
Abstract
The purpose of this prospective cohort study was to investigate whether Type D personality was related to periodontal disease in Japanese university students. Among students (n = 600) who were interested in receiving oral health examinations, logistic regression analysis showed that the risk of developing periodontal disease during a 3-year period was associated with body mass index ⩾ 25 (odds ratio: 2.543; 95% confidence interval: 1.297–4.989; p = 0.007) and Type D personality (odds ratio: 1.473; 95% confidence interval: 1.027–2.111; p = 0.035). In this short-term prospective cohort study, a significant association between periodontal disease and Type D personality was observed in Japanese university students.
Introduction
Periodontal disease is one of the most widespread chronic diseases and is predominantly a bacterial infection involving the dental biofilm or dental plaque (Genco and Borgnakke, 2013). Numerous studies have investigated the risk of periodontal diseases and have provided evidence supporting the important role of risk factors of periodontal disease. The prevalent risk factors are being of male sex (Eke et al., 2012), smoking (Tonetti, 1998), diabetes (Simpson et al., 2010), obesity (Suvan et al., 2011), osteoporosis (Martinez-Maestre et al., 2010), psychological stress/psychiatric symptoms (Peruzzo et al., 2007), and genetic factors (Meng et al., 2011). In addition, behaviors such as coping stress (Wimmer et al., 2005) and oral health behavior (usage of dental floss or regular dental check-ups) (Mizutani et al., 2012) are related to periodontal disease. However, few studies have investigated the relationship between personality and periodontal disease.
Type D personality was established to describe individuals who exhibit both negative affectivity (NA) and social inhibition (SI) (Denollet, 2005). Individuals with high NA tend to experience undesired emotions such as anger, distress, hostility, and depression. Individuals with high SI tend to experience social difficulties because they hide their emotions in social interactions due to fear of rejection or disapproval from others. In recent years, Type D personality has been linked to a series of illnesses. Type D personality is associated with negative outcomes in various diseases such as Type 2 diabetes, irritable bowel syndrome, heart diseases, and coronary heart disease (Ginting et al., 2016; Nefs et al., 2012; Schiffer et al., 2010; Yildirim et al., 2013). The relationship between Type D personality and various psychological problems, including depression, anxiety, and posttraumatic stress disorder, has been investigated (Howard and Hughes, 2012; Kupper et al., 2007). Moreover, Type D personality is associated with work-related problems, such as job stress and burnout (Mommersteeg et al., 2012; Oginska-Bulik, 2006), and subjective health (Williams et al., 2016).
There are some studies about Type D personality and health behavior in healthy adults. Individuals with Type D personality exhibited an approximately four times increased risk of having sleep disturbances, and type D personality was associated with fewer sleeping hours (Condén et al., 2013). Type D individuals engaged in fewer health behaviors like eating a balanced diet and getting regular exercise and were less likely to get regular medical check-ups than non-Type D individuals (Williams et al., 2008). Type D personality was also associated with smoking, lack of physical activity, low levels of self-efficacy, maladaptive coping, and less healthy food intake (Booth and Williams, 2015; Gilmour and Williams, 2012; Wiencierz and Williams, 2017). Thus, Type D personality affects health behavior in even the young generation. Although periodontal health is critically dependent upon the oral health behaviors of the patient (Newton and Asimakopoulou, 2015), no studies have examined the relationship between Type D personality and oral health behaviors.
It is important to evaluate the relationship between Type D personality and periodontal disease in young adults as progression of periodontal disease, which is one of the major causes of tooth loss, was observed in university students (Mizutani et al., 2015). We hypothesized that Type D personality may predict onset of periodontal disease in young adults. The aim of this prospective cohort study was to explain the relationship between Type D personality and periodontal disease in university students.
Methods
Study population
Of the first-year students (n = 2297) who underwent both general and oral health examinations (pre-university) at the Health Service Center of Okayama University in April 2012, 692 students volunteered to receive a 3-year follow-up examination before graduation in April 2015 (follow-up rate: 30.1%). After excluding participants with incomplete data in their questionnaires (n = 44) and with periodontal disease at baseline (n = 48), data from 600 systemically healthy students (282 males, 318 females) aged 21.2 ± 0.6 years (range: 21–28 years) at follow-up were analyzed (Figure 1). The study was approved by the Ethics Committee of Okayama University. Verbal consent was obtained from all participants.

Flow chart of participants.
Type D personality
Type D personality was assessed using the 14-item Type D Personality Scale (DS14) (Denollet, 2005). The DS14 comprises two subscales: NA (7 items; range: 0–28) and SI (7 items; range: 0–28). Participants were asked to rate their responses on a 5-point Likert-type scale (from 0 = false to 4 = true). We defined participants with Type D personality as those with scores of greater than 10 on both subscales (i.e. NA and SI) (Denollet et al., 1996; Emons et al., 2007). Cronbach’s alpha was 0.88 for the NA and 0.86 for the SI, respectively, and test–retest reliability was 0.72 and 0.82 for the NA and SI, respectively, in the original DS14 (Denollet, 2005). In this study, Cronbach’s alpha observed was 0.891 for the NA subscale and 0.874 for the SI subscale. Moreover, the test–retest reliability was 0.827 for the NA subscale and 0.824 for the SI subscale in the preliminary study targeted at other university students (n = 38).
Oral examination
Three dentists (D.E., S.M., and T.A.) examined the oral health status of the participants. The number of teeth present was recorded. Periodontal condition was assessed using the community periodontal index (CPI) (Furuta et al., 2011). A total of 10 teeth were selected for periodontal examination: two molars in each posterior sextant, and the upper right and lower left central incisors. Measurements were made using a CPI probe (YDM, Tokyo, Japan) at six sites (mesio-buccal, mid-buccal, disto-buccal, disto-lingual, mid-lingual, and mesio-lingual) per tooth. The percentage of teeth exhibiting bleeding on probing (BOP) at least one site (%BOP: number of BOP-positive teeth per total number of teeth) was calculated. Since, BOP has been shown to be an earlier and more sensitive indicator of inflammation than visual signs of inflammation (redness and swelling) (Greenstein, 1984). Thus, we also assessed %BOP as an indicator of periodontal disease in this study (Furuta et al., 2011). Periodontal disease was defined using the following criteria: the presence of probing pocket depth (PPD) ⩾ 4 mm (CPI score = 3 or 4) and BOP ⩾ 30 percent (active periodontal pocket) (Kawabata et al., 2016). Good intra- and inter-examiner agreement was achieved for repeated PPD measurements in the 10 teeth used for CPI with Kappa statistic >0.8.
Body mass index
In the general health examination, the height and body weight of participants were measured by the University’s public health nurses using the Tanita body fat analyzer (Model No. BF-220; Tanita, Tokyo, Japan). Obesity was assessed on the basis of body mass index (BMI) (kg/m2) at four levels: <22.0, 22.0–24.9, 25.0–29.9, and ⩾30.0 (Ekuni et al., 2014; Morita et al., 2011).
Questionnaire
At baseline, participants filled out a self-administered questionnaire. In addition to gender, age (continuous), general health condition, and smoking status (current/never), the questionnaire also asked about the following items: (1) daily frequency of tooth brushing (⩽One time/⩾Two times), (2) use of dental floss (yes/no), and (3) visits to dental clinics for regular check-up (yes/no). The questionnaire also evaluated the change in oral health behaviors at the 3-year follow-up (Mizutani et al., 2015).
Statistical analysis
Cronbach’s alpha coefficient was used to examine the consistency of scales. Differences between the baseline and follow-up were evaluated with paired t-test or McNemar test, as appropriate. When the participants have periodontal disease after 3 years, they were defined as the subjects with onset of periodontal disease. First, we examined the association between Type D personality and oral health behaviors at baseline and after 3 years using chi-square test. Second, unpaired t-test and chi-square test were used to determine whether there were any significant differences between the participants with and without the onset of periodontal disease at re-examination. We used Fisher’s exact test when expected cells were found to be less than five. Multivariate logistic regression was used to calculate odds ratios (ORs) and 95 percent confidence intervals (CIs) after controlling simultaneously for potential confounders. The onset of periodontal disease was used as the dependent variable. Independent variables were selected when the p value was <0.20 for the chi-square test or unpaired t-test in each variable. Since there were only two students who had BMI ⩾ 30, we combined two categories (BMI ⩾ 30 and 25.0–29.9) into one (BMI ⩾ 25.0). Results of logistic regression analyses were considered statistically significant when p < 0.05. We evaluated the predictive performance of the model by assessing its discrimination (ability to classify correctly), and assessed the model fit using the Hosmer–Lemeshow goodness-of-fit test for logistic regression. We conducted all analyses using SPSS version 22.0 (IBM, Tokyo, Japan).
Results
The characteristics of the 600 participants at baseline and after 3 years are shown in Table 1. The number of participants with onset of periodontal disease was 186 (31.0%) during 3 years. Although the percentage of participants who use dental floss increased during 3 years (p < 0.001), regular dental check-up and smoking state turned worse (p = 0.042 and p < 0.001, respectively) (Table 1).
Participant characteristics (N = 600).
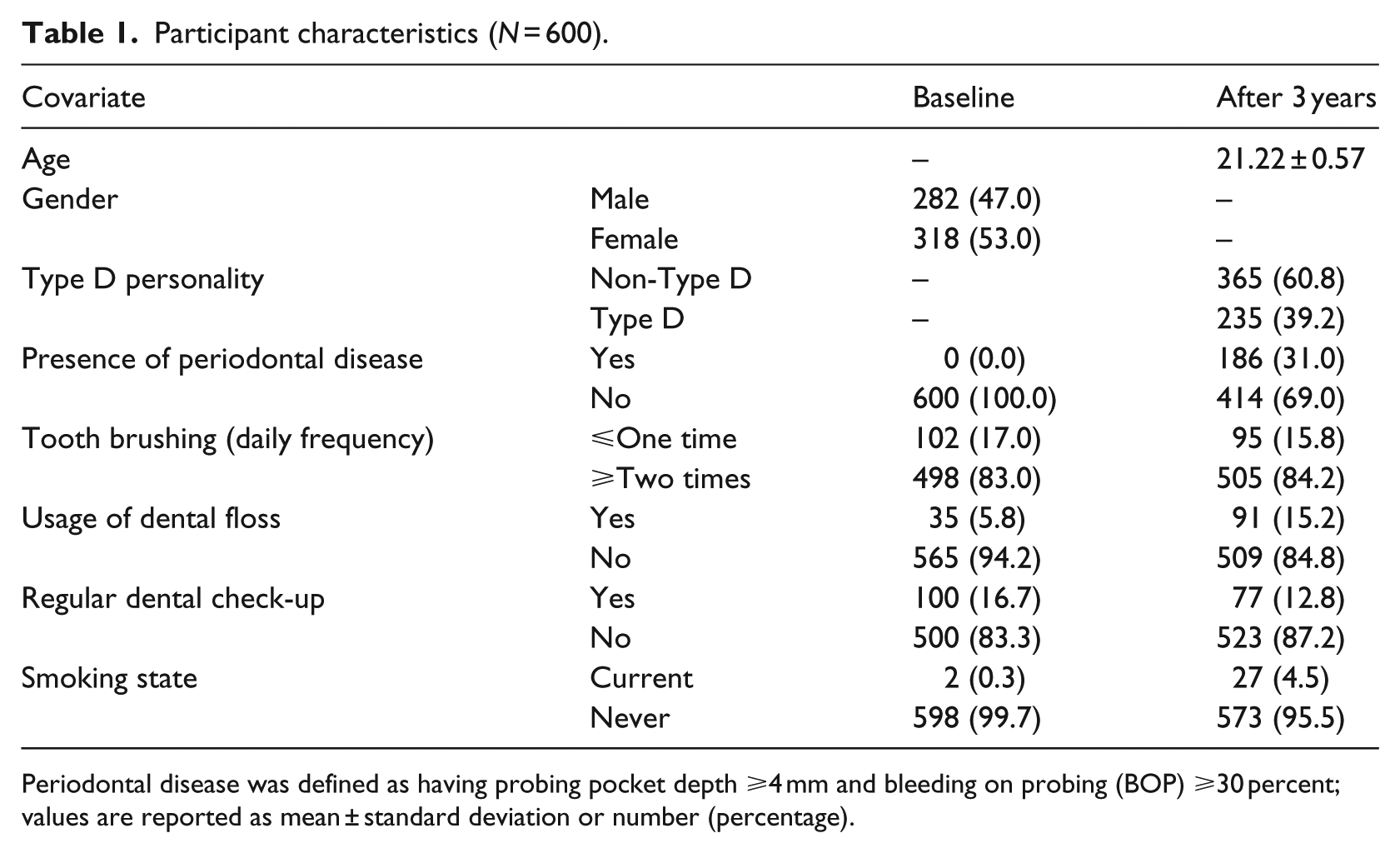
Periodontal disease was defined as having probing pocket depth ⩾4 mm and bleeding on probing (BOP) ⩾30 % values are reported as mean ± standard deviation or number (percentage).
Table 2 shows the association between Type D personality and oral health behaviors at baseline and after 3 years. A significant difference was not observed between Type D and non-Type D personality at both baseline and follow-up (Table 2).
Association between Type D personality and oral health behaviors at baseline and after 3 years in participants (N = 600).
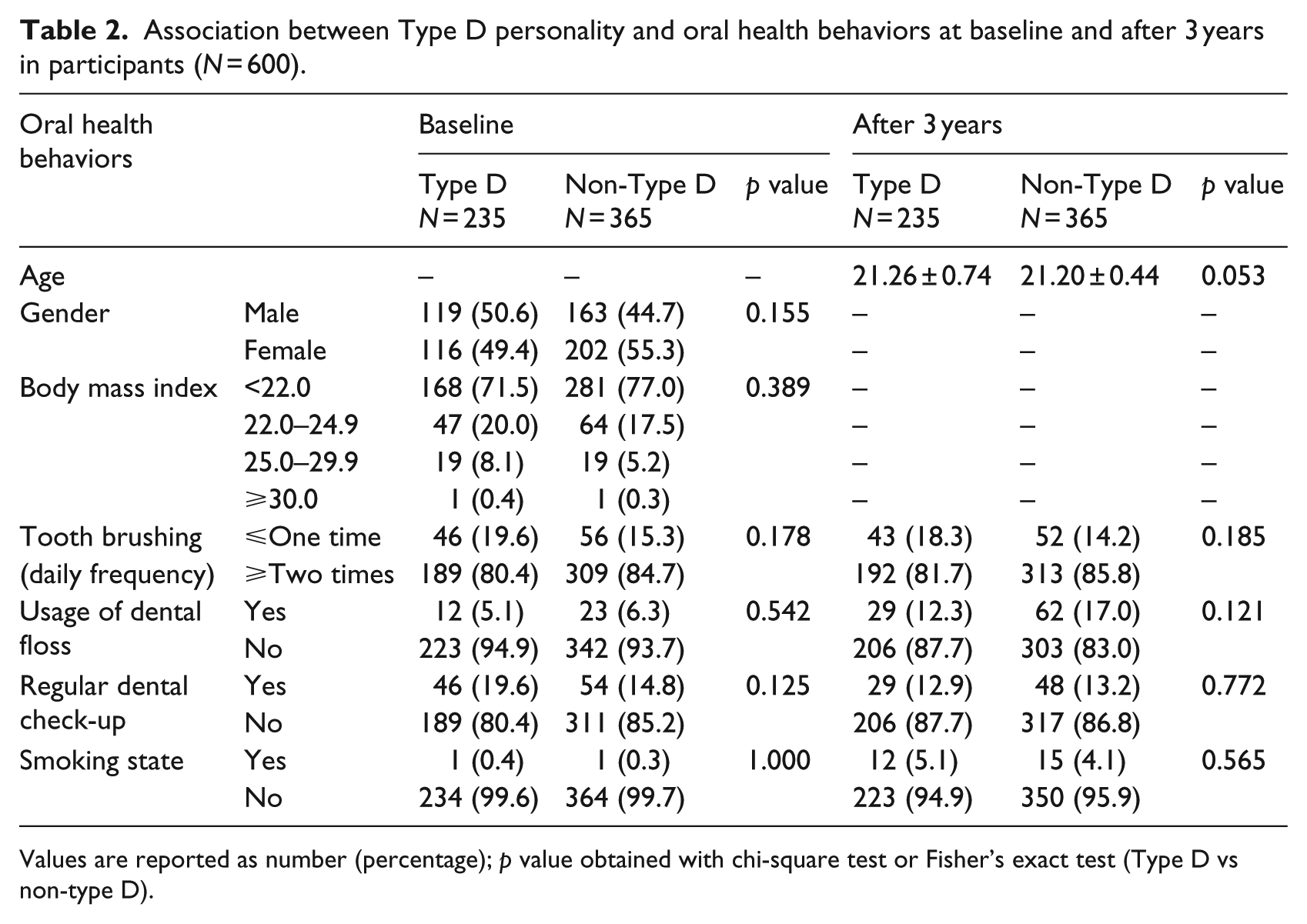
Values are reported as number (percentage); p value obtained with chi-square test or Fisher’s exact test (Type D vs non-type D).
The comparisons of covariates between the participants with and without progression of periodontal disease are shown in Table 3. The percentage of males with onset of periodontal disease after 3 years was 54.8 percent, while that without the onset of periodontal disease was 43.5 percent. The onset of periodontal disease was more prevalent in males than in females (p = 0.010). In the participants with Type D personality, the percentage of the onset of periodontal disease was higher than those in non-type D personality (p = 0.019). In addition, there was a significant difference between BMI at baseline and the onset of periodontal disease (p = 0.003); however, no significant differences between oral health behaviors at baseline and the onset of periodontal disease were observed (Table 3).
Association between onset of periodontal disease and related factors (N = 600).
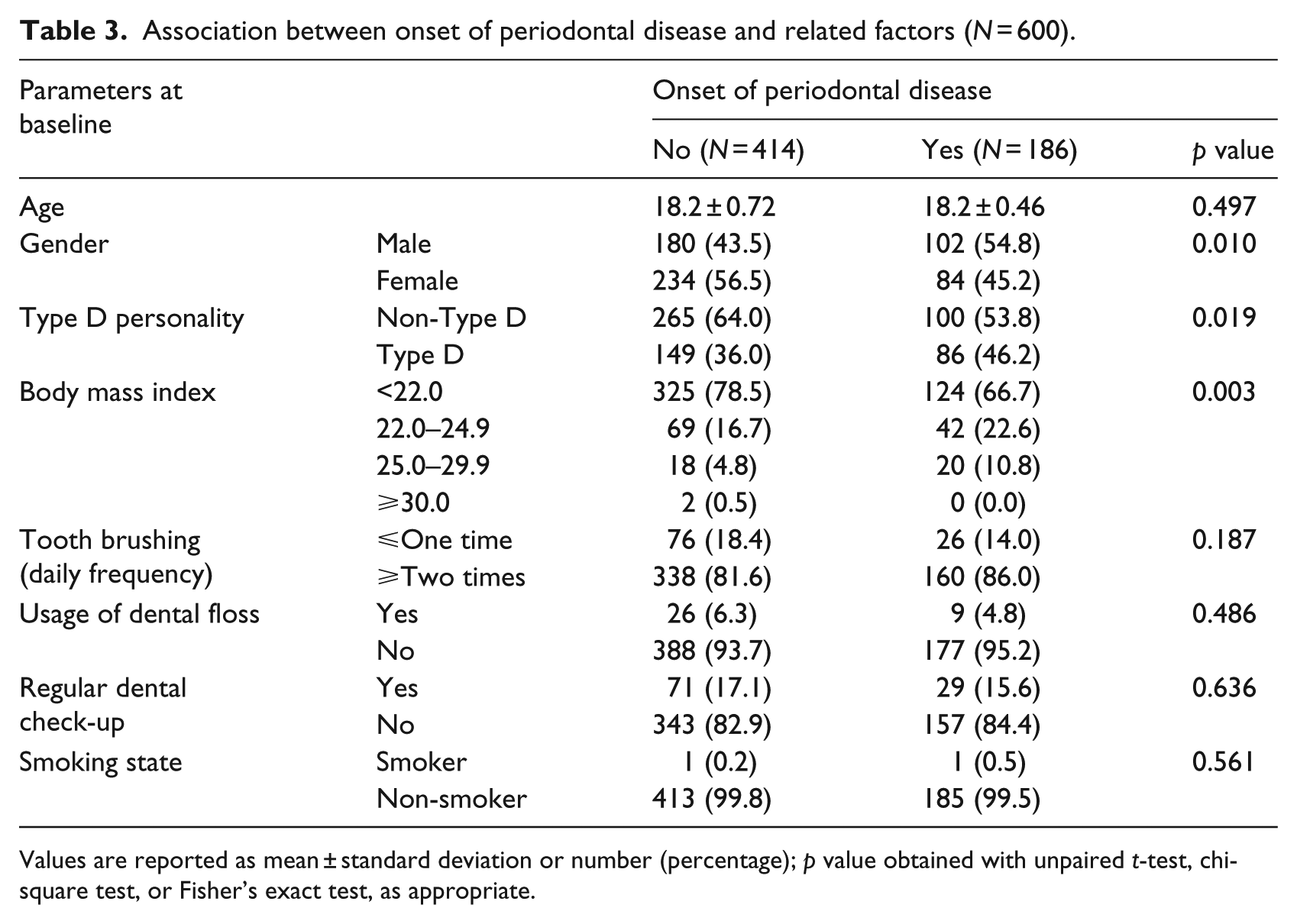
Values are reported as mean ± standard deviation or number (percentage); p value obtained with unpaired t-test, chi-square test, or Fisher’s exact test, as appropriate.
In the logistic regression analyses, the risk of periodontal disease after 3 years was significantly associated with “BMI ⩾ 25” (OR: 2.543; 95% CI: 1.297–4.989; p = 0.007) and “Type D personality” (OR: 1.473; 95% CI: 1.027–2.111; p = 0.035) (Table 4). The accuracy of discrimination was 69.5 percent, and the Hosmer–Lemeshow test found the model fit to be acceptable, with chi-square statistics of 7.704 (p = 0.359) (Table 4).
Adjusted odds ratios and 95 percent CIs for onset of periodontal disease.
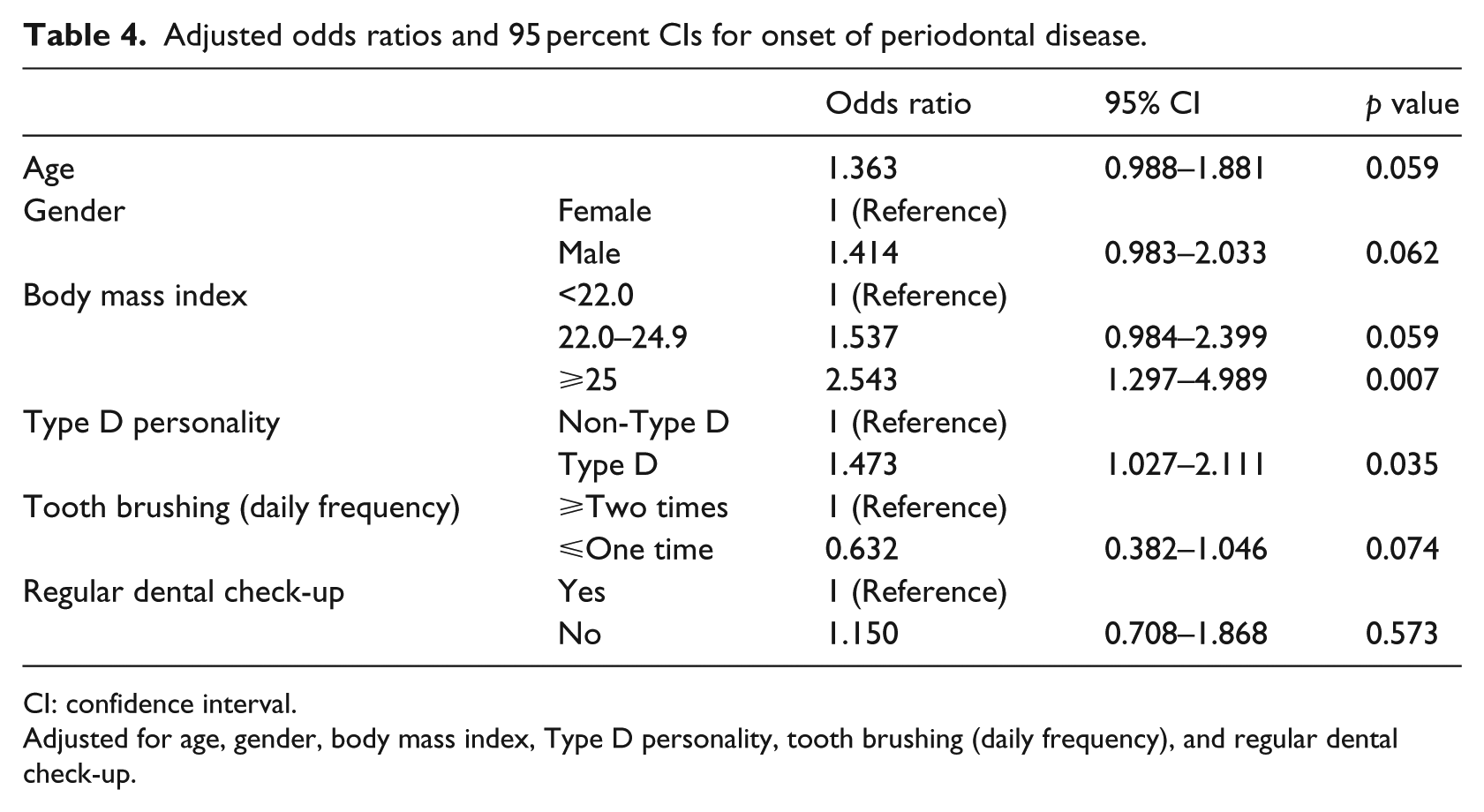
CI: confidence interval.
Adjusted for age, gender, body mass index, Type D personality, tooth brushing (daily frequency), and regular dental check-up.
Discussion
To the best of our knowledge, this is the first study which adopted Type D personality in the field of dentistry. In addition, we are the first to report the prevalence of Type D personality in Japanese young population. Our findings suggest that Type D personality is associated with the onset of periodontal disease during a 3-year period in young adults (Table 4). Although there are many risk factors, including diabetes (Simpson et al., 2010) and smoking (Tonetti, 1998), for periodontal disease, Type D personality may be evaluated as a new risk factor. In addition, the evaluation of Type D personality might be effective in the field of public health activity because measuring Type D personality is easy (Denollet, 2005), inexpensive, and can predict the occurrence of other diseases or health behaviors (Howard and Hughes, 2012; Kupper et al., 2007; Nefs et al., 2012; Schiffer et al., 2010; Yildirim et al., 2013).
Cortisol and stress are the common factors in the association between Type D personality and periodontal disease. Type D individuals tend to experience negative emotions (Denollet, 2000; Habra et al., 2003). Stressful situations involving fear, anxiety, helplessness, and loss of control result in release of cortisol (Sher, 2005). On the other hand, stress is one of the important risk factors for periodontal disease, and cortisol levels are associated with the extent and severity of periodontitis (Hilgert et al., 2006). Exposure to stress can induce the release of noradrenaline through the sympathetic nervous system by activation of the adrenal medulla, which can have immunosuppressive effects. Such immunosuppressive effect can enhance periodontal tissue destruction (Breivik and Thrane, 2011). Since the stress or cortisol levels of the participants in this study were not measured, we could not be certain whether Type D personality preceded the stress related to the onset of periodontal disease. Clarifying the mechanisms to explain the association among periodontal disease, stress, and Type D personality is the next critical step.
Type D individuals engaged in unhealthier behaviors including smoking, poor diet, and lack of physical activity are less likely to get regular medical check-ups than non-Type D individuals (Williams et al., 2008). However, there was no relationship between Type D personality and oral health behaviors in our results (Table 2). The discrepancy between our study and the previous study may depend on field (Japan vs the United Kingdom and Ireland). However, further studies may be needed to examine the relationship.
In this study, the risk of the onset of periodontal disease during 3 years was significantly associated with BMI ⩾ 25 (overweight/obesity) at baseline. Morita et al. (2011) showed a direct dose–response relationship between BMI and the subsequent development of periodontal disease in a population of 3590 Japanese individuals followed over 5 years. Our data are consistent with the previous study. Since obese individuals develop infections of various types more often than those with normal weight (Falagas and Kompoti, 2006), improving overweight during undergraduate days might be effective to prevent the onset of periodontal disease.
In our study, the prevalence of students with Type D personality was found to be 39.2 percent (Table 1). A previous study in the United Kingdom reported that the prevalence of Type D was 38.5 percent in 1012 healthy young adults (mean age: 20.5 years), which supports our result (Williams et al., 2008). On the other hand, a survey in Japan showed the prevalence of elderly Japanese people (⩾65) with Type D personality was 46.2 percent. The discrepancy of prevalence may be mainly due to differences in age groups (Kasai et al., 2013). Although many studies explained that Type D personality predicts the occurrence of various diseases (Nefs et al., 2012; Schiffer et al., 2010; Yildirim et al., 2013), it is unknown whether a disease affects the personality yet. Further studies may need to examine the relationship among Type D personality and age, race, or diseases.
The presence of periodontal disease was defined as the presence of both PPD ⩾ 4 mm and BOP ⩾ 30 percent. BOP is an earlier and sensitive indicator of inflammation (Greenstein, 1984), and deepened PPD with BOP (+) increases the risk of progression of periodontal disease (Oliveira Costa et al., 2011). Dentists usually diagnose periodontal disease using the results of PPD, clinical attachment level, BOP, and destruction of the alveolar bone. Thus, full-mouth periodontal examination is recommended (Dye et al., 2014); however, it is rather invasive and unsuitable for screening. We examined only 10 teeth, which can be underestimated compared with full-mouth examination.
This study had other limitations. First, all participants were recruited among many students at Okayama University. Thus, extrapolation of our findings to a general population of young-aged people may be limited. Second, the follow-up rate in this study was low (30.1%), as applicants received the 3-year follow-up examinations only just prior to graduation. However, there were no significant differences in oral health behavior, periodontal states, and body composition at baseline between participants who were followed up and those who were not (data not shown). Thus, the effect of sampling bias on the results may be small. Finally, we used BMI as measure of body composition. Although BMI is often used to assess obesity in young people (Ekuni et al., 2014), we did not know whether it is muscle or obesity.
In conclusion, a significant association between Type D personality and the onset of periodontal disease was observed in Japanese university students.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.