
Abstract
We examined the relationship between recognition of a 3-kg weight gain in 1 year with metabolic syndrome parameters and lifestyle status related to metabolic syndrome or cardiovascular disease in Japanese workers. Data were collected twice between April 2009 and March 2011, and self-reported questionnaires were completed at a follow-up by 275 workers who gained more than 3 kg in 1 year. This study showed that ~40 per cent of those who gained more than 3 kg in a year did not recognise their weight gain, and a weight gain over 3 kg was associated with worse metabolic syndrome parameters regardless of weight gain recognition.
Introduction
Metabolic syndrome (MetS) is a major risk factor for cardiovascular disease (CVD; Mottillo et al., 2010; Ninomiya et al., 2007). Mortality from CVD is high in Japan, accounting for about 10 per cent of the total number of deaths per year (Ministry of Health Labour and Welfare (MHLW), 2014). In Japan, MetS is defined by the presence of central obesity plus two of the following four factors: high triglycerides (TG), reduced high-density lipoprotein cholesterol (HDL-C), high blood pressure and high fasting blood glucose (FBG) (Committee to Evaluate Diagnostic Standards for Metabolic Syndrome, 2005). Preventing the development of MetS and controlling metabolic abnormalities are important issues today. However, according to the National Health and Nutrition Survey in 2011, in Japan, more than 50 per cent men and about 20 per cent of women 40–74 years old are suspected to have MetS or preliminary MetS (MHLW, 2011).
To improve this situation, the ‘Specific Health Check-up and Specific Counseling Guidance’ programme began in April 2008 (MHLW, 2007). Through this programme, all Japanese medical insurers are obligated to cover annual health checks for people over the age of 40 years. If they are at high risk of non-communicable diseases, specialists such as doctors and dieticians support them in reviewing their lifestyle in a specific counselling guidance session. The check-up includes measurements of weight, height, abdominal circumference (AC), blood pressure and a blood analysis, along with a standardised self-reported questionnaire. The questionnaire asks whether the subject had a change in body weight greater than 3 kg over the last year. From this question and the measured weight, we are able to assess whether the person’s recognition of their weight change was correct, and use the answer for specific guidance.
In a previous study (Toga et al., 2014), we examined the accuracy of respondents’ weight change perceptions and found that 29.2 per cent of people did not recognise a weight change of more than 3 kg. Generally, the more weight people gain, the higher the risk of various diseases (Bot et al., 2010; Chang et al., 2013; Saito et al., 2011). However, in other studies, it was shown that even a small weight gain increased the risk of disease (Kataja-Tuomola et al., 2010; Toga et al., 2016). We explored the relationship between weight gain and changes in MetS parameters over the course of 1 year among Japanese workers. Longitudinal data analysis revealed that certain MetS parameters were negatively affected by weight gain, even when it was a small weight gain of ~1.00 kg. For example, AC changes were 0.60, 1.55, 2.86 and 4.42 cm in those who gained 0–0.99 kg (the reference group), those who gained 1.00–1.99 kg, those who gained 2.00–2.99 kg and those who gained over 3.00 kg, respectively; the differences between the reference group and all other groups were significant. Similarly, TG levels increased gaining over 3.00 kg, and blood pressure increased (only in males) when the weight gain was over 2.00 kg (Toga et al., 2016).
However, it is unclear whether there are actually trends in MetS parameter changes with personal recognition of a 3-kg weight gain, even though this is used as a criterion in the Japanese Specific Check-up. Furthermore, it is possible that those who recognise their weight change lead more healthy lifestyles than those who did not, as the former group may pay more attention to their health in general, but this assertion has not been empirically supported.
Thus, in this study, we examined the relationship between a 3-kg weight gain in 1 year and changes in MetS parameters and compared trends in MetS parameter changes between those who recognised their weight gain and those who did not. Moreover, we also compared lifestyle variables that are said to have some relationship with MetS or CVD.
Materials and methods
Subjects
This study used longitudinal data from 3802 participants (1840 men, 1962 women) aged 23–62 years at baseline (Figure 1). The data were obtained from a check-up called the Specific Health Check-up (MHLW, 2007), which was conducted twice by a health insurance society at a large financial firm, once between April 2009 and March 2010 as baseline, and again between April 2010 and March 2011 as the 1-year follow-up, across the firms’ Japanese offices (27 prefectural and city governments).
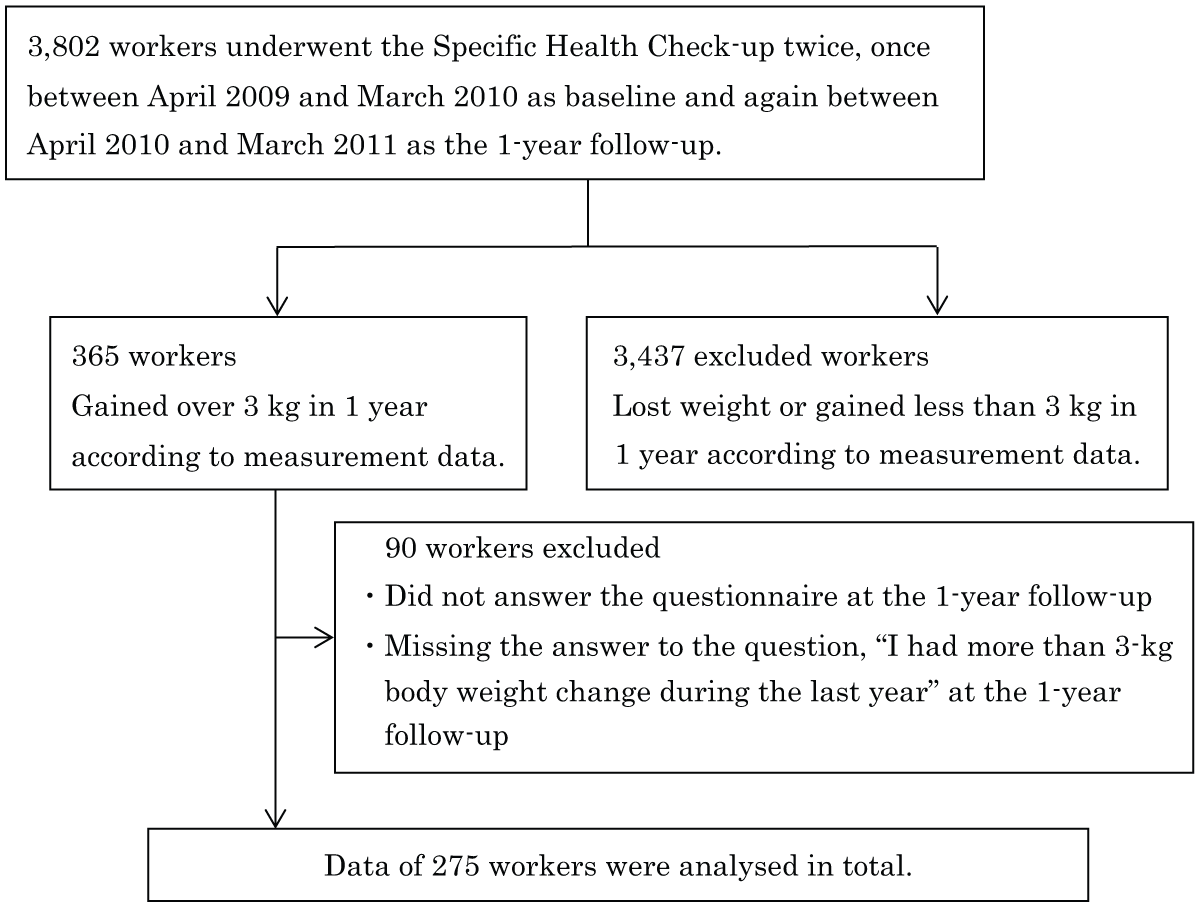
Flow chart of analysed participants.
To focus on those who had a higher risk of disease, 365 workers who gained more than 3 kg in the year between the baseline and the follow-up were included in the study population (9.6% of the overall population). For the analysis, workers who did not answer the questionnaire or who were missing answers to the question ‘I had more than 3-kg body weight change during this year’ at the 1-year follow-up were excluded. Finally, data for 275 workers were analysed (response rate, 75.3%). This study was approved by the Ochanomizu University Ethics Review Committee (No. 24-16).
Demographic characteristics
We used gender and age in the statistical analyses.
Anthropometric measures
We used body weight and height in the analyses. Height was measured with a stadiometer, and weight was measured with a calibrated scale. Body mass index (BMI) was calculated from height and weight (kg/m2).
Inspection results
In addition to the anthropometric measures, we used six items that were checked at both baseline and follow-up during the Specific Medical Check-up: AC, diastolic blood pressure (DBP), systolic arterial pressure (SAP), FBG (in Japan, the term generally means plasma glucose; The Japan Diabetes Society, 2012), TG and HDL-C. These six measurements are used as criteria for MetS in Japan (Committee to Evaluate Diagnostic Standards for Metabolic Syndrome, 2005). The measurements were determined according to the methods of the Standard Health Check-up and Health Instruction Program (MHLW, 2007).
Definition of self-reported body weight change
This item was included in the standardised self-reported questionnaire that was completed at the Specific Health Check-up (MHLW, 2007) during the 1-year follow-up. Workers responded ‘yes’ or ‘no’ to the item ‘I had more than 3-kg body weight change this year’. Participants were asked about their weight gain and loss in one question, as the questions are standardised by the government. However, we selected those study participants who had gained more than 3 kg in 1 year. Those patients who answered ‘yes’ and recognised their weight gain accurately were defined as the ‘accurate’ group, and the others as the ‘inaccurate’ group.
Definition of lifestyle status at follow-up
From the standardised self-reported questionnaire taken 1 year later, the following six lifestyle issues related to MetS or CVD were selected for this study based on evidence from previous studies: smoking (Higashiyama et al., 2009), regular exercise (Ikeda et al., 2012; Leitzmann et al., 2007), physical activity (Ikeda et al., 2012; Leitzmann et al., 2007), skipping breakfast (Cahill et al., 2013), speed of eating (Otsuka et al., 2008) and frequency of alcohol consumption (Ikehara et al., 2008). To determine the pattern of lifestyle status at follow-up, each healthy behaviour was first defined as follows: smoking – not smoking recently; regular exercise – intensive/sweat-inducing exercise ⩾30 minutes at a time and ⩾2 times/week; physical activity – walking or equal strength physical activity at least 1 hour/day; skipping breakfast – skipping breakfast <3 times/week; speed of eating – not eating rapidly compared with others; frequency of alcohol consumption – not drinking every day. Those who met the health behaviour criteria were defined as the ‘met’ group, and the others as the ‘unmet’ group.
Statistical analyses
To compare baseline characteristics and lifestyle status, the χ2 test was used for categorical variables and the t-test for consecutive variables. A two-way repeated-measures analysis of variance (ANOVA) was used to examine measured change values in body weight, BMI and MetS parameters from baseline to follow-up between the accurate and inaccurate groups (time × group). We analysed each gender separately due to a significant difference in number. Data were analysed using the SPSS software (ver. 19 for Windows; SPSS Institute, IBM, Japan). All tests were two tailed, and p-values < 0.05 were considered to indicate statistical significance.
Results
Subject characteristics
At baseline, the mean age of all subjects (n = 275) was 40.0 years (standard deviation (SD) = 7.9 years), and 154 subjects (56.0%) were men. There were 167 workers (60.7%, 84 men and 83 women) who answered that they had gained more than 3 kg of weight in 1 year by a self-reported questionnaire at the 1-year follow-up (the ‘accurate’ group), and 108 workers (39.3%, 70 men and 38 women) who answered they had not (the ‘inaccurate’ group). The inaccurate group had a significantly higher percentage of men than the accurate group (p = 0.018). In the men, the mean ages were 39.9 years (SD = 8.2 years) in the accurate group and 41.8 years (SD = 7.9 years) in the inaccurate group (n.s.); among women, the numbers were 38.9 years (SD = 7.2 years) and 39.3 years (SD = 8.5 years), respectively (n.s.).
Changes in MetS parameters in 1 year
To assess changes in mean body weight, BMI, AC, DBP, SAP, FBG, TG and HDL-C between baseline and follow-up and between the accurate and inaccurate groups, two-way repeated-measures ANOVA was used (Table 1). Among men, significant main effects for time (from baseline to follow-up) were seen in all measures (SAP: p = 0.002; HDL-C: p = 0.014; all others: p < 0.001). Thus, body weight, BMI, AC, DBP, SAP, FBG and TG increased over the year, but HDL-C decreased in both groups. A significant main effect for group was found only for HDL-C (p = 0.004), with the value higher in the inaccurate than in the accurate group at both baseline and follow-up. Significant interaction effects between baseline/follow-up and accurate/inaccurate were shown for body weight, BMI and AC (body weight: p = 0.001; BMI: p = 0.015; AC: p = 0.049), meaning that the changes in values from baseline to follow-up were not the same between the accurate and inaccurate groups. The increasing trends were stronger in the accurate group for body weight, BMI and AC, but the other parameters did not differ.
Mean values of body weight, BMI and MetS parameters per accurate or inaccurate groups at baseline and follow-up.
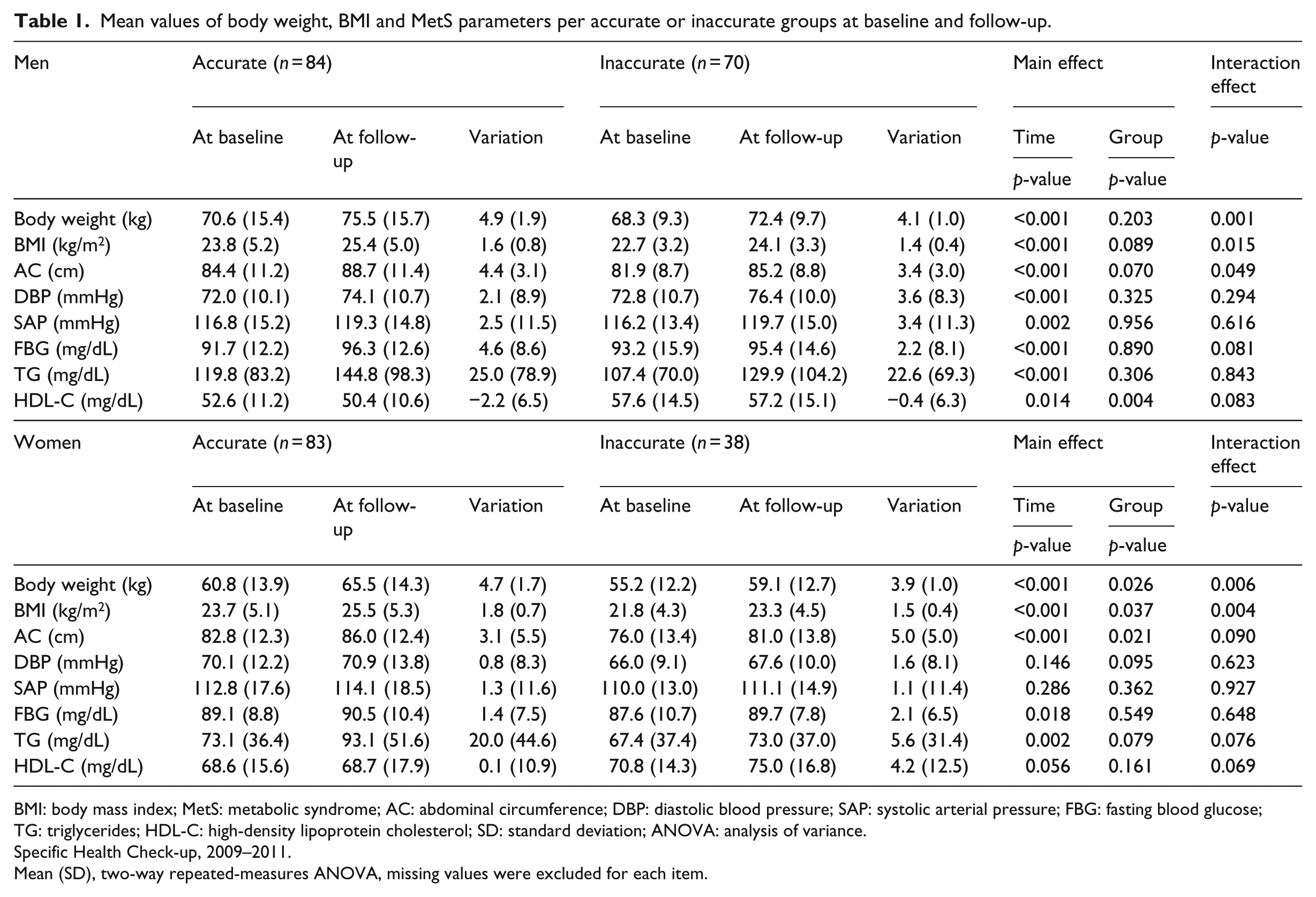
BMI: body mass index; MetS: metabolic syndrome; AC: abdominal circumference; DBP: diastolic blood pressure; SAP: systolic arterial pressure; FBG: fasting blood glucose; TG: triglycerides; HDL-C: high-density lipoprotein cholesterol; SD: standard deviation; ANOVA: analysis of variance.
Specific Health Check-up, 2009–2011.
Mean (SD), two-way repeated-measures ANOVA, missing values were excluded for each item.
Among women, significant main effects of time were seen for body weight, BMI, AC, FBG and TG (FBG: p = 0.018; TG: p = 0.002; all others: p < 0.001); all increased from baseline to follow-up. Significant main effects for group were found for body weight, BMI and AC (body weight: p = 0.026; BMI: p = 0.037; AC: p = 0.021), and those values were higher in the accurate group than the inaccurate group. Significant interaction effects between time and groups were shown only for body weight and BMI (body weight: p = 0.006; BMI: p = 0.004); this result was similar to that in men.
Lifestyle status at follow-up
Furthermore, we examined the lifestyle status between the accurate and inaccurate groups (Table 2). There was a significant difference only in speed of eating among women. Thus, 42 (50.6%) subjects reported eating quickly in the accurate group, but only 12 (31.6%) in the inaccurate group (p = 0.039).
Number of individuals and lifestyle status in accurate and inaccurate groups at follow-up.
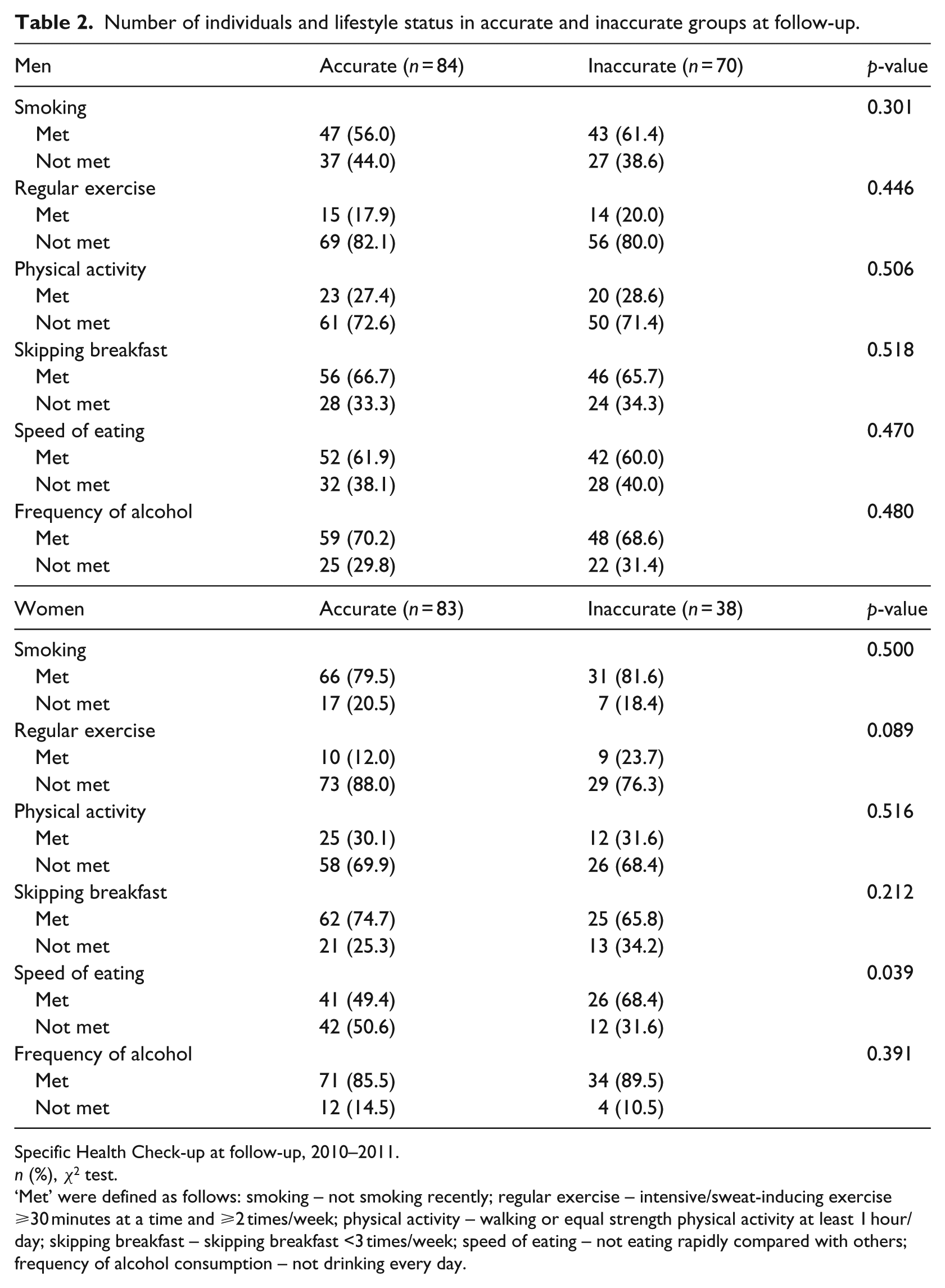
Specific Health Check-up at follow-up, 2010–2011.
n (%), χ2 test.
‘Met’ were defined as follows: smoking – not smoking recently; regular exercise – intensive/sweat-inducing exercise ⩾30 minutes at a time and ⩾2 times/week; physical activity – walking or equal strength physical activity at least 1 hour/day; skipping breakfast – skipping breakfast <3 times/week; speed of eating – not eating rapidly compared with others; frequency of alcohol consumption – not drinking every day.
Discussion
In this study, we examined the relationship between a 3-kg weight gain over 1 year and changes in MetS parameters. Furthermore, we compared trends in MetS parameters and lifestyle status between those who recognised their weight gain and those who did not. Longitudinal data analysis revealed that ~40 per cent of people did not recognise their weight gain of more than 3 kg; however, the change trends in MetS parameters were similar regardless of weight gain recognition. Furthermore, the tendencies in almost all lifestyle behaviours were similar in the two groups.
It was reported that 73 per cent of those who gained more than 3 kg in 6 months were aware of their weight gain (Rahman and Berenson, 2012). In our study, 60.7 per cent of those with weight gain recognised their weight gain, and the rest did not. Thus, to determine weight changes accurately, we have to use scales in addition to self-reported values.
Furthermore, in this study, most of the medical measures worsened similarly, regardless of the patients’ weight gain recognition. There seems to be a high probability that those who did not recognise their weight gain would also not realise their poor physical condition until MetS had developed because they may have a less developed sense of their own health. Thus, it is important to encourage people to constantly measure their weight independently so that they become aware of any weight gain at an early stage. In addition, during the specific guidance, specialists such as dieticians and doctors need to check weight change using scales to help prevent MetS development.
Furthermore, the speed of eating was the only lifestyle factor that differed between those who recognised their weight gain and those who did not among women. Previous studies have found that people who eat quickly tend to have higher BMIs (Otsuka et al., 2008). In our study, women who recognised their weight gain accurately tended to eat faster and had higher BMIs than those who did not recognise their weight gain. This study generally showed results consistent with those reports.
This study has some limitations. First, we did not consider weight fluctuation within the year. It is possible that a pattern of extreme weight gain and loss within a year is related to the observed changes in MetS parameters, but we did not include those who gained more than 3 kg but then lost it before the 1-year follow-up. However, the question in the standardised self-reported questionnaire that asked whether there was a weight change of more than 3 kg over the year sought to determine the quantity of weight change 1 year later, not weight fluctuation within a year (MHLW, 2007). Therefore, in this study, we followed that intent. Second, we could not examine changes in lifestyles. We tried to examine the relationship between the accuracy of weight gain and changes in lifestyle from baseline to follow-up, but the sample size was too small. However, when we examined lifestyle at follow-up instead, we discovered that recognition of weight gain was related to the speed of eating in women.
This study showed that weight gain of more than 3 kg affected MetS parameters regardless of participants’ recognition of their weight gain. While providing specific guidance to these patients, specialists need to check weight changes using scales to help prevent the development of MetS. In future studies, factors that promote self-weighing to raise patients’ recognition of their weight change and the creation of environments where it is easy to check the state of their health should be examined.
Conclusion
This is the first reported study to examine the relationship between 3-kg weight gain and changes in MetS parameters in 1 year and to compare trends in MetS parameter change according to lifestyle status between those who recognised their weight gain and those who did not. This study revealed that ~40 per cent of subjects did not recognise their more than 3-kg weight gain. However, the change trends in the MetS parameters were similar regardless of their recognition of their weight gain. Furthermore, there were similar tendencies in almost all lifestyle behaviours in both groups. To help prevent the development of MetS and to control metabolic abnormalities, checking 1-year weight change is useful, and it should be done using scales rather than relying on patient-reported values.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.