
Abstract
We modified the Weight Control Behaviours scale to explore unhealthy/healthy behaviours to increase, decrease or maintain weight in young adults (N = 1082) and associations with body mass index, depression and body image. Females reported more use of all strategies except those which increase body size or exercising to exhaustion. Although the sample reported more use of healthy weight management strategies, the use of dangerous ones warrants attention by healthcare professionals. Feelings of fatness was an important predictor of weight management behaviours. Public health campaigns should focus on the harmfulness of unhealthy weight management practices as well as the importance of healthy ones.
Introduction
With the high rates of overweight and obesity in Australia (63.4%; Australian Bureau of Statistics, 2015), New Zealand (66%; Ministry of Health, 2015) and worldwide (59%; World Health Organization, 2011), people are encouraged to engage in healthier lifestyle practices. Dieting is one common weight control strategy (Williams et al., 2007), with just under half of women in a large Australian study (Kenardy et al., 2001) reporting dieting for weight loss purposes in the last 12 months. Dieting has traditionally been considered as a unitary, negative construct (Wardle et al., 1997), often driven by aesthetic rather than health concerns (Calder and Mussap, 2015). However, considered more broadly, dieting is one example of a range of weight control behaviours (WCBs), which can encompass both positive strategies (e.g. regular exercise, eating well) and negative strategies (e.g. fasting, vomiting).
Prevalence of healthy and unhealthy WCBs
Although direct comparisons between studies is difficult for a variety of methodological reasons (e.g. French and Jeffery, 1994), and in particular the different contexts in which the behaviours are assessed (e.g. for weight loss, weight maintenance, dieting), general conclusions can be made. First, healthy WCBs are reported more frequently than unhealthy ones (e.g. Davison and Birch, 2004; Markey and Markey, 2005; Neumark-Sztainer et al., 2000). Second and related, the frequency of WCBs appears to be higher in women than men (Gillen, 2015; Markey and Markey, 2005; Wammes et al., 2007). For example, Markey and Markey (2005) reported that 95 per cent of females and 79 per cent of males had used a healthy WCB within the last 12 months, compared to rates of 57 per cent (females) and 36 per cent (males) for use of unhealthy strategies. Some studies do report gender similarities (e.g. Neumark-Sztainer et al., 2000); however, gender comparisons are limited by measurement problems in male samples (described further shortly).
Commonly reported strategies (e.g. used by more than 50% of the adult sample in at least one study) include eating more fruits and vegetables, limiting general food or junk intake, eating reduced fat or low-calorie foods, eating more fibre, limiting red meat, limiting salt, and exercise (Neumark-Sztainer et al., 2000; Wammes et al., 2007; Wardle et al., 1997). Specific unhealthy WCBs include vomiting, using diet pills, diuretic, laxatives or steroids, fasting and skipping meals. Use of these unhealthy behaviours is low in the general population (e.g. less than 10% in Neumark-Sztainer et al., 2000) but higher in adolescent females (e.g. 12.3%–25% in Cruz-Sáez et al., 2015a). Brown et al. (2015) suggest that use of unhealthy WCBs could be used as a ‘red flag’ for other psychological problems such as suicide ideation/plans/attempts, victimisation, feelings of hopelessness and substance abuse in adolescents. One WCB with a higher frequency is skipping meals (e.g. 51% in Savage and Birch, 2010), perhaps due to the increasing popularity of intermittent fasting, despite effects on mood and work performance stemming from distraction (Appleton and Baker, 2015). Diet-related WCBs are used more frequently than exercise (French and Jeffery, 1994; Serdula et al., 1999; Wammes et al., 2007). Only 20–30 per cent of individuals report using the recommended combination of monitoring food intake and engaging in sufficient exercise (e.g. weekly moderate-high intensity exercise and use of at least one weight gain prevention strategy, Serdula et al., 1999; defined as 150 minutes of exercise per week and reducing calories in Wammes et al., 2007; see Marks, 2016 for a discussion of the need to consider other factors than simply diet and exercise). However, dieters who anticipated exercise or viewed exercise as work (rather than fun) consumed more food compared to when no exercise was anticipated (Chang and Lin, 2015).
Associations with body mass index, body image and depression
Use of WCBs has been linked to a range of physical and psychological outcomes, but here we focus on depression, body image and body mass index (BMI) given their consistent associations with dieting behaviours. However, we extend this line of research by considering the unique associations with healthy and unhealthy WCBs (e.g. Gillen et al., 2012). Frequent dieting and use of extreme WCBs has been found to be predictive of negative body image outcomes such as increased restrained eating (French et al., 1995a), body dissatisfaction and drive for thinness (Cruz-Sáez et al., 2015a, 2015b; French et al., 1995a) in a sample of adolescents, as well as negative outcomes in adults. Kenardy et al. (2001) found that women who reported frequent dieting in the previous year were about three times as likely to report high levels of weight/shape dissatisfaction. Markey and Markey (2005) also reported that increased body dissatisfaction was associated with the use of more healthy and unhealthy dieting strategies in both men and women, even when controlling for BMI. Worryingly, Fredrickson et al. (2015) found that weight dissatisfaction was associated with restriction of healthy foods and greater consumption of unhealthy foods in a sample of overweight adolescents. Unhealthy dieting has also been linked to problematic eating behaviours (Laessle et al., 1996), with Hilbert et al. (2014) finding that the most common onset symptom for anorexia nervosa was dieting. Conversely, positive body image, defined as a love and respect of one’s body, has been associated with a lower use of unhealthy WCBs (Gillen, 2015) and coupled with self-compassion may lead to better quality of life (Duarte et al., 2015).
Unhealthy dieting strategies can have negative effects on psychological well-being (French and Jeffery, 1994; Kenardy et al., 2001). Associations between greater use of unhealthy dieting strategies and depression have been found in female adults (Gillen et al., 2012) and poorer psychological functioning in adolescent girls (Cruz-Sáez et al., 2015a). Negative affect has also been related to unhealthy eating behaviours such as binge eating (Rosenbaum and White, 2015) and overconsumption of high-calorie foods within a buffet setting for obese individuals (Privitera et al., 2019). Kenardy et al. (2001) reported that Australian women who dieted for weight loss five times or more in the previous year had a 45 per cent increased likelihood of depression compared to women who had never dieted. Lower levels of depression have been associated with a greater use of healthy WCBs in women (French et al., 1995b; Gillen et al., 2012) with a 15 per cent reduction in the likelihood of depression noted for low frequency dieters (Kenardy et al., 2001). These findings highlight how depression can be positively related to unhealthy WCBs but negatively related to healthy WCBs.
Increased BMI is consistently positively correlated with use of WCBs (Gillen et al., 2012; Kenardy et al., 2001; Neumark-Sztainer et al., 2000). More specifically, higher BMI has been associated with higher levels of healthy dieting in both men and women (Gillen et al., 2012; Markey and Markey, 2005), but the relationship is variable when considering unhealthy dieting (e.g. significant moderate positive relationship for men but no relationship for women in Markey and Markey, 2005; significant weak positive relationship for women but no relationship for men in Gillen, 2015). Other research has found that increased BMI has a moderate negative correlation with use of both healthy and unhealthy WCBs for both men and women (Gillen et al., 2012). Worryingly, research has also shown that a number of women who are underweight engage in dieting to lose weight (e.g. 21% in Kenardy et al., 2001). Considered together, Gillen et al. (2012) suggest that increased depression may be associated with less use of healthy WCBs, perhaps because depression may deplete cognitive resources needed for the forward planning of preparing healthy meals. Conversely, unhealthy strategies may serve as a form of self-punishment, particularly if the person is already experiencing body dissatisfaction or has a high BMI. Marks (2015) has recently described a comprehensive ‘Circle of Discontent’ model which (in part) discusses a feedback loop between increased weight, body dissatisfaction, the experience of negative affect and overconsumption of (typically) high-calorie foods.
Measurement issues
There are a small number of studies that have considered how BMI, depression and body image variables are related to both healthy and unhealthy strategies, but these may be limited by measurement issues. The commonly used Weight Control Behaviour Scale (French et al., 1995a), as well as many other similar lists of WCBs, contains few strategies employed by men. Men commonly report dissatisfaction with their muscularity (McCabe and Ricciardelli, 2004) and may engage in weight lifting or use protein supplements to build muscle mass (Ricciardelli and McCabe, 2003). We therefore added items designed to capture such behaviours. Furthermore, 10 out of the 11 items belonging to the ‘healthy weight loss methods’ subscale concern changes to eating, with only one item reflecting exercise. Therefore, we added a number of exercise-related items and differentiated between exercising at, and beyond, government-recommended levels (as excessive exercise is likely to be detrimental; Neumark-Sztainer et al., 1999). Finally, there are some women and a large proportion of men (McCreary et al., 2005) who wish to gain or maintain weight, rather than just reduce weight. We also added items to reflect strategies to increase weight using both healthy (e.g. used weight lifting to increase muscle mass) and unhealthy means (e.g. used steroids). Prevalence studies rarely consider weight-gain strategies. This diverse collection of behaviours may more accurately capture the range of strategies used by men and women to increase, decrease or maintain weight (collectively considered as WCBs) and is in line with research calling for greater care in the operationalisation of dieting strategies (French and Jeffery, 1994).
This study
We examined the prevalence of healthy and unhealthy WCBs in young adults (18–30 years) from Australia and New Zealand using an exploratory, modified version of the Weight Control Behaviour Scale which included a list of more nuanced and varied behaviours that men and women use to increase, decrease or maintain weight. Furthermore, we explored associations between these healthy and unhealthy WCBs and BMI, body image and depression. We predicted that increased BMI, depression and poorer body image would be predictive of use of unhealthy WCBs, while only increased BMI and poorer body image would be predictive of healthy WCB use. We tailored the selection of body image measures for males and females given that males are more likely to strive for muscularity and females are more likely to show concerns with reducing fatness (Ferreira et al., 2013; McCreary et al., 2005). We focused on young adults as this is a development period associated with increased risk for certain elements of body image and unhealthy eating. For women, body satisfaction appears to remain relatively stable across the lifespan (Tiggemann, 2004; Tiggemann and Lynch, 2001). However, dietary restraint and disordered eating have been found to be negatively correlated with age, and 20- to 29-year-old women in particular showed the greatest levels of disordered eating (Tiggemann and Lynch, 2001). Conclusions regarding body image across the lifespan for men are limited by the small number of papers in this area, but research generally suggests that weight and muscle tone are important elements of young adult men’s body image (McCabe and Ricciardelli, 2004).
Method
Participants
Data were gathered from 1082 participants aged between 18 and 30 years from a moderate-sized regional Australian university and a large urban university in New Zealand. The 808 females had a mean age of 21 years (standard deviation (SD) = 3.15) and an average BMI within the normal/healthy weight range (M = 22.76, SD = 4.36). The 274 males had an average age of 21 years (SD = 3.00) and on average had a healthy/normal BMI (M = 23.92, SD = 4.60). Most participants identified as being New Zealand-European (44%) or Australian-European (35%).
Measures
Body image
Separate scales were used for males and females to capture the distinct body image elements relevant to each sex. Although there was some overlap in constructs (e.g. both sexes completed measures of feelings of fatness), we used scales developed and normed for males and females separately as the aim was not to make direct comparisons between sexes.
For females, the 26-item Body Attitudes Questionnaire (BAQ; Ben-Tovim and Walker, 1991) was used to assess feelings of fatness (Feeling Fat; 13 items), satisfaction with physical appearance (Attractiveness; five items) and loathing of the body (Disparagement; 18 items). Items are rated on a 5-point Likert scale with higher scores indicating greater feelings of fatness, more feelings of attractiveness and greater loathing of one’s body. Sound psychometric properties have been noted previously (Ben-Tovim and Walker, 1991) and all subscales had acceptable internal consistency in this study (α = 0.75–0.94).
For males, the 15-item Male Body Attitudes Scale–Revised (MBAS-R; Ryan et al., 2011) was used to assess satisfaction with muscularity (Muscularity; seven items), satisfaction with body fat (Body Fat; five items) and height satisfaction (Height; three items). Items are rated on a 5-point Likert scale with higher scores indicating more negative attitudes. This scale has acceptable internal consistency in this study (α = 0.83–0.90) and in past research (Ryan et al., 2011).
Depression
The 9-item Patient Health Questionnaire (PHQ-9; Kroenke et al., 2001) is a self-report measure of major depressive disorder. Participants are asked how often they have been bothered by a range of problems (such as feeling down or hopeless) over the past 2 weeks. Items are scored on a 3-point Likert scale with higher scores indicating higher levels of depressive symptoms. This scale was shown to have acceptable internal consistency in this study (α = 0.88) and in past research (Kroenke et al., 2001).
WCBs
A modified version of French et al. (1995b) Weight Control Behaviour Scale was used as a measure of healthy and unhealthy dieting behaviours. Table 1 shows the items and categorises the modifications. For the healthy subscale, four items were retained (including one item from a Weight Loss factor), two items were modified (to increase specificity regarding exercise levels and to combine similar items) and three new items were added. Four items were dropped as they were similar dietary restrictions (e.g. reducing kilocalories, fat, meat and high carbohydrate foods). For the unhealthy subscale, four new items were added (two exercise and two dietary items), four original items were retained and two items were slightly modified (listed enemas; clarifying purposeful vomiting). These modifications were made to add more items relevant to males (e.g. ‘used weight lifting to increase muscle mass’; Neumark-Sztainer et al., 1999), modify wording throughout to acknowledge that participants may desire to gain weight or maintain weight (rather than simply lose weight) and increase the variety of behaviours given recent trends (e.g. new items such as ‘used protein shakes’).
Frequency of use within previous 12 months of weight management strategies among young adults (females and males) from Australia and New Zealand.
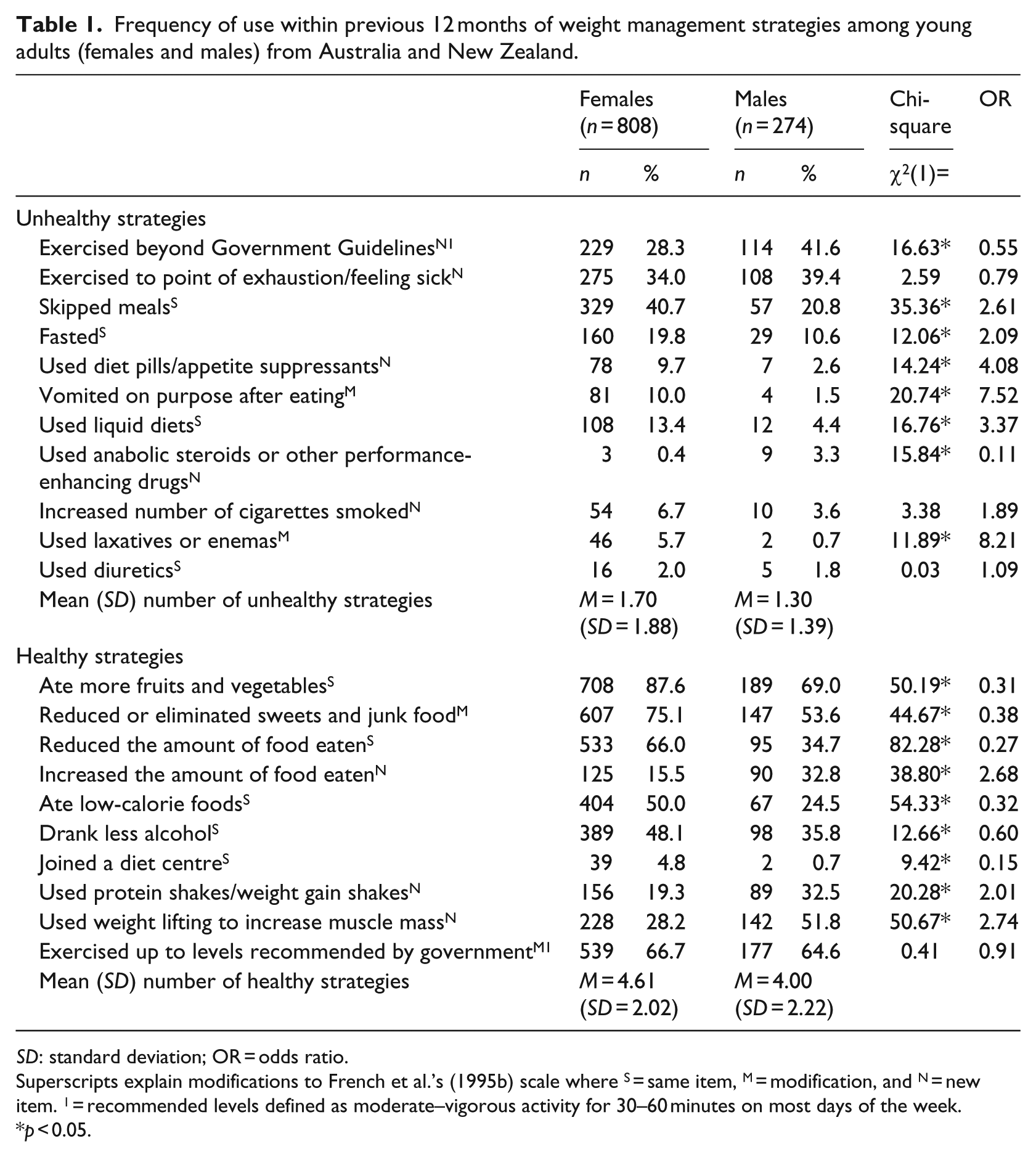
SD: standard deviation; OR = odds ratio.
Superscripts explain modifications to French et al.’s (1995b) scale where S = same item, M = modification, and N = new item. 1 = recommended levels defined as moderate–vigorous activity for 30–60 minutes on most days of the week.
p < 0.05.
The revised scale consisted of 10 healthy and 11 unhealthy behaviours. Participants indicated ‘yes’ or ‘no’ as to whether they had used each behaviour in the last 12 months (as per French et al., 1995b). A total score for each subscale is produced and represents the total number of WCBs used. Factor analysis supports the distinctiveness of the healthy and unhealthy scales (French et al., 1995b). The internal consistency of the two subscales were α = 0.62 for healthy and α = 0.68 for unhealthy.
Dieting status and excessive behaviours
Participants responded to one item asking about whether they had been on a weight management diet (to increase, decrease or maintain weight) in the past year and another item asking whether they were currently on a weight management diet. A further two items asked whether other people had expressed concern about their diet and exercise behaviours. All of these items were answered on a yes/no basis.
Procedure
Ethical approval was provided by the institutions of all authors. The online survey, hosted by SurveyMonkey, was sent out in Australia and New Zealand via social media (Facebook) and university emails, research participation and teaching/course sites of the two universities. This study forms part of a larger project examining rumination, worry and health behaviours. Participants were not given information about the specific research questions. Participants first answered demographics questions, followed by the BAQ or MBAS-R, PHQ-9 and WCB scale. After completion, participants were directed to another site where they could enter their email to be in the draw for a AUD$50 gift voucher.
Results
Frequency of healthy and unhealthy WCBs
More females than males had been on a weight management diet in the last year (27% vs 11%; χ2(1) = 27.98, p < 0.05, odds ratio (OR) = 2.87) and were currently on a diet (16.5% vs 8.5%; χ2(1) = 10.78, p < 0.05, OR = 2.15). Approximately twice as many females had reported that other people had expressed concern over their level of dieting (10% vs 4.5%; χ2(1) = 6.92, p < 0.05, OR = 2.20), but the value was similar for females and males in terms of other people’s concerns about excessive exercise (7.5% vs 7.7%; χ2(1) < 1, n.s., OR = 0.98).
In terms of WCBs (see Table 1), three of the top four healthy strategies were identical for males and females: eaten more fruit and vegetables, reduced junk food and exercise at recommended levels. Males also reported lifting weights to increase muscle mass while women reported reducing the overall amount of food consumed. The behaviours with the lowest frequency of use (<10% of sample) were joining a dieting centre (both sexes) and use of protein shakes (females). A greater percentage of women reported using each behaviour except for strategies designed to increase body size (increasing food consumption, use of protein shakes, lifting weights).
For unhealthy WCBs, the top strategies reported by both males and females included skipping meal and exercising to the point of exhaustion. Males also reported exercising beyond government recommendations while females reported fasting with high frequency. Low frequency behaviours (<10% of sample) in both males and females were use of steroids, vomiting, diet pills or diuretics, and increasing cigarettes. More females than males engaged in all of the unhealthy strategies except exercising beyond government guidelines or to the point of exhaustion, using steroids, and use of diuretics was equal between the sexes.
Both females (t(807) = 40.01, p < 0.001) and males (t(273) = 22.45, p < 0.001) reported significantly higher use of healthy WCBs compared to unhealthy ones. Use of healthy WCBs was significantly correlated with the use of unhealthy WCBs in both males (r = 0.47, p < 0.001) and females (r = 0.44, p < 0.001).
Associations with body image, depression and BMI
Bivariate correlations are shown in Table 2. Greater use of healthy WCBs was associated with greater BMI (small to medium effect size for males and females) and poorer body satisfaction (greater feelings of fatness (both males and females; medium effect size)), less feelings of attractiveness (females; small effect size) and greater disparagement (females; small to medium effect size)). However, healthy WCBs were also positively associated with satisfaction with muscularity for men (small effect size). Greater use of healthy WCBs was associated with greater depression in females (small effect size; but not correlated for males).
Correlations between men’s (below the diagonal) and women’s (above the diagonal) BMI, body satisfaction, and healthy and unhealthy weight management strategies.
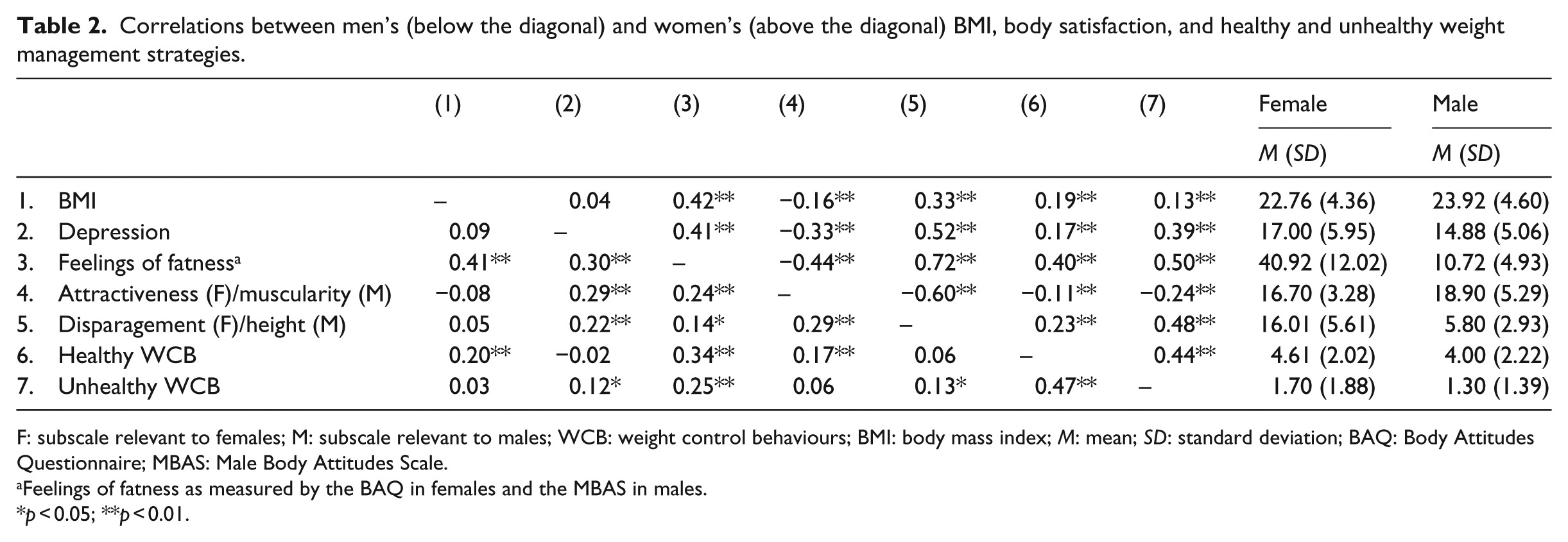
F: subscale relevant to females; M: subscale relevant to males; WCB: weight control behaviours; BMI: body mass index; M: mean; SD: standard deviation; BAQ: Body Attitudes Questionnaire; MBAS: Male Body Attitudes Scale.
Feelings of fatness as measured by the BAQ in females and the MBAS in males.
p < 0.05; **p < 0.01.
For males, greater use of unhealthy WCBs was only weakly (significant but small effect size) related to greater depression and satisfaction with height and not related to muscularity satisfaction. A small to moderate effect size positive correlation was found with satisfaction with fatness. For females, increased use of unhealthy WCBs was related to increased depression (medium effect size) and feelings of fatness (large effect size), as well as lower feelings of attractiveness (small to medium effect size), and greater BMI (small effect size).
A series of hierarchical regressions analyses were conducted to examine the predictors of healthy and unhealthy WCBs. BMI was entered in Step 1 as a control, with body image attitudes (BAQ for females, MBAS-R for males) and depression entered in Step 2. Separate analyses were conducted for males and females (see Table 3).
Multiple regression analysis of BMI, body image and depression predicting weight control behaviours.
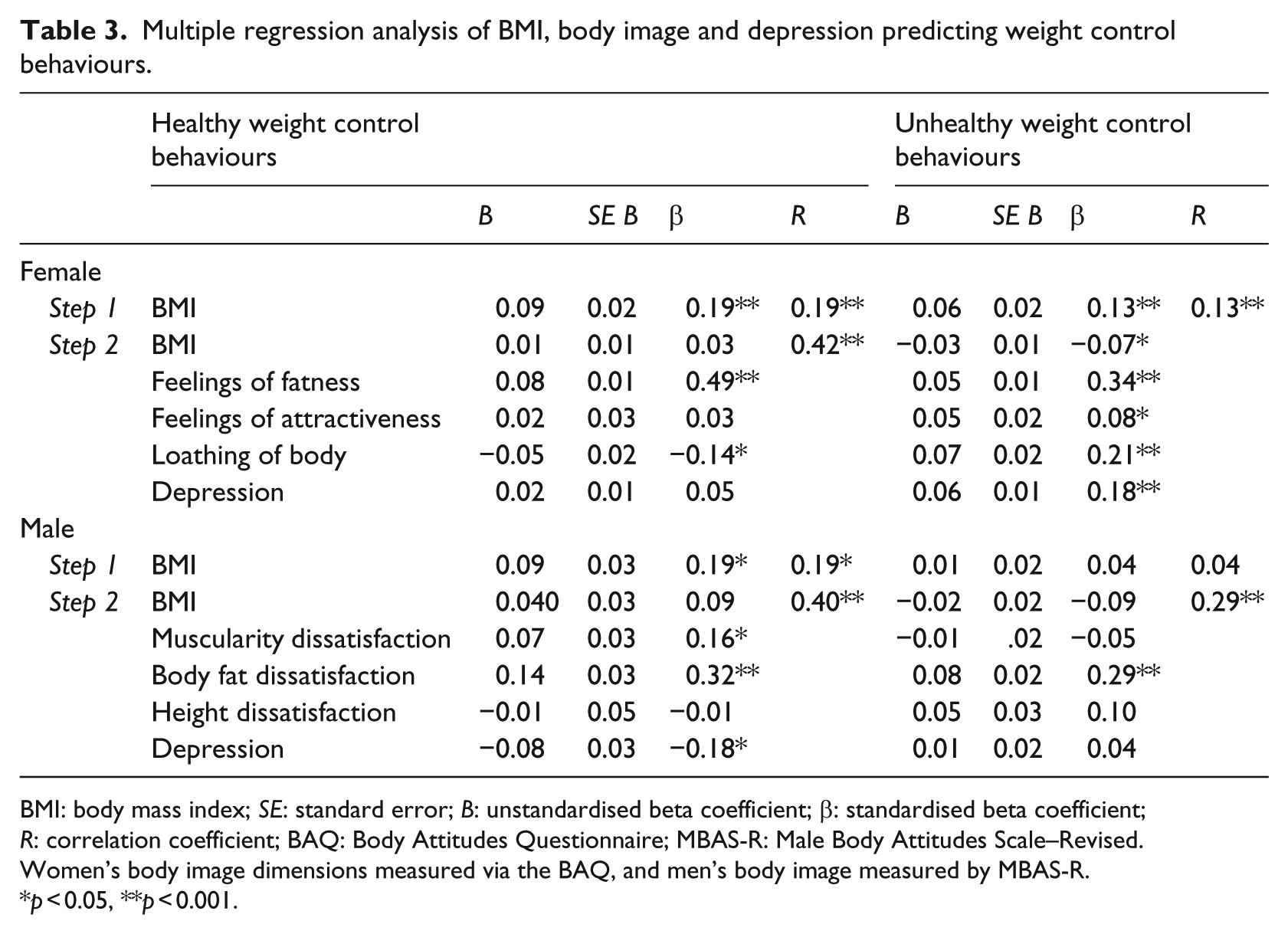
BMI: body mass index; SE: standard error; B: unstandardised beta coefficient; β: standardised beta coefficient; R: correlation coefficient; BAQ: Body Attitudes Questionnaire; MBAS-R: Male Body Attitudes Scale–Revised.
Women’s body image dimensions measured via the BAQ, and men’s body image measured by MBAS-R.
p < 0.05, **p < 0.001.
Healthy WCBs
For females, BMI accounted for a significant 3.4 per cent of the variance in healthy WCBs, F(1, 789) = 29.17, p < 0.001. When added to the model in Step 2, feeling fat, attractiveness, disparagement and depression resulted in a significant increase of variance (R2change = 0.14, Fchange (4, 784) = 34.06, p < 0.001) in healthy WCBs and the entire model remained significant F(5, 789) = 34.07, p < 0.001, accounting for 17.3 per cent of the variance. Greater levels of feeling fat and lower levels of disparagement were shown to be significant unique predictors of healthy WCBs for the female subsample. Feeling of fatness was the strongest predictor of increased use of healthy WCBs.
For males, BMI contributed significantly to the regression model, F(1, 265) = 9.59, p = 0.002, accounting for 3.1 per cent of the variance in healthy WCBs. The addition of depression and satisfaction with muscularity, body fat and height significantly improved the model, R2 change = 0.12, Fchange (4, 260) = 9.50, p < 0.001) and the model remained significant, F(5, 265) = 9.77, p < 0.001, and accounted for 14.2 per cent of the variance. Lower depressive symptoms and greater dissatisfaction with muscularity and fatness were all significant unique predictors of use of healthy WCBs. Similar to females, body fatness dissatisfaction was the strongest predictor.
Unhealthy WCBs
For females, BMI accounted for a significant 1.5 per cent of the variance in unhealthy WCBs, F(1, 789) = 13.23, p < 0.001. At Step 2, attractiveness, feeling fat, disparagement and depression accounted for a significant additional variance (R2change = 0.28, Fchange (4, 784) = 81.33, p < 0.001) of variability in unhealthy WCBs and the model remained significant, F(5, 789) = 68.79, p < 0.001, and accounted for 30.1 per cent of the variance. All predictors were uniquely significant; lower BMI, greater feelings of fatness, greater feelings of attractiveness, higher loathing of one’s body and greater depressive symptoms were all significant unique predictors of unhealthy WCBs. Again, feelings of fatness was the strongest predictor.
For males, BMI did not contribute to variance in unhealthy WCBs, F(1, 265) = 0.33, p = 0.56. At Step 2, depression, and satisfaction with muscularity, body fat and height contributed significant additional variance in unhealthy WCBs to the model, R2change = 0.08, Fchange(4, 260) = 5.97, p < 0.001, and the model remained significant, F(5, 265) = 4.85, p < 0.001, predicting 6.8 per cent of the variance. Only dissatisfaction with fatness was a significant unique predictor.
Discussion
This study assessed prevalence rates of weight management behaviours via exploratory modifications to the Weight Control Behaviour Scale (French et al., 1995b) which allowed for a greater distinction between strategies to increase, decrease or maintain weight and the inclusion of more diverse behaviours including those specifically related to men’s body image concerns. Collectively, our findings suggest that although young males and females report more use of healthy WCBs, there remains a significant risk of engagement in unhealthy behaviour. The importance of this research is underpinned by the negative physical and psychological health outcomes associated with unhealthy dieting practices (Jeffery, 1996), and the role of factors like dietary restraint, body dissatisfaction and depression as risk factors for the development of eating disorders (Stice et al., 2011). Furthermore, engagement in any strategy to lose or maintain weight is predictive of weight fluctuations longitudinally (Davison and Birch, 2004), especially for women who use both healthy and unhealthy strategies (Savage and Birch, 2010).
In terms of our first aim, young men and women were more likely to use healthy WCBs than unhealthy ones, and females reported more use of both behaviours than males. It is promising that the most frequently reported behaviours were healthy ones: eating more fruit and vegetables, reducing junk food and exercising at recommended levels. These findings are consistent with previous research (e.g. Davison and Birch, 2004; Gillen, 2015; Markey and Markey, 2005; Neumark-Sztainer et al., 2000), but extend it by including a wider variety of behaviours designed to increase, decrease and maintain weight. Of note was the measurement of exercise-related behaviours, which showed that about a third of the sample reported engaging in high levels of exercise to the point of exhaustion.
Of particular concern in this study was the number of males and females who reported disordered eating behaviours and steroid use. Although only reported by a small number of participants, steroids or other performance-enhancing drugs have considerable health consequences (Pärssinen and Seppälä, 2002) and associated with the use of other illicit drug use and sharing of needles (DuRant et al., 1993). Similarly, the rate of disordered eating (vomiting, laxatives, fasting) was relatively low, but concerning given that these behaviours are relatively stable with little chance of spontaneous recovery (Mills et al., 2012).
In terms of our second aim, feelings of fatness emerged as the most important predictor of both healthy and unhealthy WCBs for both males and females and provided more predictive utility than BMI. The importance of body image variables in the prediction of weight management behaviours is supported by previous research (Kenardy et al., 2001; Markey and Markey, 2005; Neumark-Sztainer et al., 2003), even when controlling for BMI (Markey and Markey, 2005; Neumark-Sztainer et al., 2003). Our findings extend this line of work by suggesting that feelings of fatness specifically, rather than body dissatisfaction/satisfaction more generally, is of importance. Other work has shown that feelings of fatness were positively related to perfectionism, perceived social pressure for thinness in women (Striegel-Moore et al., 1986) and tendency to engage in social comparison in both men and women (Ryan et al., 2011; Striegel-Moore et al., 1986). Positive relationships were also found with lack of control over eating, increased frequency of dieting, binging (Striegel-Moore et al., 1986) dietary restraint (Tiggemann, 1996) and eating disorders symptoms (Cooper et al., 2007). Considered together, attaching importance to weight, coupled with social comparison and perceived social pressures to achieve a thin physique may place individuals at risk of experiencing feelings of fatness which in turn may trigger a range of WCBs. Unsuccessful attempts at weight loss may further exacerbate feelings of fatness which in turn may then trigger more extreme dietary practices; a vicious cycle that may increase risk of the development of eating disorders.
Other body image variables were also important. For women, intense loathing of the body was also associated with greater use of unhealthy, and less use of healthy, WCBs. Greater satisfaction with appearance was also associated with more use of unhealthy WCBs. It is not clear why the attractiveness variable acts in a contradictory manner to the other predictors. Potentially, greater feelings of attractiveness may be associated with greater investment in appearance, which may then drive greater use of WCBs. Alternatively, the observed weak relationship may not be meaningful in the absence of other effects. For men, muscularity dissatisfaction was related to greater use of healthy WCBs, which may be explained by men seeking ways of varying their body shape through appropriate means. It may be that muscle dissatisfaction is not associated with unhealthy WCBs unless clinical samples are examined.
The combination of using both healthy and unhealthy WCBs may be particularly harmful. Savage and Birch (2010) reported that both types of WCBs were associated with increased weight gain over a 4-year period, greater weight concern, dietary restraint and more problematic eating attitudes and behaviours compared to women who use none or only healthy WCBs. Thus, public health messages should equally focus on ways to manage weight in a healthy way as well as the importance of avoiding unhealthy strategies (Savage and Birch, 2010).
Although we did not directly compare males and females, the pattern of associations between depression and WCBs was different across sexes. Higher depressive symptoms were predictive of greater use of unhealthy WCBs for females (but not males) and lower levels of depressive symptoms were related to healthy WCBs for males (but not females). That is, depression appears to act as both a vulnerability and protective factor. A similar pattern has been reported by Gillen et al. (2012), where depression was related to unhealthy WCBs in females but not males. The reason for this different pattern of results across gender and type of WCB is unclear, but may suggest a more complex interrelationship between factors such as poor coping and dieting failure (e.g. Kenardy et al., 2001).
Several limitations should be noted. First, the cross-sectional nature of this research does not allow for causal statements to be made. Second, self-reported height and weight may be prone to distortion, especially for overweight women (Rowland, 1990). Relatedly, BMI cannot distinguish between fat and lean masses (Wells and Fewtrell, 2006); additional measurements may be required. Third, the majority of our participants were university students who are not a good representation of the general community (Wardle et al., 1997). However, given the high prevalence rates of dieting, subclinical and clinical eating disorders, students remain a critical group to examine (Tavolacci et al., 2015). Fourth, it is often difficult to clearly delineate what constitutes a helpful versus harmful WCB (Neumark-Sztainer et al., 2000). Regular physical exercise, for example, is a recommended healthful behaviour, however excessive exercise is not. While items were designed to distinguish between these levels of exercise, the wording of other strategies may have required more precision. We asked about reducing calories and reducing food consumed, but not fat intake specifically, and it is likely that both are required for weight loss. Relatedly, use of WCBs may be harmful depending on the individual’s dieting motivations. For example, women who dieted for appearance-motivated reasons reported greater use of unhealthy WCBs, lower self-esteem, higher restrained eating and higher disinhibited eating compared to women who dieted for health-motivated reasons (Putterman and Linden, 2004). In their review paper, Brownell and Rodin (1994) point to the difficulties in identifying when dieting is helpful versus harmful. A range of factors are discussed including cognitions behind the dieting and greater consideration of the sample characteristics in terms of whether weight loss is needed (e.g. if there are health complications associated with a person’s excess weight vs someone who is underweight). Emerging evidence suggests that some people becoming obsessed with healthy eating and experience anxiety when trying to integrate vast amounts of dietary information (Rangel et al., 2012). More nuanced definitions of ‘dieting’ including reference to moderation of eating practices in future research may help here. Finally, we used different measures of body image for males and females to capture the unique concerns of each sex. This precludes direct comparisons, and while this was not the intention of the study, it nevertheless may have provided useful information about sex differences when predicting use of WCBs.
Future research is needed to more adequately test the psychometric properties of the revised scale. Here, our purpose was not to present a new scale but rather to explore usage rates of a broader number of dieting behaviours via small changes to an existing validated scale. Our Cronbach’s alpha levels were just below adequate (0.62–0.68) although only marginally lower than values reported in past research (e.g. 0.75 in Gillen, 2015). Further work on the factor structure of the scale may be needed.
Future research could consider WCBs in older age groups in order to provide information about the developmental course of such behaviours. For example, Serdula et al. (1999) found that while weight loss attempts generally increased with age for women, men aged 40–49 years were more likely to try and lose weight than the 18–29 year age group. These studies, along with those examining strategies in adolescent groups (e.g. Neumark-Sztainer et al., 2003), give insight in periods of development risk of dysfunctional WCBs. Future research would also benefit from including measures of positive body image such as body appreciation, which has been associated with the use of fewer unhealthy WCBs as well as greater psychological well-being in adult men and women (Gillen, 2015).
Despite these limitations, this study contributes to the limited literature assessing both healthy and unhealthy WCBs by considering strategies designed to decrease, maintain or increase weight (instead of just using the term ‘dieting’ which can be problematic, for example, Neumark-Sztainer et al., 1999). The inclusion of a wide range of strategies relevant for both males and females can provide health practitioners with a greater understanding of the strategies employed by young adults. Our findings show that feelings of fatness (rather than BMI) is a key predictor of engagement in both unhealthy and healthy WCBs in both young men and women. Therefore, prevention and intervention strategies are likely to benefit from addressing this body image component in young adults.
Footnotes
Acknowledgements
We wish to acknowledge Angela Hinz, Michelle Craig and Rosie Hoberg who assisted with the preparation of this paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.