
Abstract
This study analyses the factor structure and psychometric properties of the Chinese version of Beck Anxiety Inventory on Chinese doctors. Participants include 762 doctors sampled in 18 public hospitals in three cities in Eastern China. Exploratory factor analysis is employed to identify the potential factor structure of the inventory. Confirmatory factor analysis is referred to for model fit. The results indicate that the Chinese version of Beck Anxiety Inventory has satisfactory reliability and validity, but its factor structure is unstable and has great differences compared with international versions. Naming the four extracted factors is difficult. In general, the Chinese version of Beck Anxiety Inventory is appropriate for Chinese doctors and can be used as a good screener to detect the anxiety of Chinese doctors.
Introduction
Beck Anxiety Inventory (BAI) is a popular and common scale used to measure people’s subjective feelings about anxiety. BAI, developed by Aaron T Beck et al. in 1988, reflects the extent of respondent disturbance from many kinds of anxiety symptoms through self-rated results (Beck et al., 1988). BAI has 21 self-rated items and is currently widely applied for psychological assessment of clinical patients and self-rating of general populations. However, few studies have examined the measurement of highly anxious risky professionals, nor have they explored the factor structure and psychometric properties of the Chinese version of BAI. This study aims to employ BAI to measure the anxiety of young Chinese clinical doctors, as well as analysing the factor structure and psychometric properties of this scale.
Various groups in China suffered from mental disorders (Liang et al., 2014; Liang and Cao, 2015; Liang, 2015). Among those, doctors are professionals with a high anxiety risk. Medical workers not only shoulder the responsibility of curing patients on a daily basis but also face pain, disease, death, emergency and the risk of being infected, which greatly affect psychological health (Wang et al., 2010). In China, doctors face great occupational pressure and work overloading. The conflict between high patient volume and limited medical resources forces Chinese doctors to overwork, causing exhaustion (Chen et al., 2013). Furthermore, China is currently in a stage of medical system reformation, transforming from traditionally disease-centred to patient-centred, for the purpose of maintaining and improving patients’ quality of life. This transformation has exacerbated work difficulties for doctors and increased occupational pressure (Steer et al., 1993; Wu et al., 2010). Additionally, doctors are predisposed to suffer from mental disorders such as anxiety, depression, exhaustion and burnout (Peterson et al., 2008).
In fact, studies have been conducted on the anxiety of Chinese doctors, with sampling populations including citizens living in cities in Northeast and South China. Results have shown that anxiety symptoms were very common among Chinese doctors. More than half of Chinese professionals had anxiety symptoms and among Chinese physicians, approximately 25.67 percent suffered from anxiety symptoms (Gong et al., 2014). Lifestyle, work environment and work burnout are important factors that influence anxiety in Chinese doctors (Gong et al., 2014; Sun et al., 2012). In particular, compared with older doctors with ample experience, young doctors had stronger feelings of burnout; their psychological conditions were more worrisome. As well as having to face work pressure, they also experienced stress caused by updated knowledge, improved techniques and job promotions (Schaufeli et al., 2009). Furthermore, poor mental health in doctors negatively affects attitude towards patients, leading to misdiagnosis and even increasing suicide rates among doctors (Hawton et al., 2004).
As a fast improving and commonly used anxiety inventory, BAI has been used among different populations in many countries. However, the participants of these studies were mostly from the general population and patients; only a few studies have focused on anxious and risky professionals, such as physicians (Ahmed et al., 2009). In addition, the Chinese version of BAI has not been thoroughly explored. With samples of outpatients in Hong Kong hospitals, Leung (2001) extracted two factors, physiological response and anxious thought. These factors were considered consistent with the logic of the cognitive behavioural theory that explains anxiety. However, this conclusion has not been fully investigated. Few studies have explored the factor structure and psychometric properties of BAI among Chinese people. This study employs BAI to measure anxiety among Chinese young doctors and analyses the factor structure and psychometric properties of the Chinese version of BAI among medical professionals. This study aims to: (1) explore the factor structure and psychometric properties of the Chinese version of BAI among Chinese people, providing more empirical evidence for BAI development and improvement and (2) by studying the reliability and validity of the Chinese version of BAI, promote the use of BAI for clinical measurement and self-rating.
Methods
Participants
Participants were Chinese doctors working in public hospitals. During the sampling procedure, we designed and conducted a cross-sectional study, selecting three cities with comparatively developed economies in East China (Shanghai, Nanjing and Hangzhou). These cities have better urban construction and more complete and professional hospitals, so they have certain representativeness as sample regions. Two hospitals were then randomly selected from three levels of public hospitals (district, city and province) in each city, and 50 doctors aged 15–44 years old were sampled from each hospital. In the process of distributing the questionnaire, participants were first asked whether they were willing to accept the investigation and state principles, such as confidentiality and authenticity in advance. Subsequently, participants were asked to complete the questionnaire independently. If they did not understand any items during the completion process, they could consult the investigator on the site. Ultimately, 900 questionnaires were distributed, that is, 300 questionnaires per city. A total of 762 questionnaires were returned, with an effective rate of 84.67 per cent.
Participant information included gender, age, education, marital status, job title, last monthly income and work hours per day. The population was composed of 58.18 per cent male doctors and 41.82 per cent female doctors. The mean age of participants was 34.08 years. Education was categorised into five levels from junior college and below to doctoral and post-doctoral degree. Approximately 32.58 per cent of participants held a master’s degree. Most participants were attending physicians, accounting for 37.77 per cent of the sample population. In addition, 50.81 per cent of participants were married. Most participants’ salaries ranged from Chinese Yuan (CNY) 3000 to CNY 5000; regarding working hours, 42.01 per cent of participants indicated that they worked 12–14 hours daily.
Tools
This study uses BAI to measure the anxiety of Chinese doctors. BAI has 21 self-rated items. All answers have four options (1 = not at all, 2 = mildly, 3 = moderately and 4 = severely). The total score is the summary of all items, ranging from 21 to 84. A higher score indicates more severe anxiety.
Previous research has indicated that BAI has satisfactory reliability and can effectively distinguish anxiety diagnostic symptoms. BAI is an easy-to-use and convenient clinical tool that diagnoses people’s subjective anxiety symptoms, and has simple but concise items that are easy to understand and handle (Beck et al., 1988). Previous studies have applied BAI to different population groups in many countries to explore its reliability and validity. Participants included community residents of different ages, such as adolescents (Osman et al., 2002), adults (Chapman et al., 2009; Osman et al., 1993) and the elderly (Le Roux and Kemp, 2009). Many studies focus on patient groups, including outpatients and inpatients (Chen et al., 2013; Steer et al., 1993, 1994). In addition, many language versions of BAI have been proven to be acceptable, such as Spanish (Magán et al., 2008), Persian (Kaviani and Mousavi, 2008) and Turkish (Ulusoy et al., 1998). Although few studies have focused on the applicability of BAI among the Chinese population, the Chinese version has also been proven to be reliable and valid (Che et al., 2006; Leung, 2001). Leung (2001) applied the Chinese version of BAI to diabetic patients and cancer patients, indicating that the inventory is a reliable and valid instrument. Che et al. (2006) employed the Chinese version of BAI among psychiatric outpatients and reached the same conclusion.
The majority of previous studies extracted 2–6 factors from 21 items. The first factor analysis was conducted by Beck with a sample of 160 psychiatric outpatients. It revealed two factors: subjective (nine items) and somatic (21 items), which were positively and moderately correlated (r = 0.56). However, the factor loadings for some of the items were rather low. There is a series of existing models that yielded a two-factor structure similar to the original model described by Beck et al (Schaufeli et al., 2009). Using a sample of 108 psychiatric inpatients, Kumar et al. (1993) extracted two factors similar to Beck’s, which could explain 79 per cent of the entire variance. The Chinese version of BAI has also been used to measure factor structures among outpatients in Hong Kong hospitals. Results indicated the two factors, physiological response and anxious thought, were consistent with the logic of the cognitive behavioural theory explaining anxiety (Leung, 2001). However, other studies found the original two-factor structure was not appropriate for non-clinical samples (Schaufeli et al., 2009) because it insufficiently distinguished a normal population in the absence of an external stressor (Creamer et al.,1995). In conducting an exploratory factor analysis (EFA) of a sample of 225 non-clinical adults, Osman recognised that two-factor models were inappropriate and he consequently extracted four factors (Osman et al., 1997). With a sample of 197 disadvantaged older medical outpatients, Wetherell also revealed four factors, indicating that BAI could serve as a valuable screening test for anxiety symptoms among older primary care patients (Wetherell and Areán, 1997). Furthermore, a study extracted six factors through principal axis factoring with orthogonal rotation (Morin et al., 1999). In general, a consensus regarding the most stable factor structure has not been reached. Therefore, exploring the factor structure of BAI is necessary.
Data analysis
This study uses EFA to identify the potential factor structure of the Chinese version of BAI among participants. Confirmatory factor analysis (CFA) is referred to for model fit. A 5 per cent level of significance test is used for all significance tests. AMOS™ 21.0 is used for CFA models and SPSS version 22.0 is used for EFA and other statistics tests. Thus, with this step-by-step analysis, we examine the reliability and validity of the Chinese version of BAI among Chinese doctors.
Results
Factor structure analysis
First, EFA is conducted on BAI to identify potential latent variables, using the principal axes extraction method with promax rotations (k = 4). In deciding the numbers of factors extracted from the EFA, the following criteria were used: Kaiser’s thumb rule (eigenvalue > 1.0) and the scree test (Cattell, 1978). Ultimately, a four-factor model was retained as the best model. Table 1 shows the results, indicating that the Kaiser–Meyer–Olkin (KMO) measures the sampling adequacy of BAI as 0.98 and the Bartlett test results pass the significance test (approximated chi-square = 5089.62, df = 210, p < 0.001). The measurement of sampling adequacy (MSA) is above 0.9 and the factor analysis results are satisfactory. Four factors can be extracted. F1, F2, F3 and F4 are the abbreviations of Factor 1 (items 1, 11, 12, 14, 17 and 21), Factor 2 (items 2, 5, 8, 10, 19 and 20), Factor 3 (items 3, 7, 15, 16 and 18) and Factor 4 (items 4, 6, 9 and 13), respectively. All factor loadings that permit the assignment of an item to a specific factor exceed 0.4, while the others are less than 0.3. The cumulative variance of four factors is 56.83 per cent, indicating that they can explain 56.83 per cent of BAI variation.
Summary of factor analysis results of BAI.

BAI: Beck Anxiety Inventory; KMO: Kaiser–Meyer–Olkin; MSA: measurement of sampling adequacy.
Bold value indicate the factor whose factor loading was more than 0.40.
By referring to the CFA model of naming methods for factors in previous studies using different versions of BAI among different kinds of populations (Borden et al., 1991; Fydrich et al., 1992; Sun et al., 2012), the four factors are first given abbreviated names of F1, F2, F3 and F4. However, more careful and serious discussion about how to correctly name them is required. Accordingly, the CFA models are established, as shown in Figure 1. The 21 items of BAI (B1–B21) are observed variables. The four factors (F1–F4) are latent variables, which correlate with each other.

CFA initial model of BAI.
Table 2 shows the estimation results of the CFA models. All regression coefficients pass the significance test at the level of 0.001. The values of standard errors (SE) are close to 0, and all critical ratios (CR) are over 2. In addition, all standardised regression coefficients are between 0.5 and 1.0, indicating that the coefficients are reasonable.
CFA model results.
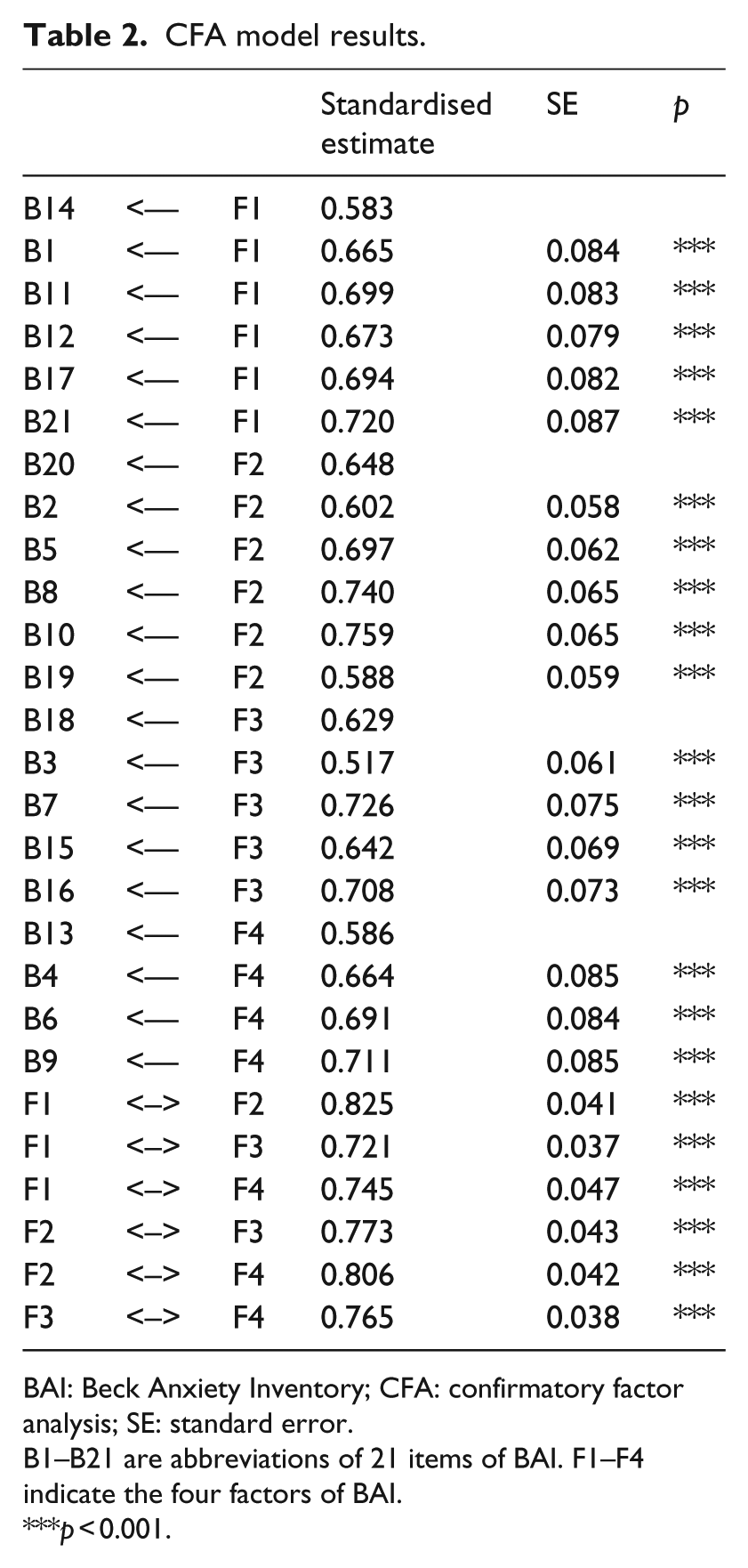
BAI: Beck Anxiety Inventory; CFA: confirmatory factor analysis; SE: standard error.
B1–B21 are abbreviations of 21 items of BAI. F1–F4 indicate the four factors of BAI.
p < 0.001.
Finally, the correlations between the four factors are strong and significant. Among the correlations, the largest is between F1 and F2 (0.825). In terms of model fit indexes, the chi-square statistic is 188.896 and the degree of freedom is 183. The comparative fit index (CFI) is 0.999, the normed fit index (NFI) is 0.974 and the incremental fit index (IFI) is 0.999, all are close to 1. Furthermore, the root mean square error of approximation (RMSEA) is 0.047 (0.043–0.052), which is less than 0.05, indicating that the model fit is good.
Reliability analysis
Table 3 shows the Cronbach’s alpha coefficient and correlation coefficients. The total Cronbach’s alpha coefficient of BAI is 0.940. All the coefficients of each factor are above 0.7. The four-factor structure of BAI is reasonable. Finally, the four factors have high correlation with BAI (between 0.8 and 1.0).
Reliability analysis and correlation of BAI.

BAI: Beck Anxiety Inventory.
Discussion and conclusion
This study samples doctors working in public hospitals in Eastern China, employs the Chinese version of BAI to measure the characteristics of their anxiety symptoms and explores its factor structure and reliability. In addition, the study intends to explore the factor structure of the Chinese version of BAI, providing more empirical evidence for BAI promotion and anxiety measurement development. The main research findings are as follows:
1. Most participants are middle-aged adults with a high level of education but low-level job titles (attending physician). Their work hours are usually more than 12 per day, but with relatively low salary.
Previous research found that lengthy work hours were an important factor that leads to poorer quality of life among medical professionals than in general populations (Wu et al., 2010; Liang and Guo, 2015; Liang, 2016). Similarly, long work hours and frequent night shifts potentially damage the physical health of Chinese doctors, causing anxiety or depression disorders (Sun, 2012). Thus, improving the psychological capital of Chinese doctors is essential (Liu et al., 2012).
2. As previously mentioned, the construct validity and factor structure are satisfactory. The Chinese version of BAI is reliable and valid, which is consistent with the findings of previous studies (Le Roux and Kemp, 2009). The factor loadings are also very high (0.40–0.93). The CFA results also show that the model fit is good, indicating the four-factor structure is appropriate for the Chinese version of BAI.
The factor structure exploration finding for the Chinese version of BAI is similar to those of other international versions (Leyfer et al., 2006; Osman et al., 2002), that is, the original two-factor structure is not appropriate for the different language versions of BAI. However, the results of this study are inconsistent with the findings of previous studies on the Chinese version of BAI. With samples of outpatients in hospitals, both studies by Leung and Che obtained a two-factor solution (Che et al., 2006; Leung, 2001). This is mainly because both Leung and Che’s research applied the Chinese version of BAI to the outpatients. However, as a high-risk occupation, doctors have higher qualifications, more specific occupational characteristics and work environments; thus, the characteristics of their anxiety symptoms are different from those of outpatients. In general, the present empirical evidence clearly indicates that the four factors have very good discrimination and the general fit effect is satisfactory. Therefore, the results of this study provide reference data on the factor structure of BAI.
3. The factor structure, however, is not very stable, which means it has limited applicability. F1 has the largest factor loading for item 1 and item 11, but the CFA results show that F1 has the greatest correlation with item 11 and item 21. F2 has the greatest factor loading for item 2 and item 19, while the CFA results indicate that its correlations with item 8 and item 10 are the strongest. Similarly, F3 has the greatest factor loading for item 3 and item 18, but has the strongest correlation with item 7 and item 16. As for F4, the factor loadings of item 6 and item 13 are the largest, while the correlations with item 6 and item 9 are the strongest, as indicated by the CFA results. Therefore, in the Chinese version of BAI, only the relationships between F2 and item 11 and between F4 and item 6 are relatively stable. Other relationships might not be applicable for other participant groups.
Therefore, naming the four factors is difficult. Previous studies did not originally define the specific corresponding factors of each factor. Substantial differences in factor structure exist between different versions of BAI among different respondent groups, as in the case of this study. Before starting the data analysis, one question was asked, ‘Which factor structure is appropriate for the Chinese version of BAI among Chinese doctors: the two-factorial structure (physiological response and anxious thought) or the four-factorial structure (subjective, automatic [somatic nervousness], panic, neurophysiological)?’ However, based on the two stable relationships in the research findings, the naming of F1–F4 still could not be inferred. The eleventh item (B11: choking) definitely corresponds to the physiological response domain, but it is unclear which factor it belongs to (i.e. either automatic or neurophysiological). At the same time, the sixth item (B6: dizzy) should have corresponded to the anxious thought domain, but we are not sure which factor it belongs to (i.e. either subjective or panic). Based on other weaker relationships, reliable inference is not possible. Therefore, the factor structure of the Chinese version of BAI cannot be completely consistent with other international versions, as more evidence and justification are needed to complete and verify the structure.
Finally, the reliability analysis results show that BAI has very high internal consistency. The four-factor structure is compact with strong correlations, indicating the Chinese version of BAI is very reliable and valid among Chinese doctors. However, whether the conclusions might only be applicable among Chinese doctors needs to be clarified. Participants of this study are highly professional groups, with a high level of education and with special occupational features and work environments. Considering these special features, the characteristics of their anxiety symptoms cannot be generalised in other general groups. In addition, the factor structure is not very stable and not completely consistent with the international version of BAI. Furthermore, a consensus regarding the most stable factor structure has not been reached. Thus, naming the four factors is difficult. The instability of the Chinese version of BAI among Chinese doctors implies that more studies are needed for modification and improvement in the future. Generally, the Chinese version of BAI is appropriate for professional groups and can be used as a good screener tool to detect the anxiety symptoms of Chinese doctors.
This study also has some limitations. First, all of the participants are from Shanghai, Nanjing and Hangzhou, three of the largest cities in East China. However, no focus is put on central and western China, where there are also many doctors with anxiety symptoms. Thus, the range is relatively small. Second, the study examines the factor structure of the Chinese version of BAI and extracts four factors. However, naming these four factors of BAI among Chinese doctors is difficult, and there are also two-factor and six-factor BAI solutions from previous studies. No consistent conclusion has been reached. Therefore, to obtain more BAI information regarding Chinese doctors, further studies are needed.
Footnotes
Acknowledgements
Y.L. wrote and revised the manuscript, was responsible for the design of the study and performed the statistical analysis. L.W. and Jianbo Zhu revised the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This paper is supported by the National Natural Science Funds for Excellent Young Scholar of 2016: Social Security and Social Policy, the General Program of National Natural Science Foundation of China: health-related quality of life (HRQOL) and professional social work intervention model for earthquake survivors of post disaster reconstruction: a follow-up survey of six earthquake hit areas in Lushan (71473117), research on the interaction between local government ecological management and the development of green community volunteer organization – a study on the construction of green ecological city in Yangtze River Delta (71173099), and the key project of the National Social Science Fund (16AZZ014).