
Abstract
Poor breast cancer–related quality of life is associated with flattened cortisol rhythms and inflammation in breast cancer survivors and women with advanced disease. We explored the associations of cancer-specific distress (Impact of Events Scale), mood (Profile of Mood States), activity/sleep (wake after sleep onset, 24-hour autocorrelation coefficient) and cortisol (diurnal slope) circadian rhythms, and inflammation (interleukin-6) with quality of life (Functional Assessment of Cancer Therapy–Breast) among patients awaiting breast cancer surgery (N = 57). Models were adjusted for differences in age and cancer stage. Distress and mood disturbance were significantly correlated with lower quality of life. Ethnic differences in the relationship between distress and mood disturbance with global quality of life and subscales of quality of life were observed. Actigraphic measures showed that in comparison with non-Hispanic patients, African Americans had significantly poorer activity/sleep (wake after sleep onset, 24-hour autocorrelation coefficient). Circadian disruption and inflammation were not associated with quality of life. Physiological dysregulation and associated comorbidities may take time to develop over the course of disease and treatment.
Introduction
Quality of life (QOL) is especially important when quantity of life is threatened. Breast cancer patients commonly experience distress, poor sleep, circadian disruption, and altered systemic immune imbalance. Each of these may contribute to a patient’s QOL.
Breast cancer can be thought of as a series of stressors related to diagnosis, treatment, functional capability, and social roles. Psychological distress is common in breast cancer patients and encompasses sadness, depression, anxiety, and social isolation (Mertz et al., 2012). Breast cancer patients experience more mood disturbance and greater emotional lability than healthy women (Stanton, 2006). Distress related to diagnosis worsens with cancer-related physical impairment (Glanz and Lerman, 1992; Portenoy et al., 1994). Nearly 40% of women with breast cancer experience ongoing mood disturbance, symptoms of fatigue, and poor QOL for years after treatment (Carlson et al., 2004; Von Ah and Kang, 2008).
Insomnia often exacts a toll on QOL of a patient with cancer (Savard and Morin, 2001) and is particularly prevalent among breast cancer patients and survivors (Davidson et al., 2002). Although insomnia symptoms are pervasive during radiation and chemotherapy treatment (Palesh et al., 2013), many women report sleep disturbance prior to treatment (Ancoli-Israel et al., 2006), and symptoms often persist long after treatment has concluded (Dow et al., 1996). While sleep disturbance is likely exacerbated by the cancer experience and subsequent treatment (Savard and Morin, 2001), the exact timeline for sleep disturbance among breast cancer patients remains unclear. Sleep disturbance is associated with poorer functional and physical well-being prior to adjuvant or neo-adjuvant chemotherapy (Ancoli-Israel et al., 2006), although more information on sleep disturbance during this pre-treatment period is warranted. Importantly, sleep disturbance is most problematic among minority patients (Otte et al., 2010) and affects not only the quality but also the quantity of life. Sleep disruption, particularly wake after sleep onset (WASO), has been shown to be associated with poorer social and emotional well-being in patients with lung cancer (Dean et al., 2015) and to predict early mortality in patients with breast cancer (Palesh et al., 2014). Additionally, rest-activity rhythms (i.e. 24-hour autocorrelation coefficient) has been shown to be related to overall QOL and physical, emotional, and social functioning in metastatic colorectal cancer patients, such that more coordinated rhythms were associated with better QOL (Mormont and Waterhouse, 2002).
Sleep disruption may be one manifestation of central nervous system (CNS)-regulated circadian disruption (Ancoli-Israel et al., 2006; Eismann et al., 2010). Circadian disruption is common in advancing cancer and is strongly correlated with poor QOL across several cancer types (Innominato et al., 2009). Aberrations of the diurnal cortisol rhythm, a marker of central circadian rhythms (Dickmeis et al., 2013), are linked with fatigue among breast cancer survivors (Bower et al., 2005) and decreased global QOL across diverse cancer types (Carlson et al., 2004). Compelling new research has shown conclusively that circadian disruption accelerates tumor progression (Eismann et al., 2010; Escobar et al., 2011; Fu and Lee, 2003). Several independent clinical studies demonstrate that disrupted circadian rhythms predict early mortality among patients with metastatic breast (Sephton et al., 2000), metastatic colorectal (Innominato et al., 2009), renal cell (Cohen et al., 2012), lung (Sephton et al., 2013), and ovarian cancers (Schrepf et al., 2015).
Circadian disruption may exacerbate detrimental psychoneuroimmune effects on cancer QOL and impair tumor defense mechanisms (Cash et al., 2015; Eismann et al., 2010). Flattened or aberrant patterns of cortisol secretion are associated with elevated proinflammatory markers and poorer cancer QOL (Miller et al., 2008). Immune dysregulation may accelerate progression of some cancers (Coussens and Werb, 2002). Notably, interleukin (IL)-6 has been associated with increased fatigue and exacerbation of anxiety and depressive symptoms, which affect QOL in cancer patients (Cleeland et al., 2003; Seruga et al., 2008). Among breast cancer patients tested before chemotherapy, inflammatory markers predict greater QOL decrements after treatment (Mills et al., 2005).
Clinical profiles vary across ethnicities, as does QOL. Breast cancer incidence is highest among non-Hispanic Whites, but African Americans suffer the highest mortality, which may be explained by barriers to access to care (DeSantis et al., 2011). However, it has also been suggested that this disparity may be explained by other factors (Chlebowski et al., 2005). African Americans are often diagnosed in more advanced stages with larger, higher-grade tumors (Middleton et al., 2003). Minority patients experience more distress and poorer QOL as compared with their non-Hispanic White counterparts during and after treatment (Carlson et al., 2004; Smith et al., 2009). QOL is also linked with poor access to and low rates of participation in cancer support groups (Janz et al., 2009), which have been shown to affect survival among metastatic breast cancer patients (Spiegel et al., 1989). It has also been suggested that disparities in survival rates among non-Hispanic White and African American breast cancer patients may be attributable to racial differences in patterns of care (Diehr et al., 1989), as well as noncompliance with therapy and incomplete treatment adherence, which may be related to socioeconomic status (Baquet et al., 2008). African American women have been shown to terminate chemotherapy prematurely and are less likely to receive surgical removal of tumors, compared to non-Hispanic White counterparts (Bradley et al., 2002; Hershman et al., 2005). Additionally, biological factors such as differences in genetic and tumor phenotypes may also be viable explanations for survival differences (Baquet et al., 2008).
Ethnic differences in QOL may also be mirrored in physiology. Compared with non-Hispanic Whites, African American patients demonstrate a higher prevalence of flattened cortisol slopes that are tightly linked with distress (Cohen et al., 2006; DeSantis et al., 2015). African Americans also display elevated circulating inflammatory biomarker IL-6 (Stowe et al., 2010).
Much of the QOL literature comes from breast cancer patients actively in treatment, those who have concluded treatment, or who have remained disease-free 5 or more years after treatment (i.e. survivor status). Relatively little work has explored factors of QOL prior to cancer treatment. However, early responses to the stress of diagnosis predict long-term behavioral symptoms (Dupont et al., 2014). A patient’s initial cancer-related distress can influence adherence to treatment, health behaviors, and subsequent stress responses to ongoing cancer-related challenges, thereby affecting downstream physiological pathways of cancer outcomes (Andersen et al., 1994). We explored these relationships in this early period, positing as factors of QOL: distress, mood disturbance, disrupted circadian sleep and activity patterns, altered diurnal cortisol rhythms, and elevations in the systemic proinflammatory marker, IL-6. Associations were explored in ethnic subgroups.
Methods
Participants
In all, 57 breast cancer patients were recruited from two clinic sites in conjunction with a treatment planning appointment with the breast surgical oncologist. The same surgical oncologist served both clinics. Women underwent a pre-treatment biopsy with intent to verify malignancy and then completed assessments. Research assistants provided informed consent. Participants were English speakers with no active psychoses (i.e. hallucinations and/or delusions). Medical records provided data on disease (i.e. stage, tumor size, diagnosis date, estrogen receptor (ER), progesterone receptor (PR), human epidermal growth factor receptor 2 (HER2)/neu receptor status) and functional status (i.e. Karnofsky rating; Table 1). Patients reported demographics (Table 1), distress, and QOL and provided home-based rest/activity and salivary cortisol data over 3 days. IL-6 was measured in serum.
Demographic and medical characteristics of the sample (N = 57).
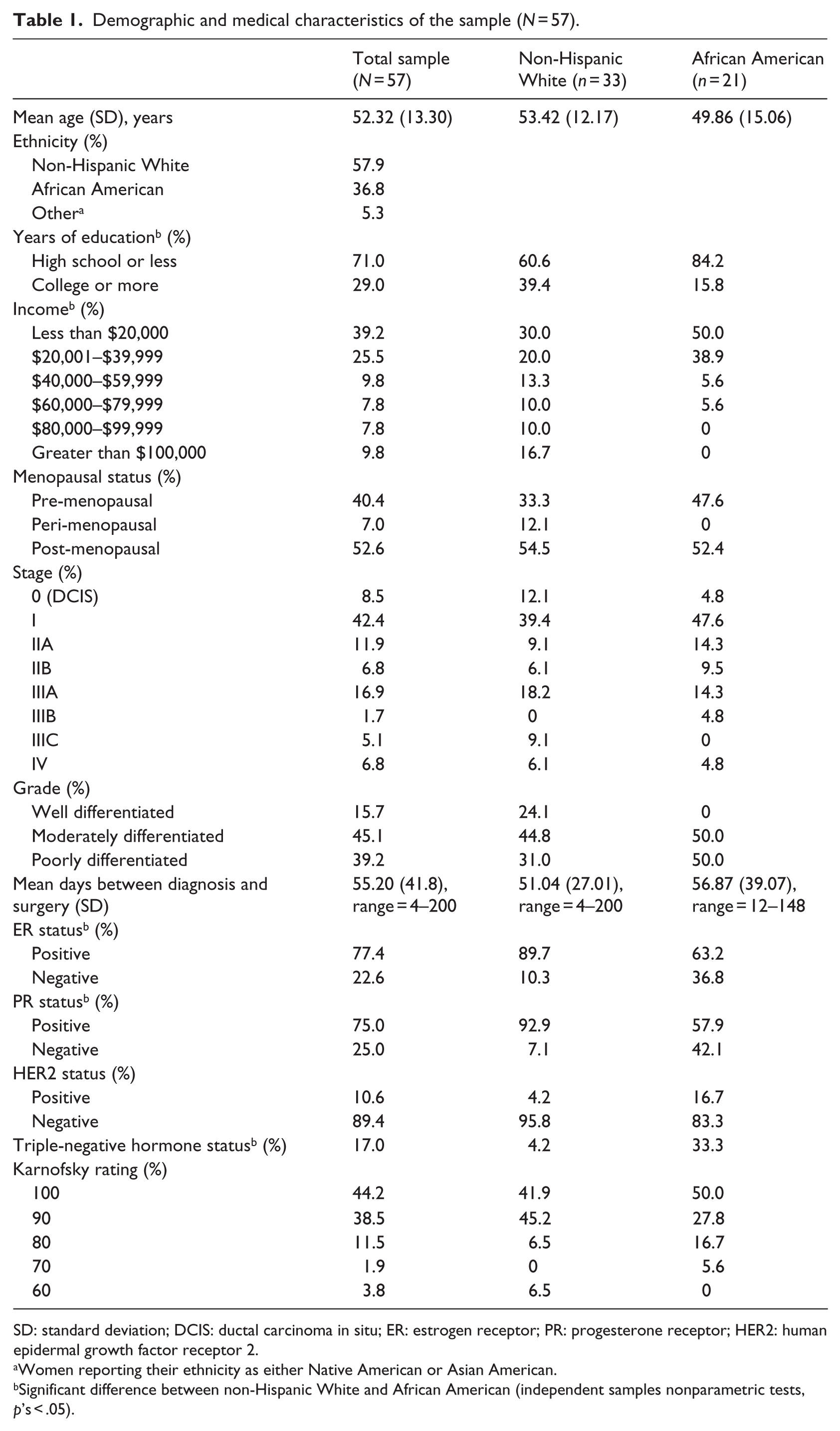
SD: standard deviation; DCIS: ductal carcinoma in situ; ER: estrogen receptor; PR: progesterone receptor; HER2: human epidermal growth factor receptor 2.
Women reporting their ethnicity as either Native American or Asian American.
Significant difference between non-Hispanic White and African American (independent samples nonparametric tests, p’s < .05).
Measures
Psychological distress
The 15-item Impact of Events Scale (IES; Horowitz et al., 1979) was used to assess for frequency of intrusive and avoidant thoughts regarding a cancer experience from the current day, a measure that has previously been used in breast cancer samples (Cordova et al., 1995). Patients also rated mood over the past week on the Profile of Mood States (POMS), a 65-item measure (McNair et al., 1971) frequently used in cancer settings (Stanton et al., 2000). IES total and POMS total mood disturbance (TMD) scores were calculated. Cronbach’s alpha was used to indicate the internal consistency of items in our two measures of distress, the IES and the POMS. For the IES, the internal consistency was α = .89, and for the POMS-TMD, it was α = .92.
Actigraphy
Sleep characteristics and circadian rest/activity rhythms were measured over three days and four nights via wrist-worn actiwatches (Ambulatory Monitoring Inc., Ardsley, NY, USA). These data yielded two summary variables: as a measure of sleep, we used the mean time awake after initial sleep onset (WASO). As a measure of circadian rhythmicity (i.e. day-to-day variability in the rest/activity rhythm), we used the 24-hour autocorrelation coefficient.
Endocrine disruption
Participants collected saliva at waking, waking + 30 minutes, 4 p.m., and bedtime for cortisol assessment over 3 days. Samples were frozen at −80°C until assay (Salimetrics, Inc., State College, PA, USA). Assays were within an acceptable range (previously described; Dedert et al., 2012). Diurnal cortisol slope was calculated, excluding + 30-minute samples, using the unstandardized beta of log-transformed cortisol regressed on collection time (Kraemer et al., 2006).
Immune function
Blood was drawn by a trained phlebotomist and serum aliquots were frozen at −80°C. Since biomarkers of interest are known to exhibit circadian patterns of release in systemic circulation (Kronfol et al., 1997), the timing of blood draw was restricted as much as possible. Our clinic scheduled all new patients at 11 a.m. and 1 p.m. The mean blood collection time was 1:15 p.m. (standard deviation (SD) = 119 minutes; median = 1:32 p.m.); none was postprandial. IL-6 was assayed in serum samples using an electrochemiluminescent quantitative sandwich immune assay (Meso Scale Discovery, Gaithersburg, MD, USA). Assay plates were imaged on a SECTOR Imager 2400A and data analyzed using Discovery Workbench software (Meso Scale). For IL-6, the low limit of detection was 0.09 pg/mL. Intra-assay coefficient of variation (CV) was 5.2%, and the inter-assay CV was 3.1%. No sample fell below the low limit of detection. Raw data were log-transformed.
Health-related QOL
The Functional Assessment of Cancer Therapy–Breast (FACT-B) is a 44-item self-report measure of QOL used in breast cancer samples (Brady et al., 1997). Subscales include physical, emotional, functional, and social well-being, and breast cancer–specific concerns. Greater QOL is represented by higher summary, physical, emotional, functional, and social well-being, and cancer-specific concerns’ scores. The summary score (primary analyses) and all subscales (secondary analyses) were entered as dependent variables in analyses. Table 2 presents descriptive statistics for variables of interest.
Descriptive statistics for variables of interest.
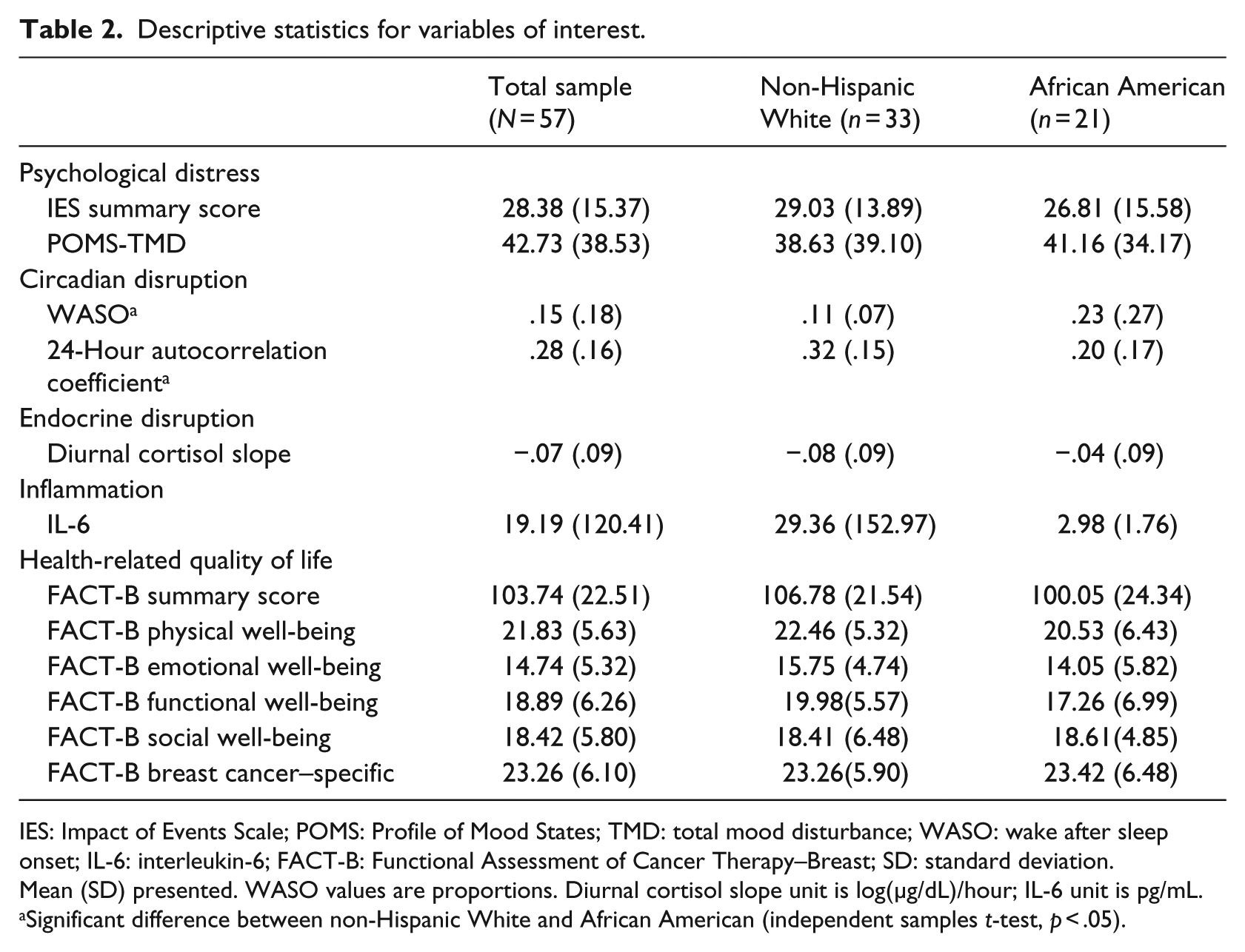
IES: Impact of Events Scale; POMS: Profile of Mood States; TMD: total mood disturbance; WASO: wake after sleep onset; IL-6: interleukin-6; FACT-B: Functional Assessment of Cancer Therapy–Breast; SD: standard deviation.
Mean (SD) presented. WASO values are proportions. Diurnal cortisol slope unit is log(µg/dL)/hour; IL-6 unit is pg/mL.
Significant difference between non-Hispanic White and African American (independent samples t-test, p < .05).
Statistical analyses
All data were confirmed to meet analytic assumptions using the skewness statistic. Two theoretically derived control variables, age at diagnosis (Linden et al., 2012) and cancer stage (Iwatani et al., 2013), were chosen, as both are associated with psychosocial distress (Andersen et al., 1994; Antoni et al., 2006). Tumor receptor status was not included as a control variable because this presurgical sample had not yet received this information or undergone any treatment differentiated by receptor status.
Primary analyses
Multiple linear regression models tested relationships between self-reported indicators of distress and QOL, actigraphically recorded circadian disruption and QOL, salivary cortisol rhythm dysregulation and QOL, and serum IL-6 and QOL. The two control variables were entered in the first block in each analysis; predictors were entered separately, one per regression, in the second block. The QOL summary score was entered as the dependent variable.
Secondary analyses
The sample was grouped by ethnicity to explore differences between non-Hispanic White women (n = 33) and African American women (n = 21). Two women who did not report on ethnicity were excluded from analyses, as well as two Native American and one Asian American out of respect for potential cultural differences on QOL ratings. FACT-B subscales (physical, emotional, functional, and social well-being, and breast cancer–specific concerns) were entered separately, one per regression, as the outcome. Given the concern of limited power due to the small sample size of the two ethnic groups, a more stringent alpha level of .01 was adopted for secondary analyses.
Independent samples t-tests were conducted to describe differences between the ethnic subgroups. Significant differences were further explored using boxplots and regressions. Hypothesis tests were repeated in post hoc tests within these two ethnic subgroups adjusting for age and stage.
Results
Primary analyses
Descriptive statistics for variables can be found in Table 2. Cancer-specific distress (IES total) was associated with QOL, independent of age at diagnosis and cancer stage. Patients who reported greater cancer-specific distress reported lower overall QOL (β = −.511, p < .001, ΔR2 = .260). Patients with greater mood disturbance (POMS) had poorer QOL, independent of age at diagnosis and cancer stage (β = −.733, p < .001, ΔR2 = .466). Sleep (i.e. WASO), circadian rhythm (i.e. 24-hour autocorrelation coefficient), cortisol profiles (i.e. diurnal cortisol slope), and IL-6 were not significantly correlated with QOL.
Secondary analyses
Within the non-Hispanic White subgroup, the associations of cancer-specific distress (β = −.467, p = .001, ΔR2 = .216) and TMD (β = −.688, p < .001, ΔR2 = .354) with poorer QOL persisted. The African American subsample demonstrated associations of mood disturbance (β = −.862, p < .001, ΔR2 = .667) with poorer QOL.
Subscales of the FACT-B were then examined as separate outcomes. Table 3 presents the associations of cancer-specific distress and TMD with the QOL subscales for each ethnic subgroup. TMD was associated with poorer physical, functional, and breast cancer–specific well-being (all p’s ⩽ .005) in both samples. Among non-Hispanic White, but not African American patients, cancer-specific distress was associated with poorer emotional well-being and breast cancer–specific well-being, and TMD was associated with poorer emotional well-being (all p’s < .005). In contrast, no significant associations between cancer–specific distress and QOL subscales were noted among African American patients. However, African American patients with higher levels of TMD reported poorer social/family well-being (p < .001).
Significant associations of cancer-specific distress or mood disturbance with QOL subscales.
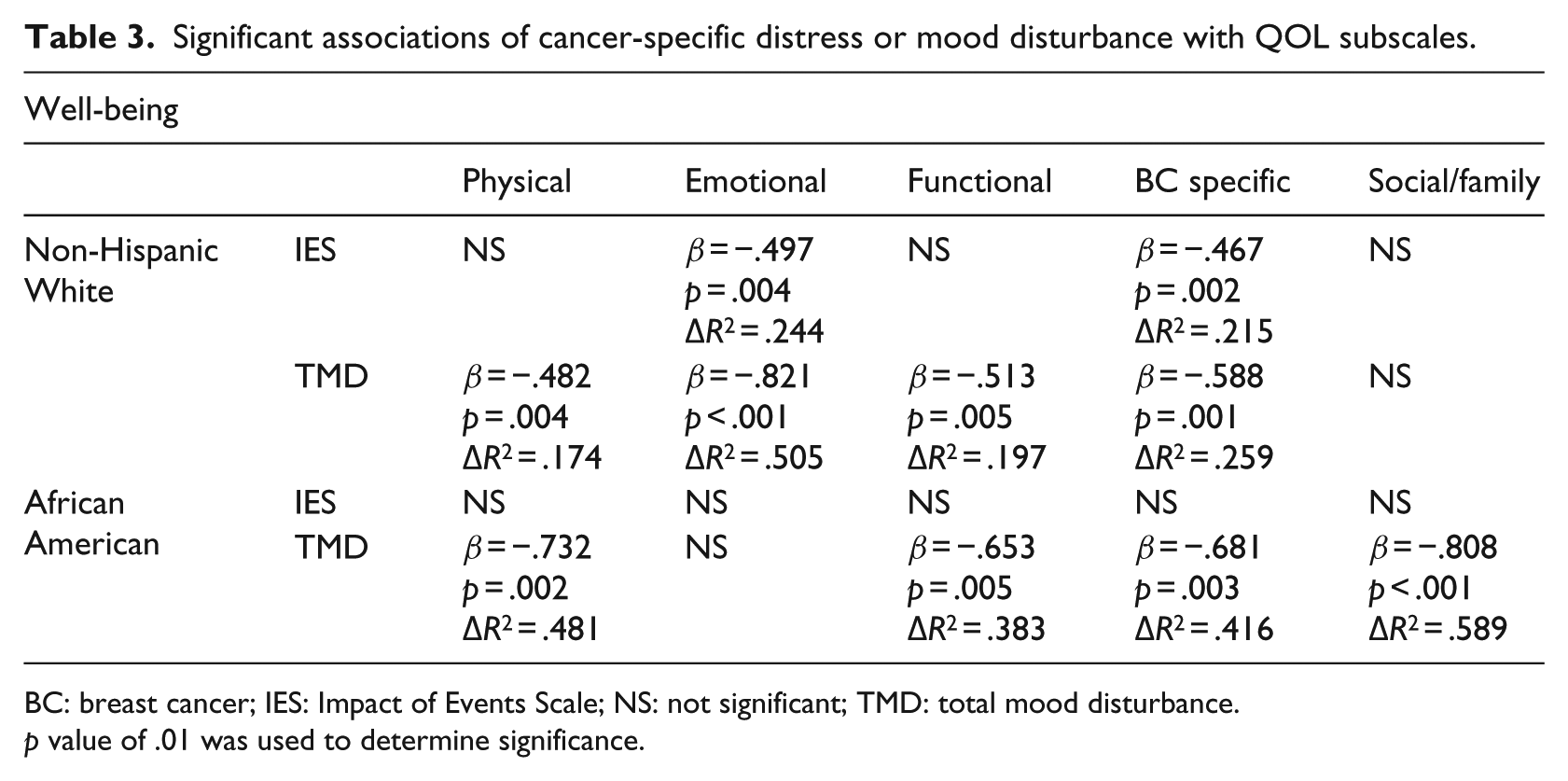
BC: breast cancer; IES: Impact of Events Scale; NS: not significant; TMD: total mood disturbance.
p value of .01 was used to determine significance.
African American women had significantly poorer sleep, as measured by WASO, and poorer circadian coordination, as measured by 24-hour autocorrelation coefficient (Table 2). Post hoc analyses revealed that these differences persisted after adjustment for differences in age and cancer stage (WASO: β = .353, p = .017, ΔR2 = .116; 24-hour autocorrelation: β = −.109, p = .037, ΔR2 = .093).
Discussion
Among women awaiting breast cancer surgery, QOL was associated with psychological but not physiological indicators of stress. Compared to data collected from women who have further progressed in the cancer trajectory, our findings suggest that stress-related physiological dysregulation takes extended time to accumulate over the course of cancer and treatment. Informative prior work has linked flattened cortisol rhythms and inflammation with fatigue and other signs of poor breast cancer QOL, but in the context of advanced disease or survivorship (Bower et al., 2005; Carlson et al., 2004; Miller et al., 2008). Because only a few studies have explored such biobehavioral interactions in the context of early or recently diagnosed disease, we looked for similar associations among presurgical breast cancer patients. We found no association of circadian, endocrine, or immune physiology with QOL during the presurgical period. Rather, presurgical patient’s QOL was associated only with their self-reported distress and mood disturbance. Perhaps the diagnosis and early treatment of breast cancer can be thought of as activating acute, as opposed to chronic, stress responses. Indeed, biobehavioral relationships characterizing acute stress can differ markedly from those patterns seen in individuals who have suffered for longer periods of time (i.e. months or years) with disease. Over time, the physical effects of cancer-based psychological stress may combine with those of treatment, resulting in worsening physiological dysregulation and, in turn, increasingly poor QOL.
Understanding the early psychological response to a cancer diagnosis is important: early psychological response is an indicator of behavioral symptoms over the longer term. Cancer-specific distress (i.e. intrusive thoughts) measured at the end of adjuvant treatment in a large breast cancer study predicted depressive symptoms, negative affect, pain, and poorer physical functioning at 1 year (Dupont et al., 2014). Interestingly, intrusive thoughts were not associated with symptoms that may be more physiologically driven, including fatigue, sleep, breast cancer-specific symptoms, and mental functioning (Dupont et al., 2014). The predictive value of persistent distress with regard to long-term psychological adjustment to cancer appears relevant across cultures (Lam et al., 2012). Clinical data show that distress during the preoperative period predicts greater immunosuppression postoperatively, leading to longer hospital stays, slower recovery, and higher risk of complications (Renzi et al., 2015). One intriguing finding suggests that brief presurgical psychosocial intervention may alleviate some degree of postsurgical immunosuppression (Larson et al., 2000). Even so, there are very few studies that have examined presurgical distress interventions.
We observed a divergence of psychological and physiological symptoms early in the disease trajectory. This is consistent with findings from Carlson et al. (2007), who found that women at a 1.36 years post-diagnosis stage demonstrated elevated distress, but did not differ from controls on physiological indices. In our sample, both cancer-specific distress and mood disturbance were significantly associated with poorer QOL. Among cancer patients undergoing treatment and within 5 years of treatment completion, depressed mood is one of the strongest correlates of fatigue, a factor integral to health-related QOL (Jacobsen et al., 2003).
We observed significantly poorer sleep (i.e. WASO) and circadian rhythmicity (i.e. 24-hour autocorrelation coefficient) among African American women (Table 2). To our knowledge, this is the first observation of its kind and differs from prior research examining actigraphically recorded sleep among breast cancer patients within 2 years of treatment (Budhrani et al., 2014). WASO scores were comparatively poorer in our sample, possibly indicating decrements in sleep during the stressful presurgical period. Because WASO and 24-hour autocorrelation coefficients were not associated with QOL in this sample, it seems unlikely that ethnic differences in QOL can be attributed to poorer activity/sleep in the African American patients. Promising initial data suggest that sleep parameters may respond to psychosocial interventions such as mindfulness-based stress reduction (Lengacher et al., 2015).
Research has shown that better sleep efficiency and fewer sleep disruptions are associated with lower mortality over a 6-year period within an advanced breast cancer sample (Palesh et al., 2014). Similarly, the 24-hour autocorrelation coefficient has demonstrated 5-year prognostic significance among patients with metastatic colorectal cancer (Innominato et al., 2009). It will therefore be important for future studies to consider examination of activity/sleep decrements as a factor related to ethnic differences in breast cancer survival. Further exploration is needed to clarify the sleep trajectory, identify disparate activity rhythms, and pinpoint onset of survival effects as well as impact on QOL.
Many risk factors for cancer incidence and progression differ across ethnicities. In comparison with non-Hispanic Whites, African American breast cancer patients suffer at an earlier age, with more advanced stage at diagnosis and more aggressive cancer types (Middleton et al., 2003), worse physical functioning (Paskett et al., 2008), more difficulty with pain, fatigue, and sleep (Northouse et al., 1999), poorer access to treatment, and lower sociocultural support. Access to treatment (e.g. chemotherapy) and stage at diagnosis strongly contribute to QOL (Janz et al., 2009; Krupski et al., 2006).
As expected, our African American participants appeared to have more difficult prognoses as measured by their younger age (mean 49.86 vs 53.42 years), fewer presenting in earlier or pre-cancerous phases of disease (e.g. 4.8% vs 12.1% were diagnosed with ductal carcinoma in situ (DCIS)), and, among those with confirmed malignancies, tumors that were more poorly differentiated (50.0% vs 31.0%), or had negative hormone receptor status, limiting treatment options (ER: 36.8% vs 10.3%, PR: 42.1% vs 7.1%, HER2/neu: 83.3% vs 95.8%). Notably, 33.3% of the African American participants had triple-negative hormone receptor status versus 4.2% of the non-Hispanic White women.
Our exploratory findings highlight some differences and some similarities across racial/ethnic subgroups with regard to the associations of distress and mood with QOL. In our sample, non-Hispanic White women with high cancer-specific distress had lower overall QOL, but this association was not significant in our subgroup of African American women. In contrast, a significant association of mood disturbance with poorer QOL was apparent in both racial/ethnic subgroups. Previous research with women with breast cancer suggests that, especially prior to surgery, African American women may report significantly less distress and depressive symptoms than non-Hispanic White women, although their distress levels may rise over time (Culver et al., 2002).
When QOL subscores were examined, poor mood was significantly associated with lower physical, functional, and breast cancer-specific well-being in both racial/ethnic subgroups. These dimensions of QOL reflect common physical breast cancer symptoms and/or the severity of their effects on daily functioning.
Among non-Hispanic White women, greater cancer-specific distress and mood disturbance were both associated with poorer emotional well-being, while neither of these associations were observed in the African American subsample. It may be that African American patients utilized coping strategies or had social support resources that buffered the effects of distress and mood on their emotional well-being. African Americans are more likely to report using spirituality to cope with cancer-related emotions (Culver et al., 2002; True et al., 2005). In turn, spirituality is associated with decreased distress and increased emotional well-being in the cancer context (Leak et al., 2008). African Americans also effectively utilize social support and optimism in the face of cancer distress, which may protect against the loss of emotional QOL (Shelby et al., 2008). It is also possible that our measures of distress and emotional well-being did not have sufficient cultural sensitivity to adequately measure distress experienced by African American women in our region. Thus, phrases like “nervousness,” “losing hope,” and “fear of dying” on the emotional well-being subscale of the FACT-B may have been less frequently endorsed by our African American subsample. If this was the case, our findings might also be explained by restricted variance on both the predictors and outcomes.
African American women with higher mood disturbance reported significantly poorer social and family well-being, while their non-Hispanic White counterparts did not. African American breast cancer survivors generally experience greater role limitations than non-Hispanic White survivors (Paskett et al., 2008). The strain that disease puts on QOL may be alleviated by a supportive partner, especially among patients with lower education or material wealth (Krupski et al., 2006). Data from our sample suggest that women in our African American subsample may have been more likely to be single and never married (26% vs 6%), widowed (24% vs 12%), and less likely to be living in a nuclear family with a partner and children (0% vs 21%). Indeed, a higher proportion reported living as a single parent with children only (29% vs 15%) and had more than double the number of children living in the home compared with the non-Hispanic White subsample (1.53 vs 0.67 children). Thus, our African American women were more often serving in their homes as sole parents and/or caregivers (31.6% vs 15.2% of non-Hispanic Whites lived with children and no partner). Single parents and caregivers would have likely felt greater concern regarding the impact of cancer on their families (Ashing-Giwa et al., 2004), the burden of which could have been manifest in lower QOL ratings.
Research has shown that marital status may play an important role in medical (i.e. survival; Goodwin et al., 1987; Osborne et al., 2005) and psychological (i.e. QOL; King et al., 2000) cancer outcomes. However, given that marital status may be seen as a stressor or ameliorative factor for an individual, marital satisfaction may provide a better understanding of the role that marriage plays in relation to outcomes among individuals with cancer. Additionally, living situation is another factor that may shed light on the possible ameliorative role of social support within the home for individuals experiencing cancer, particularly in samples like ours, where there are many diverse family systems living in the home, therefore lending to different possibilities for sources of support within the home.
Additionally, education and financial resources influence the QOL of single African American mothers (Ensminger, 1995). As compared to the non-Hispanic White subsample, women in our African American subsample reported lower education and lower income (Table 1). Thus, African American women in our sample were potentially carrying more family responsibility while having fewer resources. In support, previous research has shown that for African American women with cancer, fear regarding the impact of the disease on family members is particularly salient (Ashing-Giwa et al., 2004). Family context is important to consider in future studies. Furthermore, nuance in QOL and well-being across ethnicities highlight the need for the use of culturally sensitive instruments in cancer research.
Our sample allowed for the investigation of two questions that have been unanswered among presurgical breast cancer patients: the impact of psychological and physiological stress on QOL and potential ethnic differences in these associations. Identification of factors related to QOL early in the course of the disease and treatment will inform intervention design. Nevertheless, the data from this study have limited applicability to patients who have already received neo-adjuvant, surgical, or adjuvant treatment, or to breast cancer survivors. Given the high incidence of breast cancer in African Americans, research in ethnically diverse populations is crucial to inform our understanding of psychological and physiological disturbances that may affect both the quality and quantity of patients’ lives. For women of different ethnicities, QOL may be affected by different factors over the course of disease. Additionally, limitations of the study include the small sample size and high number of statistical comparisons required for this multifaceted approach. The intent of this work is to generate hypotheses for further study and not to claim any definitive proof of hypothesized relationships. In light of these limitations, we limited secondary analyses only to those relationships that proved significant in preliminary analyses. In addition, primary analyses were limited only to the use of total scale scores, rather than subscale scores, for all psychometric variables.
Taken together with the existing literature, our findings suggest that physiological effects of stressors related to cancer may accumulate over time, leading to eventual disruption of circadian, endocrine, and immune function that becomes relevant to progression and QOL later in the treatment or survivorship trajectory (Eismann et al., 2010; McEwen and Seeman, 1999). Although there is a growing body of evidence of biological mechanisms involved in bidirectional links between mood and chronic medical illnesses (Eismann et al., 2010), our sample may not have had their disease long enough for poor mood to translate into physiological dysregulation (Spiegel and Giese-Davis, 2003). However, the strength and consistency of links we observed between distress/mood and QOL highlight a need for culturally sensitive clinical interventions to enhance adjustment among presurgical cancer patients.
Our findings illuminate a need for cultural sensitivity in psycho-oncology research generally, not only in the construct of our measures but also in their interpretation. QOL throughout the disease trajectory is crucial to the patient, and early adjustment to cancer predicts symptom severity later on. Studying the QOL of presurgical patients is important for understanding the psychological trajectory of coping, well-being, and potential downstream physiological effects. Given the potential benefits of psychosocial intervention during early disease stages, a research-based understanding of stress-health relationships among these patients is needed. Moreover, only a few studies have described ethnic and socioeconomic determinants of stress-health relationships, and it seems important to reconsider cultural context as we seek to understand what factors contribute to QOL. Longitudinal data should be collected to elucidate how changes in physiology—including circadian rhythms, sleep, cortisol rhythms, and serum parameters—may relate to QOL over time. The results of this research will assist with development of targeted therapies and interventions, improving the psychological symptoms and QOL of patients throughout the cancer journey.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Developmental Cancer Research Award, awarded to authors F.S.D., S.E.S., and D.S. from the Stanford Cancer Institute, Standford University School of Medicine, Stanford, CA; University of Louisville Intramural Research Incentive Grant for Research on Women awarded to S.E.S. from the University of Louisville Office of the Vice President for Research; Carl & Elizabeth Naumann Startup Fund awarded to F.S.D.