dnr 09-171M). All participants gave their informed consent to participate.
Statistical analysis
The IBS and referent groups were compared on the background variables (Table 1) with independent t-tests and chi-square analyses. Based on binary logistic regression analysis, comorbidity in IBS with each of the nine other physician-diagnosed conditions was expressed as both a crude (unadjusted) odds ratio (OR) and an OR adjusted for sex, with the reference group as referents. Two-factorial analyses of variance (ANOVAs; one-sided due to stated hypotheses; sex as a controlled factor) with general linear model (GLM) procedure were conducted to compare the IBS and referent groups on scores on the CSS-SHR and NSS-11. Cohen’s d (Cohen, 1988) was used as effect-size measure. The α-level was set at 0.05. The Statistical Package for the Social Sciences (IBM SPSS Statistics for Windows, Version 22.0; IBM Corp., Armonk, NY, USA) was used for the data analyses.
Results
Percentage of the participants with IBS who also had a condition of environmental intolerance, other FSSs, and psychiatric disorders is shown in Figure 1. The higher prevalence rates for self-reported compared to physician-diagnosed environmental intolerance may be explained by self-reported intolerance being a less strict criterion than physician-diagnosed intolerance. The figure also gives ORs for comorbidity in IBS with the 11 conditions when unadjusted (crude) and adjusted for sex. All conditions had an OR that was significantly higher than unity, irrespective of adjusting or not for sex. The ORs adjusted for sex were 2.12–2.87 for environmental intolerances, 3.10–6.28 for other FSSs, and 3.71–10.12 for psychiatric disorders. These results show that although only a minority of the participants with IBS also have a condition of environmental intolerance, other FSSs or psychiatric disorders, there was a 2- to 10-fold increased risk in the IBS group of having these conditions.
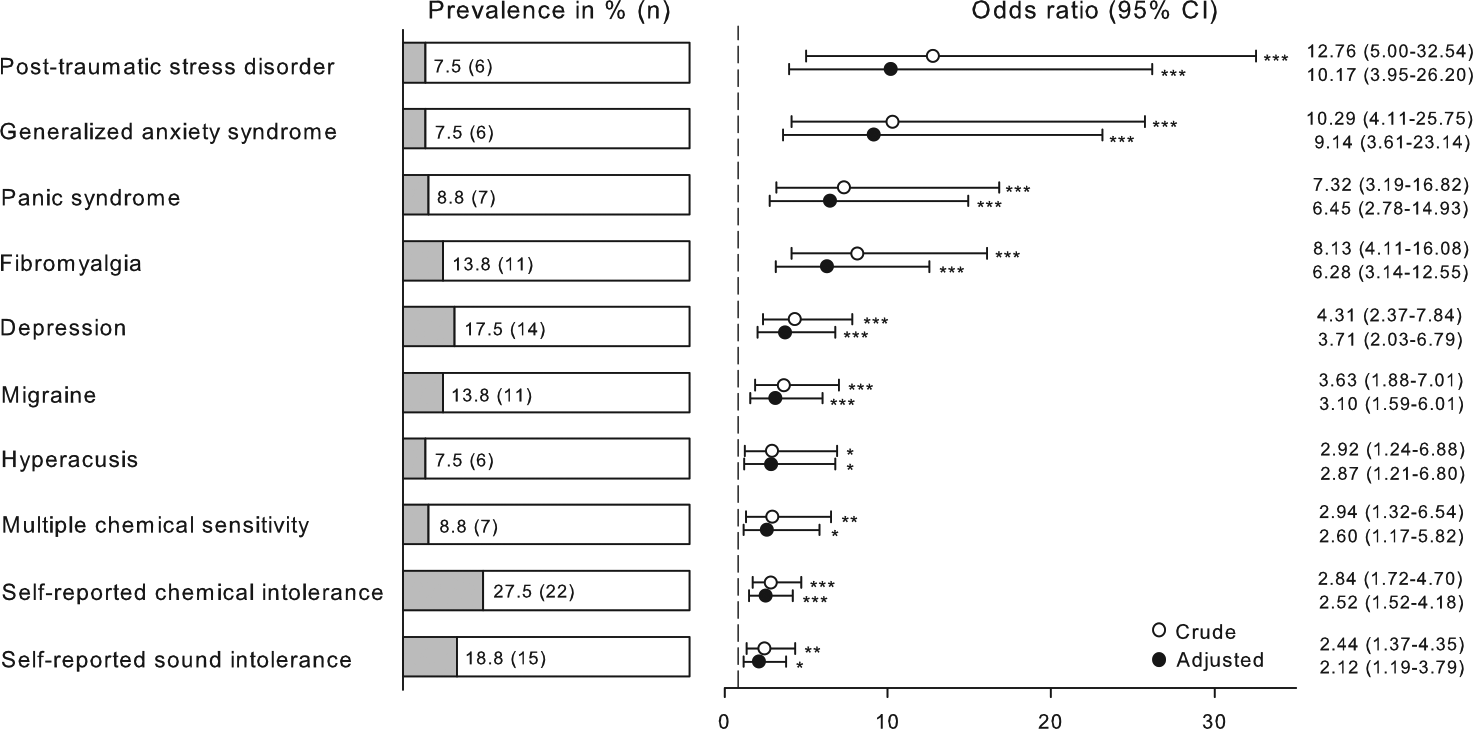
Prevalence of environmental intolerances, functional somatic syndromes and psychiatric disorders among participants with irritable bowel syndrome. Odds ratios (ORs), confidence intervals (CIs) and p-values for comorbidity with these conditions are given when unadjusted (crude) and adjusted for sex. Referents are used as a reference group. The vertical dashed line represents an OR of unity.
Mean (standard deviation (SD)) score on the CSS-SHR was 32.4 (9.93) in the IBS group and 29.7 (9.23) in the referents. Corresponding scores in the NSS-11 were 30.2 (9.75) and 27.2 (8.07), respectively. The scores were significantly higher in the IBS group on both the CSS-SHR (F = 3.92, p = 0.048, d = 0.217) and NSS-11 (F = 7.56, p = 0.006, d = 0.304) when controlled for sex. Thus, the IBS group, compared to the referents, showed significantly stronger affective reactions to and behavioral disruptions from odorous/pungent chemicals and sounds, respectively.
Discussion
The purpose of this study was to test the hypotheses of (1) IBS showing comorbidity with environmental intolerance, other FSSs, and psychiatric disorders and (2) high level of affect/disruption by chemicals and sounds in daily life. Both hypotheses were supported by the data. Irrespective of whether the criteria were physician-diagnosed or self-reported chemical or sound intolerance, there was an increased risk of having such an intolerance in IBS. Further support for IBS being associated with environmental intolerance is provided by the data showing stronger affective reactions to and behavioral disruptions by both odorous/pungent chemicals and sounds. As for the ORs for environmental intolerance, the effect sizes for these measures of chemical (d = 0.22) and sound (d = 0.30) intolerance can be considered as small (Cohen, 1988).
As expected, the comorbidity in IBS with other types of FSSs and psychiatric disorders was considerable. Among the FSSs, the highest risk was found for fibromyalgia, whereas post-traumatic stress syndrome showed highest risk among the psychiatric disorders. The comorbidity found in this study is in accordance with results of prior studies in IBS regarding both FSSs (Whitehead et al., 2002, 2007) and psychiatric disorders (Chang, 2011; Hausteiner-Wiehle and Henningsen, 2014; Surdea-Blaga et al., 2012; Tosic-Golubovic et al., 2005; Whitehead et al., 2003). A validation of the comorbidities with psychiatric disorders is the high levels of anxiety, depression, stress, burnout, and somatization in the sample with IBS, assessed with validated questionnaire instruments (Table 1). The participants with IBS were also, compared to the referents, distributed toward poorer perceived general health status (Table 1).
The results showing comorbidity in IBS with fibromyalgia, migraine, generalized anxiety disorder, depression, panic syndrome, and post-traumatic stress disorder provide indirect support for central sensitization in IBS. The psychiatric conditions are likely to underlie sensitization in IBS, and IBS has together with the other types of FSSs been suggested to be included in the central sensitization syndrome (Yunus, 2007).
Although there is still limited empirical support (Andersson et al., 2009a; Bell, 1996; Tran et al., 2013), there is solid theoretical ground for central sensitization being an explanatory model also for chemical intolerance (Bell et al., 1992; Sorg, 1999; Ursin and Eriksen, 2001). Furthermore, comorbidity in chemical and sound intolerance with psychiatric disorders is documented (Black et al., 2000; Bornschein et al., 2001; Jüris et al., 2013) and fibromyalgia in chemical intolerance (Jason et al., 2000). The present results of comorbidity in IBS with environmental intolerance provide indirect support for central sensitization in chemical and sound intolerance, and findings from brain-imaging studies provide further support. It was early proposed that the anterior cingulate cortex serves as a gaiting function in modulating conditioned fear (Hamner et al., 1999). In addition to fear, the anterior cingulate cortex plays a role in regulating attention, suffering, avoidance, and sensory inhibition and inhibition of structures such as the amygdala, insula, hippocampus, and orbitofrontal cortex (for review, see Andresen et al., 2005; Hamner et al., 1999). Dysfunctional inhibition in the anterior cingulate cortex, resulting in increased activity in insula, has been reported for IBS (Andresen et al., 2005) and fibromyalgia (Jensen et al., 2009). Interestingly, preliminary analyses suggest inhibition in the anterior cingulate cortex, resulting in increased activity in insula, amygdala, and orbitofrontal cortex in chemical intolerance when exposed to odorous/pungent stimuli (Nordin et al., 2012). The high comorbidity between different types of FSSs has been explained by kindling of limbic structures causing hypersensitivity to a variety of stimuli through cross-sensitization (Eriksen and Ursin, 2004). Consequently, an interpretation of the comorbidities found in this study is that cross-sensitization may have occurred from IBS (or any other comorbid type of FSS) to environmental intolerance or in the opposite direction.
As a theoretical framework, and with support from the present data, the dysregulation of the brain–gut axis in IBS may be referred to central sensitization. The sensitization may be enhanced by psychiatric conditions (Ursin and Eriksen, 2001) and due to cross-sensitization (Yunus, 2007) explain the comorbidity with chemical and sound intolerance. The sympathetic and parasympathetic pathways that constitute the brain–gut axis are known to be regulated by the anterior cingulate cortex (Critchley et al., 2003). Although outside the empirical scope of this study, dysfunctional inhibition of this cortex in IBS (Andresen et al., 2005) may, in addition to sympathetic and parasympathetic dysregulation, cause decreased inhibition of activity in the amygdala, insula, hippocampus, and orbitofrontal cortex and as a consequence result in fear and attention to internal and external stimuli (Andresen et al., 2005; Hamner et al., 1999).
Regarding therapy for IBS, Deary et al. (2007) have reviewed cognitive behavioral models that are tailored for specific mechanisms underlying FSSs, including IBS. The review includes models for attentional processes and processes related to the hypothalamic–pituitary–adrenal axis, likely to be of relevance for IBS. However, the authors do also review models for sensitization, which, according to the present results, may be of particular relevance, preferably in combination with traditional IBS treatments, such as changed diet, probiotics, exercise, and medication (e.g. antidepressants).
Whereas strengths of this study include being population-based, having a large sample size, and that the county of Västerbotten has an age and sex distribution that is very similar to that of Sweden in general (Statistics Sweden, 2016), it does also have limitations. One such limitation is the relatively low response rate (40%), which may have resulted in a selection bias, with implications for the representativeness. Noteworthy, the effect of selection bias has been shown to vary very little between response rates of 30 and 70 percent (Galea and Tracy, 2007). Other limitations are having to rely on the participants’ reports of having been given a diagnosis by a physician and the lack of information on time for the diagnoses being given. Furthermore, caution should be taken regarding the size of the ORs since the confidence intervals are large.
In conclusion, despite limitations, the results from this study suggest that persons with IBS experience intolerance, albeit weak, to environmental odorous/pungent chemicals and sounds. The high comorbidity in the IBS sample with other types of FSS and psychiatric disorders is in accordance with the notion of central sensitization in IBS. This result together with the found association between IBS and environmental intolerance does also provide indirect support for central sensitization in intolerance to chemicals and sounds.
Footnotes
Acknowledgements
This study is an extension of an undergraduate thesis by Linnea Ståhlberg.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from the Swedish Asthma and Allergy Association’s Research Fund (2012030-K), the Swedish Council for Working Life and Social Research (2011-0396), the Swedish Foundation for Humanities and Social Sciences (M14-0375: 1), and the Graduate School in Population Dynamics and Public Policy, Umeå University.