
Abstract
Binge drinking represents a major clinical and public health concern. Here, we investigated the prevalence of binge drinking and its related consequences, in a population of young adults. A questionnaire was administered to a sample of 4275 healthy subjects. In the overall sample, the percentage of binge drinkers was 67.6 per cent; among regular alcohol users, 79.5 per cent reported episodes of binge drinking. Among binge drinkers, several serious consequences were identified (staggering and stuttering, amnesia, loss of control, aggressiveness, sexual disinhibition). Raising awareness about the seriousness of binge drinking may help health care providers to identify cases early on and provide appropriate treatments.
Introduction
The consumption of alcoholic beverages is considered in Italy, as well as in many Western countries, as part of social life (De Bruijn et al., 2016). However, excessive consumption and the introduction of new patterns of alcohol use have changed this tradition dramatically, increasing alcohol-related risks in both personal and social development (Bryan et al., 2015; Kuntsche et al., 2004). The globalization of alcohol consumption styles has led to the diffusion of habits, such as binge drinking, previously more common in the United States and in Northern Europe (World Health Organization (WHO), 2013). Binge drinking results in immediate intoxication and loss of control and very often involves young populations (Chainey and Stephens, 2016; Furtwängler and de Visser, 2016; Standridge et al., 2004).
Binge drinking is defined as the consumption of five or more drinks in men, or four or more drinks in women, in a single episode at least once during the past 2 weeks (Wechsler and Nelson, 2001). The National Institute on Alcohol Abuse and Alcoholism (NIAAA) identifies binge drinking as a pattern of drinking that brings blood alcohol concentration (BAC) to 0.08 g per cent or above. This typically takes place after four or five drinks (for women or men, respectively) in a 2-hour period (NIAAA, 2004).
Research conducted in the European Union highlighted the frequency of binge drinking behaviours in those countries: the highest rates were recorded in Ireland (44%), Romania (39%), Germany and Austria (both 36%), United Kingdom, Spain and Greece (34%) and Italy (30%). This study also indicated that binge drinking episodes were more frequent in men than women (36% vs 19%, respectively) (Eurobarometer, 2010). This is consistent with data from the WHO, indicating that binge drinking is very common among young males (18–26 years old) (WHO, 2013). According to the data from the National Institute for Statistics (ISTAT), in Italy, the phenomenon involves 23 per cent of men and 8.6 per cent of women; the most affected age group ranges from 18 to 24 years old (Bartoli et al., 2014; Chillemi et al., 2015; ISTAT, 2014; Martinotti et al., 2014b).
The major consequences of binge drinking are common to other addictive substances as well. Intoxicated driving, in addition to causing harm to the drinker, puts others at great risk (Kuntsche et al., 2004). Drinking may influence mood and cognitive performance; indeed, both long- and short-term memory may be impaired (Hatzigiakoumis et al., 2011; Wen et al., 2012). Confusion and reduced attention may affect school and work performance, as well as difficulties performing simple daily tasks (Gil-Hernandez and Garcia-Moreno, 2016). Finally, long-term physical consequences include neurological, cardiac, gastrointestinal, haematological, immune, endocrine and musculoskeletal alterations (Foxcroft et al., 2014; Jacobus and Tapert, 2013).
In this study, we investigated the patterns of binge drinking, and its related consequences associated with social harm and disease burden, in a population of young Italian adults. The aim of our research was to gain more information about the main motivations and the environmental and socio-cultural factors that underpin these behaviours with a particular focus on the potential risks of alcoholic bingeing.
Methods
Sample
A questionnaire was administered to a sample of 4275 healthy subjects (43.9% males; 56.1% females), aged 18–26 years (mean age: 22.04 years; standard deviation (SD): 2.52 years), residing in different Italian cities located in the north, centre and south of the country. This was done in order to ensure the inclusion of youths from diverse social contexts. The snowball sampling procedure was followed for the selection of the sample; specifically, stakeholders were approached, asked for contacts and gained contacts were asked to participate (Goodman, 1961).
Measure
We developed a self-administered questionnaire, consisting of 17 items, which investigated socio-economic characteristics (age, gender, residence, job status and living status), alcohol use with a specific focus on binge drinking, ‘classic’ substances use (tobacco, caffeine, cannabis, cocaine, heroin, etc.) and novel psychoactive substances (NPS) use. The questionnaire also addressed the most common consequences of binge drinking, that is, loss of control (not being master of oneself), stuttering and staggering, loss of consciousness (fainting), hospitalization, aggressiveness, sexual disinhibition (improper sexual behaviour), amnesia (global and transient episodes of ‘blackout’) and the use of medications the following day. All the participants were asked the following question: ‘do you drink alcohol?’ (Yes/No); if yes, ‘how often do you drink alcohol?’ (less than once a week, once a week, two to three times a week, every day). The binge drinking item has been defined by consumption of 4 or 5 drinks (for women or men, respectively) in a single episode and in a 2-hour period (Wechsler & Nelson, 2001; NIAAA, 2004).
Procedure
The data were collected between January 2014 and April 2015 by our team of psychologists and psychiatrists, with support of a peer-working group. The data were collected anonymously and confidentiality was maintained. Interviewers obtained informed consent from all respondents, in accordance with the Declaration of Helsinki. The study was approved by local ethics committees and institutional review boards.
Statistical analysis
The baseline data were analysed using descriptive statistics, including means and SDs, frequencies and percentages. The chi-square test of independence of categorical variables and correlational analysis using phi coefficient (ϕ) adjusted for age and gender as potentials confounder were used for comparisons of quantitative data. SPSS version 22.0 was used for all analyses.
We considered as salient only absolute correlations equal to or greater than 25, which explain 6–9 per cent or more of the variance, as the probability value is influenced by the number of subjects in the sample (Kline, 2000).
Results
Socio-demographic data indicated that 60.8 per cent of the subjects were students, 12.3 per cent working students, 17.8 per cent workers and 9.1 per cent unemployed. In addition, 68.9 per cent of the respondents lived with parents, 19.1 per cent with friends, 8.0 per cent alone and 3.9 per cent with a partner.
A total of 53.3 per cent of the subjects were tobacco smokers, with an average of 10.69 (SD: 7.04) cigarettes smoked per day, while 84.8 per cent of the respondents consumed coffee, with an average of 3.06 (SD: 1.80) cups of coffee per day.
A total of 80.9 per cent of the total sample reported drinking alcohol regularly. Within this group, females were more prevalent than males (52.6% vs 47.4%, respectively; p < .001). The frequency of alcoholic beverage consumption was less than once a week for 30.4 per cent of the subjects, 33.6 per cent drank alcohol once a week, 27.8 per cent two to three times a week and 8.2 per cent almost every day. A total of 58.2 per cent of the sample consumed 1–2 standard drinking units (SDUs) per drinking session, 27.3 per cent drank 3–4 SDUs, 9.2 per cent 5–6 SDUs, 3.2 per cent 7–8 SDUs and finally 2.1 per cent had 9 or more SDUs (1 SDU corresponds to a drink containing 12 g of ethanol; National Institute of Research on Food and Nutrition (INRAN, 2003).
Among regular alcohol users, 79.5 per cent had binge drinking habits, while among non-regular alcohol users 13.3 per cent of subjects presented occasional binge drinking behaviours. In the overall sample, the percentage of binge drinkers was 67.6 per cent, with a statistically significant predominance of males over females (52.0% vs 48.0%, respectively; p < .001). Among binge drinkers, 1.9 per cent binge drank every day, 12.0 per cent two to three times a week, 18.8 per cent once a week and 67.3 per cent less than once a week.
Among the binge drinkers population, 97.8 per cent consumed alcohol with friends; after a heavy drinking session, 49.3 per cent reported having lost control, while 81.7 per cent had staggered and stuttered, 12.4 per cent had lost consciousness, 5 per cent had been hospitalized, 28.6 per cent had episodes of aggressiveness, 45 per cent were sexually uninhibited, 50.5 per cent had amnesia and 24.2 per cent took medications the following day.
Men lost control significantly more frequently than women (p < .001); they also were more often hospitalized (p < .001), aggressive (p < .001) and sexually disinhibited (p < .001). Women more frequently took medications the day after a heavy drinking session (p < .001). The data are summarized in Table 1.
Binge drinking consequences: gender differences.
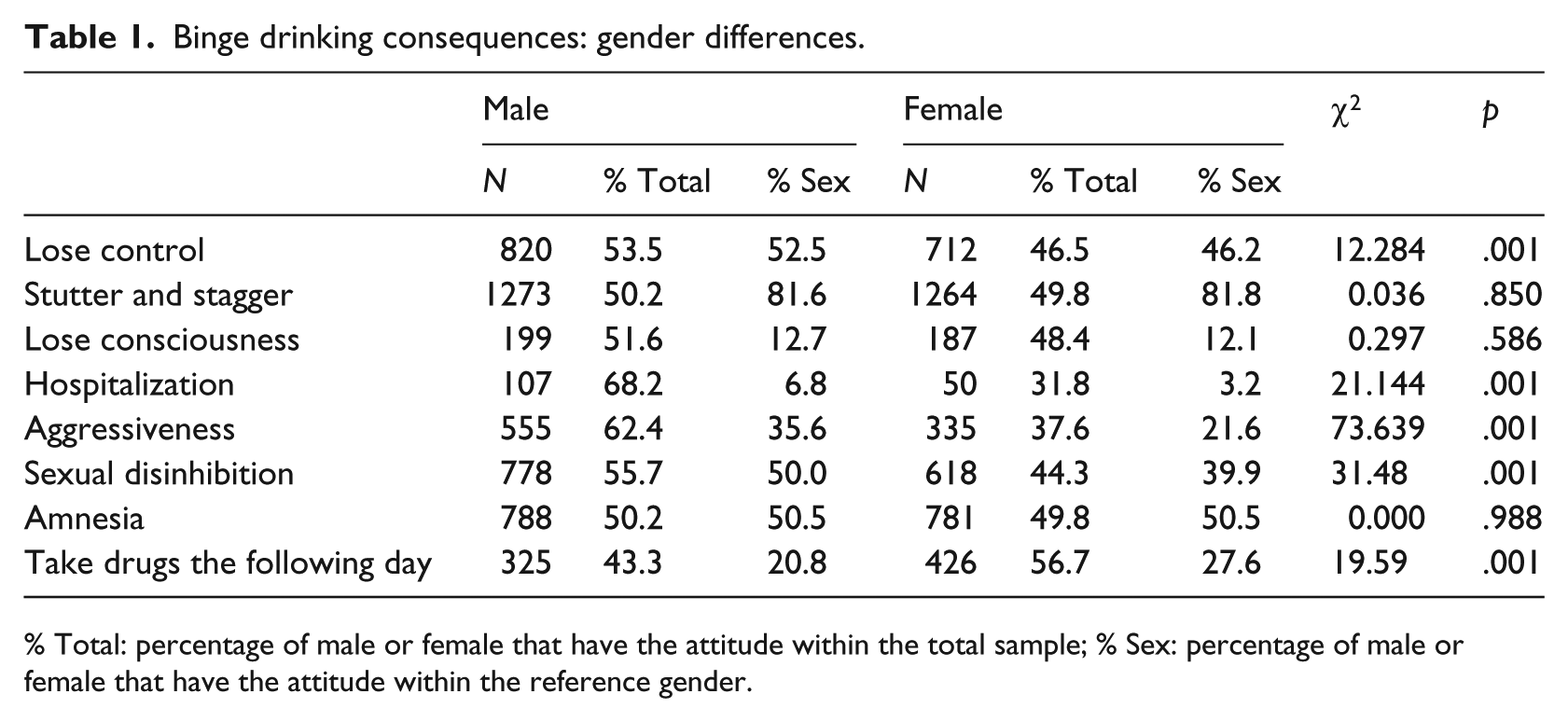
% Total: percentage of male or female that have the attitude within the total sample; % Sex: percentage of male or female that have the attitude within the reference gender.
The use of more than one substance in the same night (polyabuse) was reported by 38.2 per cent of the total sample, with a statistically significant predominance of males over females (58.3% vs 41.7%, respectively; p < .001). Among this group, 6.7 per cent used more than three substances during the same night. Besides alcohol, the most used substances were cannabinoids (84.7%), cocaine (6.5%) and 3,4 methylenedioxymethamphetamine (MDMA) (2.1%). Considering the overall sample, 28.5 per cent reported use of cannabis, 4.5 per cent of subjects reported using cocaine and 3.2 per cent reported using NPS.
Moreover, we performed correlational analysis among binge drinking behaviours and habitual alcohol consumption, polyabuse, tobacco smoking, cannabinoids, cocaine and NPS use. Among the significant correlations considered salient were those between binge drinking behaviours and habitual alcohol consumption; tobacco smoking and cannabinoids use; habitual alcohol consumption and tobacco smoking; polyabuse and tobacco smoking, cannabinoids use and cocaine habit; tobacco smoking and cannabinoids use; cannabinoids use and cocaine habit; cocaine habit and NPS use. The data are summarized in Table 2.
Correlational analysis.

NPS: novel psychoactive substances.
N = 4275.
p < .01.
Discussion
Our survey-based study indicated a 67.6 per cent prevalence of binge drinking behaviour in a general relatively large sample. This prevalence, although the term binge, its measurement and its utility are currently under scrutiny (Pearson et al., 2016), is higher compared to previous European and Italian studies conducted with similar populations (Bartoli et al., 2014; Eurobarometer, 2010; Soler-Vila et al., 2014; Tavolacci et al., 2013). On the other hand, two other studies previously reported a prevalence similar to that reported here: a study performed in the United States with 20,138 subjects indicated a prevalence estimate of binge drinking of 63.6 per cent (Cranford et al., 2006), and in a European study binge drinking ranged between 50 per cent and 72 per cent (Plant et al., 2010). Similarly, a recent Korean study on a sample of college students highlighted that 93 per cent of the respondents drank alcohol at least once during the month before the survey, and 72.2 per cent were problem drinkers, who engaged in binge drinking on average 4.5 times during the previous month (Kim and Park, 2015).
Our study identified several serious consequences due to binge drinking, among which the most frequent were staggering and stuttering (81.7%), amnesia (50.5%), loss of control (49.3%), sexual disinhibition (45%) and aggressiveness (28.6%). We also found significant gender-related differences. In fact, loss of control, hospitalization, aggressiveness and sexual disinhibition were more common among males, while taking medication the day after a heavy drinking session was more common in females. These data on alcohol intoxication are relevant and consistent with previous work on the consequences of binge drinking, such as cognitive impairment and loss of control (Miller et al., 2009; Rose and Duka, 2007). For instance, binge alcohol consumption, especially in peer group contexts (e.g. ‘spring break’ holidays), is strictly related to situational sexual disinhibition and casual sex, which, in turn, increases the risk of sexually transmitted diseases (Apostolopoulos et al., 2002). Binge drinking has also been identified in male college students as a risk factor for sexual aggression perpetration, impulsivity and hostility towards women (Kingree and Thompson, 2015), and in females of similar age it has been related to an increased lifetime risk of experiencing an incapacitated rape (McCauley et al., 2010).
Our sample presented a relevant prevalence of memory impairment after binge drinking (50.5%). Previous studies assessed cognitive function in alcohol abusers and found deficits in both frontal lobe and working memory, suggesting that the frequent consumption of high quantities of alcohol may induce long-term memory issues (Tapert et al., 2001). In addition, in animals, exposure to binge drinking leads to neurodegeneration in corticolimbic areas related to learning and space memory, such as the olfactory bulb, the piriform cortex, the entorhinal cortex and hippocampal dentate gyrus (Crews et al., 2000).
The rate of hospitalizations related to binge drinking in our sample was 5 per cent. The result is interesting given that, according to data released by the Italian National Institutes of Health, more than 25,000 deaths are caused by alcohol each year, and the number of diseases due to daily alcohol use, such as fatty liver disease or episodes of alcohol intoxication, is growing and involves very young patients (under 14 years of age). Additionally, 20 per cent of hospital admissions per year and 10 per cent of admissions in intensive care units are alcohol-related, as well as 35 per cent of liver transplants (ISTISAN, 2016).
Our study also shows that females drink more than males. This result contradicts most of the data indicating higher alcohol consumption in males (Eurobarometer, 2010; WHO, 2013). According to the data from the last European School Survey Project on Alcohol and Other Drugs (ESPAD) survey of European high-school students, while boys, compared to girls, report higher alcohol consumption on their most recent drinking day in most countries, the amount of alcohol consumed was about the same in both males and females in Iceland and Sweden (ESPAD, 2012). This may suggest that alcohol use in women, especially among the youngest generation, may become more widespread.
Correlational analysis indicated that polyabuse is also a diffuse phenomenon. This represents a serious public health challenge, and pharmacological, toxicological and psychopathological effects should be considered, given that the interactions among substances may be unpredictable and fatal in vulnerable individuals (Martinotti et al., 2009). Binge drinking is also a phenomenon commonly reported in the club scene, often characterized by a concurrent NPS polyabuse, as previously demonstrated by different studies (Bersani et al., 2014; Martinotti et al., 2014a, 2015; Vento et al., 2014). This new typology of polyabuse, associated with binge drinking, may further worsen the clinical presentation and its possible outcomes.
Our study has several limitations: (1) the questionnaire used in the study does not represent a validated instrument, able to deeply analyse the level of knowledge and the specific experiences reported by the subjects recruited; (2) standard criteria for the definition of ‘binge drinking’ that we used were recently criticized for lack of predictive validity, ecological bias and false dichotomization (Pearson et al., 2016); and (3) the snowball randomization procedure does not guarantee a strict distribution of the subjects. Although the snowballing recruitment method showed advantages, such as time, cost or when representation from diverse communities is needed (Sadler et al., 2010), it can overestimate the prevalence of a specific attitude and addictions, or unbalance samples with particular demographic characteristics (Magnani et al., 2005). In this way, the high prevalence of binge drinking in our study, compared with previous reports based on European populations, can be justified by the choice of recruiting a specific age range of 18–26 years (WHO, 2013); accordingly, the results of our study cannot be generalized to the whole populations. In spite of these limitations, our study provides additional evidence on the impact of binge drinking, not only on the health of the individual but also on social and work life. Notably, the term ‘social drinking’ refers to the use of 1 or 2 SDUs, typically consumed at meals and it is usually reported both in the common language and in the scientific literature (ESPAD, 2012). However, given the high diffusion of binge drinking, involving the majority of the subjects using alcohol, the label of social drinking might be changed, keeping in mind that this new pattern of alcohol use may lead to dramatic consequences, as shown by this and previous studies. Raising awareness about the seriousness of binge drinking may help health care providers to identify cases early on and provide appropriate treatments, as necessary.
Footnotes
Acknowledgements
The authors would like to thank the peer-working group (Corbo, Fiori, Chillemi, Bonifaci and Agresta, Astorino, Barone, Carenti, Caroprese, Carpineti, Cascetta, Cavallo, Costantini, D’Ascanio, De Falco, Di Schiena, Federico, Fina, Fonzo, Garofalo, Giancaterino, Grafone, Iezzi, Lorusso, Malagisi, Malpiede, Mangione, Marini Ricci, Marzo, Mercati, Parrella, Passiatore, Pecoriello, Pendenza and Petrillo), for their significant support with sample recruitment and data collection. The authors would also like to thank Ms Karen Smith, National Institutes of Health (NIH) Library, for bibliographic assistance. G.M. and M.L. contributed equally as first authors.
Author’s Note
Giovanni Martinotti and Matteo Lupi have participated equally in the research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: L.L. was supported by the National Institutes of Health intramural funding (grant #ZIA-AA000218, Section on Clinical Psychoneuroendocrinology and Neuropsychopharmacology; principal investigator (PI): L.L.) and jointly supported by the National Institute on Alcohol Abuse and Alcoholism Division of Intramural Clinical and Biological Research and the National Institute on Drug Abuse Intramural Research Program.