
Abstract
This study examined the difficulties couples face in relation to anorexia nervosa. Using interpretative phenomenological analysis, five couples in which one of the partners lives with anorexia nervosa were interviewed separately. The findings are conceptualized into three areas: first, the encounter ‘at the crossroads between remission and relapse’; second, the way that ‘anorexia reveals itself’; and finally, the way the ‘ménage à trois’ works, including the illness fully as part of the couple. Psychotherapists should take into account the context of the couple and the complex interaction between the couple and the illness to support both partners’ development of appropriate responses.
Introduction
Anorexia nervosa (AN) is a mental disorder characterized by a fear of gaining weight and a distorted body image, which leads to eating restriction and other weight loss strategies such as vomiting or physical activity (Zipfel et al., 2015). AN primarily affects adolescent girls and young women. A rise in the incidence of AN has been observed since the 1950s (Keski-Rahkonen et al., 2007; Lucas et al., 1999; Zipfel et al., 2015). AN, once conceived as an illness of adolescents, is now recognized as a significant mental health problem in adults (Woodside et al., 2000). Women with AN do not seem to differ from healthy women in their desire for committed relationships and engage in couples at rates comparable to healthy women (Maxwell et al., 2011).
Although the first studies on this topic are from the 1980s (e.g. Dally, 1984), study remains scarce in the AN literature (Bussolotti et al., 2002). The symptoms in women who live in couples are the same as those observed in single women: weight loss, disturbed body image, dieting, hyperactivity, laxative use or vomiting (Van den Broucke and Vandereycken, 1988). However, the intensity and frequency of these symptoms seem to be higher in the former group. In a comparative study based on marital status, AN patients who lived with a stable partner presented with greater age, duration of illness, number of treatments, weekly frequency of vomiting and eating psychopathology (Bussolotti et al., 2002). Approximately 25 per cent of them developed a chronic, relapsing course (Berkman et al., 2007) with frequent comorbidity (Fernandez-Aranda et al., 2007).
Despite their adulthood, patients remain dependent on their families or partners, both financially and emotionally (Bulik et al., 2012). They are often underemployed and socially isolated because of their weight loss, daily symptoms and treatments (Smethurst and Kuss, 2016; Treasure et al., 2001). For women with AN, their partners may be their primary interpersonal relationship (Pinheiro et al., 2010). Although many studies have considered the parents of these patients (e.g. Laghi et al., 2017), little attention has been paid to their partners (Woodside et al., 2000). Partners of women with AN often experience significant distress related to AN (Fischer et al., 2015; Ghizzani and Montomoli, 2000; Van den Broucke et al., 1995) and are challenged to understand how their loved one can starve before their eyes (Bulik et al., 2012). They must address a large variety of daily symptoms, such as refusal to eat and purging. They face relapse and chronicity of the illness as well as its consequences, such as the cost of treatment or social isolation. In terms of emotional aspects, partners report anger, anxiety, depression and guilt (Bulik et al., 2012). AN can thus be understood to be associated with chronic caregiver stress (Baronet, 1999).
Although patients with AN and their partners often report difficulties and distress in their romantic relationships, it is unclear what predicts a couple’s distress, which raises the question of interpersonal problems, such as discussions or conflicts about behavioural symptoms and recovery, between the partners (Bussolotti et al., 2002). In his study on couples with women who develop AN at or after the time of their marriage, Dally identifies a majority pattern in husbands’ behaviours (Dally, 1984): husbands are described as passive, avoiding interpersonal conflicts and, above all, wanting to be loved. Part of them welcomes the illness that reinforces their bond via a mutual dependence. A more recent study (Fischer et al., 2015) completes this description of partner behaviours by identifying two focused strategies in the distress of couples: change promotion, or helping the patient to eat, which emphasizes how a recovery would be positive, and acceptance/validation, or expressing empathy, which emphasizes the involvement of the patient in the recovery. Expectations of the partner with regard to change, ineffective modes of coping with the illness, patients’ preoccupations with their eating behaviours (Smith et al., 2016), unawareness of the adverse effects of AN and the patient’s reluctance to or readiness for change (Fox et al., 2011) or to be helped to change (Fischer et al., 2015) may be factors that disturb the relationship. These patterns of attitudes and interactions may even be involved in triggering or maintaining the disorder (Bussolotti et al., 2002).
Research proposes that involving both partners in the treatment of AN can be effective (Bulik et al., 2011). In the 1980s, Van den Broucke and Vandereycken (1988) recommended that the partner should be involved as a cotherapist to help the patient gain control over her eating symptoms. Other studies have underlined the potential benefits of adjunct support programmes dedicated to the partners to provide them with psychoeducation and opportunities to vent their feelings (Leichner et al., 1985). More recently, in line with the current extension of family-based interventions in treating younger patients, couple-based treatments have been presented as acceptable for both adult patients and their partners (Baucom et al., 2014). For patients in romantic relationships, however, the function given to the partner and the therapeutic work on the relationship cannot be directly derived from patients in family-based therapy (Bulik et al., 2011). Thus, it is important to better understand both patients’ and their partners’ experiences of AN to inform these types of treatments and couple counselling. It seems fruitful to approach this issue and to potentially deepen our understanding of it by analysing interviews with both partners. To this end, we interviewed dyads in which one of the partners lives with AN. Using a qualitative approach (i.e. interpretative phenomenological analysis, IPA) (Smith et al., 2009) in a dyadic way, our objectives were to identify the couples’ difficulties, understand the impact of the illness on the couples’ relational dynamics and provide evidence of the partners’ individual and dyadic adjustment modes for coping with the illness.
Method
Participants and procedure
The participants were recruited through the psychiatric and eating disorders department of the Saint Vincent University Hospital of Lille in northern France. Outpatients were selected from the list of persons followed by the eating disorders department between January 2014 and December 2014. The IPA approach is concerned with the participants’ experiences and the meaning that they give to those experiences. In the area of AN, this method has been used so far to analyse the patients’ experience of living with symptoms (see Fox and Diab, 2015; Fox et al., 2011). A relatively small and homogeneous sample is preferred to better capture the diversity of the lived experiences. Among the 15 couples who met the inclusion criteria mentioned below and who were called to discuss the project and solicit participation, 5 agreed to take part in the study. The study included married or cohabiting couples in which one member of each couple received a diagnosis of AN. Couples had to be in a committed relationship and cohabiting for at least 2 years. Their profile characteristics are shown in Table 1.
Participant information.
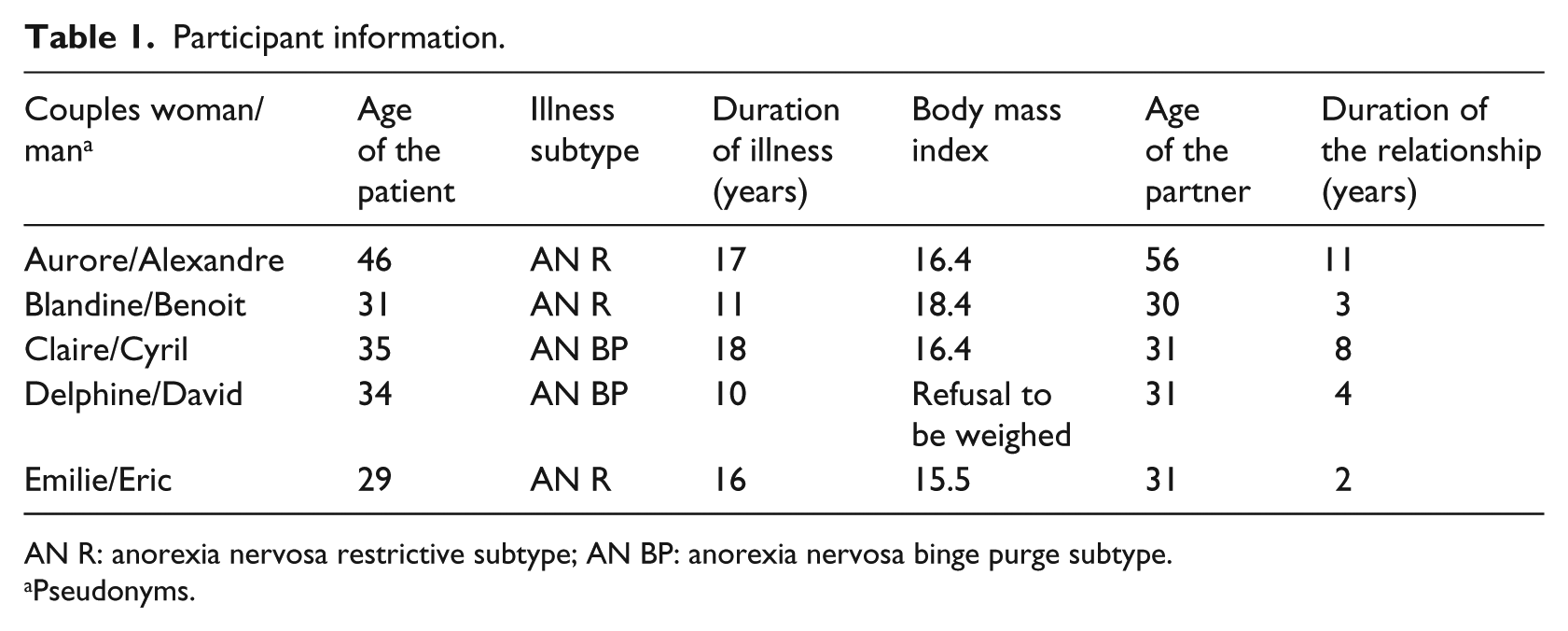
AN R: anorexia nervosa restrictive subtype; AN BP: anorexia nervosa binge purge subtype.
Pseudonyms.
The mean age of the partners was 35.8 years (standard deviation (SD) = 11.3 years), and the mean age of the women with AN was 35 years (SD = 6.6 years). The couples had lived together for an average of 5.6 years (SD = 3.8 years). An average of 14.4 years (SD = 3.6 years) had elapsed between the first AN diagnosis and the time of interview. The patients had body mass indexes (BMIs) in the 15.5–18.5 range at the time of the interview. All patients had a medical follow-up for AN at the time of the interview, two for a binge purge subtype and three for a restrictive subtype.
Ethical issues
The study was approved by the university ethics committee and adhered to the tenets of the Declaration of Helsinki of 1964, revised at Edinburgh in 2000. Each of the 10 participants was given an information letter and verbal explanations of the study details. If they agreed to participate in the study, they signed a consent form. Couples were assured that their information would be kept confidential and that their identity would not be revealed in published reports.
Interview
The two main types of dyadic IPA are separate interviews (see Antoine et al., 2013, for an example) and joined interviews (see Wawrziczny et al., 2016, for an example). The latter qualitative design creates a joint picture and considers shared experiences. However, we preferred a separate design that enabled each partner to tell the story from his or her own perspective (Morris, 2001) and that captured the individual within the dyad without neglecting the dyadic perspective (Eisikovits and Koren, 2010). The interviews occurred in the couples’ homes. The semi-structured schedule started with a general question about the consequences of the illness in the person’s life, followed by topics addressing treatment, eating, the body, the family, the couple, sexuality and the social and professional life. The patients’ interviews ranged from 69 to 110 minutes, and the partners’ interviews ranged from 55 to 132 minutes. The interviews were recorded and transcribed in full.
Data analysis
The interview transcription data were analysed qualitatively using IPA (Smith et al., 2009). The IPA approach allowed us to explore the participants’ experiences, the meaning they gave to those experiences and the underlying psychological processes. In a dyadic approach, IPA provides evidence of the experiences of each partner, the differences between each partner’s experiences and their points of divergence and convergence. The verbatim transcripts were read several times to ensure familiarity with the data. For each couple, all possible themes and sub-themes were identified for the patient, the partner and the couple as a whole. Shared themes, connections and discrepancies between partners were identified. References to the original verbatim transcripts were recorded under each sub-theme. Based on these couples’ analyses, an overall list of themes and sub-themes was developed with reference to the transcripts of the couples. All the transcripts were reread to guarantee that the final list of themes was representative of the interviews. Quotes were selected based not on their representativeness but on their ability to express a theme, to account for the diversity of phenomena or to relativize the scope of a theme. To preserve the anonymity of the participants, any identifying information was excluded or modified without changing the sense of the discourse. Finally, the results were presented and discussed in two wrap-up meetings in which the psychologists and psychiatrists in the eating disorders department considered whether the themes reflected the data and suggested new interpretative leads.
Results
The couples’ descriptions of their experiences with AN were conceptualized in terms of three broad areas and eight sub-areas (see Table 2).
Broad areas and sub-areas.

Emphasis is placed on the dynamics of the couples and the divergences and convergences rather than on individual paths. For each quote by the couples, two transcripts are presented side by side, one from the woman (on the left) and one from the man (on the right).
At the crossroads between remission and relapse
A remission conducive to the encounter
The women had in common a chronic anorexic history. All of the women in the sample consider their existence marked by alternating periods of acute disorder and periods in which symptoms are present but are residual and under control. These periods of remission are more serene and involve less disturbing weight loss. At these times, the disease is not an insurmountable obstacle to romantic encounters. At first, anorexia can be knowingly ignored. If it occurs again, its implications may not be understood by the partners or may be partially denied, as illustrated in Alexandre’s quote:

The prominence of fragility when choosing a partner
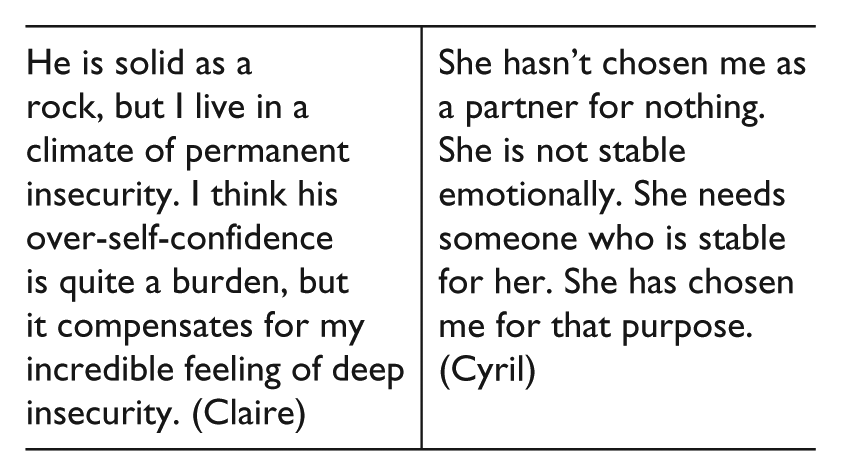
In this study, none of the couples fell in love by chance; they had to feel compatible or complementary to one another. A feeling of weakness on the part of the patients (for instance, see Claire’s quote below) or a deep-rooted lack of affection led them to look for certain qualities in their partners, from listening and kindness to stability and reassurance, depending on the couples. Reciprocally, the patients provided their partners with the opportunity to show understanding or be reassuring:
When the existence of AN becomes more evident, a gap has already emerged between the two partners. All the patients are determined to live with anorexia. Neither partner grasps the importance of the disease. Some of them (Alexandre, Benoit, Eric) thought that the worst was over and hoped to be the ones who could help the patients come to terms with their problems permanently.
An asymmetric commitment
The transitions from the encounter to the relationship and then to the commitment were marked by an asymmetry. This dynamic is more pronounced for two couples: Claire and Cyril and Delphine and David. The patients are torn between strong loving feelings and their reluctance to cope with the illness and an affective relationship in the long term. This ambivalence is translated into a waiting posture that gives them significant power in the ongoing negotiation of love. The partners, who are emotionally attached, face this resistance and commit themselves to overcoming it, which leads them to marry without any compromise with the patients or the AN. The relationship is thus permanently sealed with this third party:

When anorexia reveals itself
From small taboos to the dark side of the force
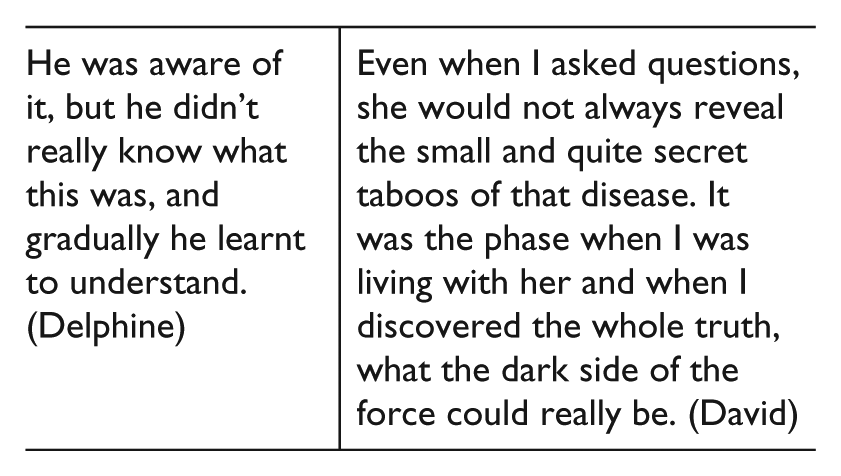
If the disorder emerged soon after the encounter, it was an abstract concept for the partners in our sample. With the beginning of their life together, the sharing of intimacy and symptoms that change in intensity, the patients introduced their partners to the reality of anorexia. There is no concrete picture of the symptoms that comes through in the partners’ statements; instead, we observe gradual anxiety in the face of the extent of the disease. Some of the partners, such as Cyril or David, were powerless when they discovered the negative impact of the disorder on their loved ones and on their life as a couple:
A compromised intimacy
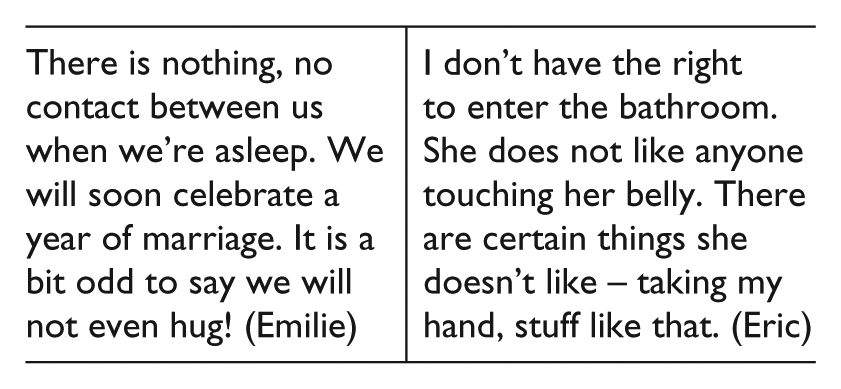
Affective gestures, accidental glances at the body and sharing intimate spaces are challenges when the body is exposed. The bodily areas usually subjected to dysmorphophobia, such as the belly, can be hidden from the partner’s gaze. For Aurore and Alexandre, this aversion extends to the whole body as well as the partner’s body. In all couples, some prohibitions are established, and a code of conduct emerges based on respect for the patients’ fears. This code seems very empirical and is based more on trial-and-error processes than on a negotiated functioning within the couples. In the case of Emilie and Eric, there seems to be an extinction of any form of intimacy beyond what is comfortable for the patient:
Globally, the couples’ sexual life is disturbed. Intimate life and symptomatic life seem to be exclusively related to the body, and they alternate without any possible coexistence. As well explained by Delphine, either issues caused by the symptoms prevent the patients from enjoying other forms of pleasure, or exhaustion does not allow the patients to experience desire or pleasure. Conversely, in the absence of symptoms, some of the patients might enjoy a satisfying sex life:

In some cases, other obstacles exist that are related to the patient’s unavoidable association of sexual intercourse and the memory of a previous trauma or in relation to internal conflicts that lead to the experience of intercourse as a degrading performance. Whatever the obstacle, the partner does not seem able to grasp it and adapts with a weak commitment to her sexual life.
Ménage à trois
The joint struggle
The temporality of the married couples in our sample follows that of the disorder that accounts for all domestic dynamics, both through the daily struggles around the body and food and, on a larger scale, with the alternation between relapses and remissions. This is well illustrated by the discourse of Claire and Cyril:

In all of the couples, the partner is caught in a spiral in which he becomes aware of having no control. He reacts in different ways: with caution by trying to understand how his partner lives, by taking over the doubts of his partner or by taking an active part in the struggle against her anxieties. This dynamic is reinforced by the ambivalence of the patients, who declare their wish to heal although, in practice, they seem to live with their illness and become inseparable from it. The partner is carried along with this hope. In all the couples, there is something unfathomable and unblamable in the dynamics of the partner because she manifests so much spontaneous guilt.
The symptoms might manifest quietly; they may be constantly present, but they may not be intrusive, and it may not be necessary to fight them. Given the intensity of crises at other times, patients may be content with this condition and may not want to disturb this appearance of a precarious balance. Thus, the symptoms are a constant threat to the partners, who may prefer to continue as if the disorder did not exist rather than suffer this insecurity. This causes ambivalence in the couples:
From active to passive distancing
Faced with daily symptoms, spouses adjust gradually and empirically to find the right attitude, whereas the patients are immune with regard to the perimeter around the disorders. Spouses oscillate between their estimation of the risk of intervening and their sense of helplessness generated by the independence they expect from the patients. In general, the partner is thus led to perform the function of reassuring and safeguarding the patient in ways that she tolerates or even seeks as long as he does not interfere in the intimate relationship she maintains with her symptoms. The dynamic between intervention and distancing may range from a physical power struggle (Blandine and Benoit) to detachment (Claire and Cyril and Delphine and David):
A petrified system
The functioning of the couples crystallizes into roles, and the regulation of the symptoms takes precedence over the loving relationship. Women fulfil a rather caricatured function as the best possible housewives. Their programme consists of being a good mother to everyone and maintaining a spotless household. In the long run, this commitment, which is coherent with daily hyperactivity, is a burden on top of the symptoms. The patient’s professional activity has stopped or is part time, which creates a sense of a lack of opportunity to fulfil herself. This reinforces a feeling of incompleteness. In a more paternalistic than loving style, men comfort, relativize, protect, temperate, and prevent fears and violence at the risk of wanting to protect them and let go. This dyadic system, by facilitating the control of symptoms, seems to contribute to maintaining the disorder. Some partners, such as Cyril, seem to be aware of their ambiguous behaviours; they may help in the short term but may be deleterious in the longer term. With this assistance, they prolong the disorder and support the efforts of the patients in hiding the need to cure the anorexia. They are animated by moments of disillusion, but they do not give up and assert their confidence in the future and the relationship. By contrast, the words of some patients, such as Claire, are far more detached and insecure. Their comments focus on anorexia and their feeling of breaking all ties:
Discussion
This study is one of the first to use qualitative and dyadic data to examine the functioning of couples in which one partner lives with AN. These functions were conceptualized in three ways: first, the encounter at the crossroads between remission and relapse; second, the way that AN reveals itself; and finally, the way the ménage à trois works, including the illness as an active participant in the couple.
Little is known about the way the couple is formed in AN and what factors contribute to partners choosing one another. Van den Broucke and Vandereycken (1988) suggest that the patient’s lack of self-esteem leads her to settle for a partner by default, whereas the man fantasizes about being in a caregiving role. In our study, these elements are combined with others in a complex chain. The period of remission seems to be a condition for the possibility of a romantic encounter. When the patient is not wrapped up in her physical and dietary concerns, she is likely to be more receptive to the relationship. In addition, the analysis of each dyad highlights that the encounter is marked by misunderstandings. The disease is not hidden, and its impact may even be visible. Nevertheless, the mark left by the illness on the identity of the patient and her conception of an existence with AN are beyond the partner. He captures the fragility emanating from the patient and believes that the illness will be relegated to the past. This fragility and the perception that it can be overcome are the basis of the relationship. This feeling is consolidated when the patient, who is less involved, distances herself, and the partner, who is intensely loving, promises to accept the patient as she is without jeopardizing her relationship to the illness.
The second set of results concerns the gradual realization by the spouse of the role of AN in the life of the patient and, more generally, in the couple itself. This process begins by highlighting a misinterpretation: the initial reluctance of the patient to address certain topics is attributed to modesty or shame. It then becomes apparent to the partner that it is not so much modesty as it is a taboo or opacity. Some partners understand that the function of this opacity is to protect the patient’s existing functioning with the symptoms. The spouse also discovers the extent of the psychic phenomenon. When he attempts to come closer to the patient in this context, he discovers that she is out of reach and that there is little he can do, even though the marriage is based on his ability to support his wife. Thus begins an empirical adjustment that consists of respecting the perimeter defined by the patient. Fischer et al. (2015) studied two main behavioural patterns used by spouses, defined as promoting change and acceptance/validation. The partner can work to change the patient’s behaviours or beliefs or demonstrate his empathy and unconditional support. There are no planned strategies, only a pattern of attitudes. The spouses have a profile similar to the categories described by Dally (1984): aside from exceptions associated with significant differences in age, the husbands seem passive; they avoid confrontation and seek to be loved above all else. For them, the AN has the advantage of strengthening dependency and collusion between the partners. Other husbands attempt to oppose the anorexic behaviour before they detach emotionally from the relationship by embarking on another romantic relationship or another area of life. What are presented as separate categories in the cross-study of Dally appear in the discourse of couples as steps in understanding disorders and the prioritization between the fight against the illness and self-preservation.
Previous studies have attempted to identify the role of interpersonal factors in maintaining AN (Treasure and Schmidt, 2013). The apparent adjustment of the couple can be explained by a lack of privacy offset by over-attachment (Van den Broucke and Vandereycken, 1988), and this relational organization may contribute to maintaining the disorder. In our study, the maintaining factors must be understood by incorporating the illness. The partner attempts to find an existence in relation to the patient, and the couple finds unity in negotiating or fighting the illness. The AN, through its constant presence, whether symptomatic or virtual, acts as a third partner in the couple.
The ambivalence of the patient has been extensively studied in the literature (Fox and Diab, 2015; Fox et al., 2011; Treasure and Schmidt, 2008). The interviews in this study show, in an original way, how this ambivalence contaminates the partner, who increasingly seeks to avoid being faced with conflicts about the illness. Even when the partner is gradually released from active patterns of change or acceptance/validation, the system is crystallized with the partner, who assumes a simple role of guarding the patient, which protects her link to her illness. The man is literally ‘the partner of the patient of the illness’. The imbalances observed during their meeting seem omnipresent; the partner remains loving even after becoming aware of his relative powerlessness, whereas the patient remains vigilant, ready to refocus on an exclusive relationship to her illness.
This qualitative study is the first to illustrate the links between AN patients and their partners. Nevertheless, some limitations must be noted. The participants are not representative of all adults living as couples with anorexia; in this study, the AN started at least 10 years before the relationship began. However, couples with a partner with AN can be divided into two categories: those who had the disorder before they met and those for whom the disorder occurred during married life. It is likely that the trigger factors as well as the adjustment strategies of these two types of couples differ. Thus, the findings are not transferable to other contexts, and a similar study among couples that formed before the onset of the disease is necessary. In future studies, it would be interesting to expand the sample to couples with recovery to understand how these couples manage to reorganize in the absence of an illness that has played a foundational and strengthening role in the relationship. A final limitation is twofold. The sample of patients had distinct clinical histories; they could be restrictive or combined with bulimic crises. The behaviours at play in these two groups differ. Furthermore, it appears in the interviews that symptoms play different roles in sexuality. Restriction decreases access to desire, whereas a bulimic crisis exhausts the patient and provides pleasure that replaces that generated by intercourse. However, it is difficult to go beyond these paths because the two sub-samples are limited. Future qualitative studies would benefit from more homogeneous samples.
Each identified theme has potential implications for treatment, especially in the follow-up of the chronic form of the disease. Traditionally, spouses are considered and informed but are not included in treatment. However, for more than 30 years, studies have argued in support of this approach and have defined the indications and contraindications (e.g. Van den Broucke and Vandereycken, 1988). Not including partners in treatment contributes to a climate of taboo around AN, which maintains the disorder. One of the most successful proposals to date is an interpersonal and cognitive-behavioural couple-based intervention for adult AN entitled Uniting Couples Anorexia Nervosa (UCAN; Bulik et al., 2011). Its authors have observed that engaging the partners in treatment is associated with lower dropout. A major issue is the many differences between the two partners, including knowledge about the disease, beliefs about development, the roles of each partner, perceptions of the state of the other partner, as well as goals and readiness regarding efforts to be implemented. These issues persist because of failing communication, and they have a negative impact on interactions that can worsen the disorder. These aspects are taken into account by the UCAN programme with work centred on psychoeducation and communication skills. Models such as structural couples’ therapy or integrative couples’ therapy (Jacobson et al., 2000) take into account other aspects of couples’ functioning, including shared ambivalence, conflicts associated with attempts at intervention for the symptoms, the role of AN in the constitution of the couple and the role of the increasingly rigid organization of the couple in maintaining the disorder.
Conclusion
Couples that met in the context of disease are characterized by a particular mode of functioning. Their meeting, daily life and terms of the relationship are forged around the illness. Couples testify to the role played by and given to symptoms in a complex relationship between the three protagonists. The treatments currently offered reflect the dyadic dimension and the specific functioning of couples with AN. It is important to continue in this direction by taking into account the complexity of this relationship, including the function of the couple in the maintenance of the disorder and the function of the disorder in the construction of the couple.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.