
Abstract
The objectives of this study were to describe the cross-sectional associations between body-related self-conscious emotions and depressive symptoms in young adults and examine self-esteem as a moderator of these associations. Data from a population-based sample of 811 young adults were analyzed using hierarchical multivariate linear regression analysis. Body-related shame (β = .26) and guilt (β = .25) were positively related to frequency of depressive symptoms. Self-esteem was negatively related to frequency of depressive symptoms (β = −.46). Self-esteem moderated the association between body-related guilt and frequency of depressive symptoms. These findings suggest promoting self-esteem may help to reduce the negative effects of body-related guilt on depressive symptoms.
It is well established that the prevalence of subclinical depression is highest during young adulthood, with people in their 20s reporting the highest levels of depressive symptoms (Sutin et al., 2013). Depressive symptoms are highly recurrent, carry significant personal and societal consequences, and predict the development of clinical depression (Kessler et al., 2003; Klein and Allmann, 2014; Whiteford et al., 2013). As such, it is important to identify factors associated with depressive symptoms in young adults in order to identify opportunities to prevent and manage depression. Despite advancements in the knowledge of factors associated with depressive symptoms, more research is needed to identify risk and protective factors that can help inform evidence-based interventions for managing depressive symptoms during the high-risk years of young adulthood.
Experiences of guilt and shame have been consistently associated with higher depressive symptoms (see Kim et al., 2010, for review). The focus on these two self-conscious emotions is centered on the beliefs that negative thoughts and maladaptive beliefs related to the self create a vulnerability to depression (Abramson, et al., 1989; Beck, 1967; Gotlib and Hammen, 2008). According to Beck (1967), thoughts focused on the perceived loss in social status and failures, beliefs of inadequacy and worthlessness, and criticism and derogation of the self may result in overly pessimistic views of the self and lead to depressive symptoms. Building on this notion, researchers have proposed that self-conscious emotions of shame and guilt, which can result in feelings of powerlessness, helplessness, and hopelessness in the case of shame or result in feelings of tension, culpability, regret, and remorse in the case of guilt (Tangney, 1995), might contribute to the development and/or worsening of depressive symptoms (O’Connor et al., 1999; Tangney et al., 1995). Thus, self-conscious emotions should be considered in efforts to advance knowledge of factors that may be associated with depressive symptoms in young adults.
Self-conscious emotions
According to Tracy and Robins (2004), people experience self-conscious emotions of shame and guilt “when they become aware that they have lived up to, or failed to live up to, some actual or ideal self-representation” (p. 105). Although shame and guilt are closely related, they can be distinguished by the target and process of self-evaluation. Theoretical accounts of shame suggest that this emotion ensues following a negative evaluation of the global self in which the person feels inferior, helpless, or vulnerable about himself or herself as a whole (e.g. “I feel bad about who I am”). It is believed that internal, stable, and uncontrollable attributions for failure result in shame. Guilt ensues following a negative evaluation of the person’s behavior or action and entails remorse or regret (e.g. “I feel bad about what I did”). Guilt is believed to result from internal, unstable, and controllable attributions for failure. The difference between self-evaluation and behavior evaluation that distinguish shame and guilt has been demonstrated consistently in general and in specific domains of the self (Tangney, 1995).
The majority of researchers who have studied the association(s) between shame and/or guilt and depressive symptoms have focused on global experiences of shame and/or guilt (Averill et al., 2002; Gilbert, 2000; Webb et al., 2007). Based on 108 published studies reviewed by Kim et al. (2010), experiences of global shame and guilt contribute to depressive symptoms, with an overall moderate association for shame and small association for guilt. However, researchers have argued for the importance of considering domain-specific self-evaluation and behavior evaluation (i.e. domain-specific shame and guilt) because of the inherent differences in people’s evaluations from one domain to another (Marsh et al., 2006). In light of the prevailing view that appraisals of the global self are driven by evaluations of the physical self (Fox, 1997), researchers have started to assess body-related self-conscious emotions (e.g., Castonguay et al., 2012; Pila et al., 2015; Sabiston et al., 2010). They have argued that self-conscious emotions specific to the physical self may be experienced when people negatively appraise a stable and uncontrollable aspect of their physique (body-related shame) or in response to a negative appraisal of a specific controllable behavior associated with their physique (body-related guilt). Thus, it is important to consider whether young adults who report greater body-related shame and guilt report more frequent depressive symptoms. This association is expected based on previous findings showing that several body image constructs are associated with depressive symptoms (Hankin and Abramson, 2001; Paxton et al., 2006; Stice and Bearman, 2001). Moreover, there is emerging evidence that body-related shame and guilt are positively associated with depressive symptoms in obese adults (Conradt et al., 2007; Duarte et al., 2015) and adolescents (Grabe et al., 2007). Establishin an associations between body-related self-conscious emotions and depressive symptoms is important as it would highlight that these emotions poses a risk to young adults’ mental health in addition to putting them at risk for eating disorders (Stice and Bearman, 2001), which are prevalent in this population (Hudson et al., 2007). Nevertheless, limited attention has been paid to associations of body-related guilt and shame with depressive symptoms in young adults. The focus of this study is to extend the current literature beyond global guilt and shame and examine the associations between body-related shame, guilt, and depressive symptoms in a population-based sample of young adults. In addition, this study seeks to examine whether self-esteem affects the direction and/or strength of the associations between body-related self-conscious emotions and depressive symptoms.
Self-esteem as a possible moderator
Although it is evident that experiences of shame and guilt are associated with mild to severe depression, there is a large range in the magnitude of associations (r = .20–.70; Kim et al., 2010). Investigating factors that moderate the associations may explain this heterogeneity and determine for whom self-conscious emotions have negative psychological outcomes; yet, few researchers have investigated potential moderators (e.g. Marta-Simões and Ferreira, 2015). Identifying moderators may also provide insight into which subgroups of young adults are more likely to experience depressive symptoms as a result of experiencing body-related shame and guilt. Self-esteem is proposed as a potential moderating factor in this study for several reasons. First, several contemporary models of depression and empirical reviews highlight the role of low self-esteem in the development of mild to severe depression (Hammen, 2005; O’Brien et al., 2006; Orth et al., 2008, 2009; Sowislo and Orth, 2013). Specifically, it has been shown that having negative attitudes and perceptions of one’s body is associated with low self-esteem, which in turn is associated with more depressive symptoms (Choi and Choi, 2016; Duchesne et al., 2016). Second, it has been shown repeatedly that high self-esteem is associated with an absence or lower frequency of psychological symptoms such as depression (Babiss and Gangwisch, 2009; Dumont and Provost, 1999; Mann et al., 2004). Third, within diathesis-stress models (Beck, 1967; Butler et al., 1994; Metalsky et al., 1993), high self-esteem constitutes a protective factor such that it can help counteract the negative effect of stressors on the risk of developing mild to severe depression. Finally, high self-esteem has been associated with less global shame and guilt (Gruenwald et al., 2004) and less body-related shame and guilt (Castonguay et al., 2014; Conradt et al., 2007; Pila et al., 2015). As such, it is possible that body-related shame and guilt exhibit stronger associations with depressive symptoms in young adults who have lower self-esteem than in young adults who have higher self-esteem. However, no study to date has assessed whether self-esteem moderates the associations between body-related self-conscious emotions and depressive symptoms.
This study
The first objective of this study was to describe the associations between body-related self-conscious emotions of shame and guilt and depressive symptoms in a population-based sample of young adults. Based on previous studies focused on global self-conscious emotions (see Kim et al., 2010, for a review), it was expected that higher levels of body-related shame and guilt would be associated with more frequent depressive symptoms but that the association between body-related shame and depressive symptoms would be stronger than the association between body-related guilt and depressive symptoms. Furthermore, although it was hypothesized that body-related self-conscious emotions would be associated with depressive symptoms, there are likely individual differences in how young adults respond to experiencing shame and guilt depending on whether they have lower or higher self-esteem. Therefore, the second objective was to examine whether moderates the associations between body-related self-conscious emotions and depressive symptoms. Drawing on diathesis-stress models (Beck, 1967; Butler et al., 1994; Metalsky et al., 1993), it was hypothesized that body-related shame and guilt would not be significantly associated with depressive symptoms in young adults reporting higher self-esteem, or if significant, the magnitude of the associations would be small compared to the associations in young adults reporting lower self-esteem.
Methods
Participants and procedures
The study sample comprised young adults participating in the Nicotine Dependence in Teens (NDIT) study, a large prospective cohort study designed to describe the natural course of nicotine dependence in relation to cigarette smoking. The design and methods of the NDIT study are published elsewhere (O’Loughlin et al., 2015). For this study, 818 of the initial 1294 participants who were recruited for the NDIT study in 1999–2000 completed a follow-up questionnaire in 2011–2012. The present cross-sectional analyses were performed using data collected from participants in 2011–2012 (i.e. survey cycle 21) who provided complete data or had <5 percent of missing data on the exposure, moderator, and outcome variables (n = 811). Those retained for the current analyses were slightly older and more had university-educated mothers compared to those not retained. No other significant differences were observed between those who participated at follow-up and those who did not. Descriptive statistics on key socio-demographic variables are presented in Table 1. The NDIT study was approved by the ethics review boards at McGill University and the Centre de Recherche du Centre Hospitalier de l’Université de Montréal. Informed consent was obtained from all participants.
Descriptive characteristics of participants in the analytical sample, 2011–2012 (n = 811).

BMI: body mass index.
Measures
The Weight and Body-Related Shame and Guilt (WEB-SG) scale (Conradt et al., 2007) was used at survey cycle 21 to assess the degree to which participants experienced shame (six items) and guilt (six items) in the past 6 months. This assessment is meant to capture the dispositional or trait-like nature of body-related shame and guilt (Conradt et al., 2007). Responses were recorded on a 4-point Likert scale (from 1 = never to 4 = always). A mean score was calculated for each self-conscious emotion. WEB-SG scores have demonstrated adequate reliability and validity (Conradt et al., 2007; Sabiston et al., 2010). Cronbach’s alpha coefficients for this study were .90 and .89 for shame and guilt subscales, respectively.
The Major Depression Inventory (MDI; Bech et al., 2001) was used to assess frequency of depressive symptoms. The MDI assesses the extent to which participants experienced 10 depressive symptoms in the past 2 weeks on a 6-point scale (from 0 = at no time to 6 = all the time). Items 8 and 10 had two sub-items (a and b), and only the highest of the two scores was used. Participants’ responses were averaged. The validity and reliability of MDI scores have been established (Bech et al., 2001; Olsen et al., 2003). Cronbach’s alpha coefficient for this study was .90.
The Rosenberg Self-Esteem (RSE) scale (Rosenberg, 1965) was used to assess self-esteem. It is a measure of global self-esteem that consists of 10 statements. No time frame or referent period is used in this dispositional measure of self-esteem. Responses were recorded on a 4-point Likert scale (from 1 = strongly disagree to 4 = strongly agree). Negatively stated items were reverse coded, and a mean score was calculated. Researchers have shown that RSE items are internally consistent and that the global score has predictive validity (Brunet et al., 2010; Diehl et al., 1998). Cronbach’s alpha coefficient for this study was .87.
A questionnaire was used to collect data on participants’ socio-demographic characteristics (age, sex, weight, height, ethnicity, educational attainment, and annual household income (<CAN$30,000–49,999; CAN$50,000–99,999; and >CAN$100,000)). Body mass index (BMI) was calculated as current self-reported weight (kg) divided by the square of self-reported height (m).
Data analysis
Prior to analysis, the data were checked for normality, outliers, and multicollinearity. Missing data on the exposure, moderator, and outcome variables were minimal (<5%) and estimated using multiple imputation methods (Yuan, 2010). Data on potential covariates were not estimated as >5 percent were missing. Descriptive statistics and Cronbach’s alpha coefficients were computed for multi-item measures. Bivariate correlations between the main study variables were examined, and the correlation coefficients obtained for the body-related shame and depressive symptoms association and for the body-related guilt and depressive symptoms association were compared using Fisher’s r-to-z transformation. Following procedures recommended for testing moderation described by Aiken et al. (2003), hierarchical multivariate linear regression analysis was conducted to assess the associations between body-related self-conscious emotions and depressive symptoms (objective 1) and determine whether self-esteem moderated these associations (objective 2). Interaction terms were created for body-related shame and self-esteem and for body-related guilt and self-esteem by multiplying the mean-centered variables, respectively. Entry was specified a priori where age, sex, BMI, education attainment, and household income were included in the first step; mean-centered body-related self-conscious emotions were entered in the second step; mean-centered self-esteem was entered in the third step; and the interaction terms were included in the final step. A moderator effect was supported if the interaction term was statistically significant at p < .05. The nature of the significant interaction was explored using simple slope analysis and a graphical representation using the regression coefficients for lower (>1 standard deviation (SD) below the mean) and higher (>1 SD above the mean) self-esteem (Aiken et al., 2003).
Results
Examination of the data revealed no univariate or multivariate outliers. The distributional properties of the exposure, moderator, and outcome variables suggested that they were all normally distributed as skewness and kurtosis values were below values that might reflect problems with the distribution of the data (i.e. all values were between −1.5 and 1.5). In addition, the variance inflation factor values for each independent variable were all <2.95, indicating that there was little or no multicollinearity issues. Descriptive statistics for the main variables are presented in Table 1. On average, participants reported low body-related shame and guilt, low frequency of depressive symptoms, and high self-esteem relative to the scale ranges.
A number of significant bivariate correlations were observed. Specifically, body-related shame and guilt were positively intercorrelated (r = .73). Body-related shame (r = .42) and guilt (r = .38) were positively associated with frequency of depressive symptoms, and the magnitude of these two associations was comparable based on Fisher’s r-to-z transformation (p < .001). Self-esteem (r = −.57) was negatively associated with frequency of depressive symptoms. Finally, body-related shame (r = −.44) and guilt (r = −.34) were negatively correlated with self-esteem.
The results of the hierarchical multivariate linear regression analysis are presented in Table 2. Based on the model controlling for age, sex, BMI, education attainment, and household income in Step 1, body-related shame and guilt were positively and significantly associated with frequency of depressive symptoms in Step 2. Also, self-esteem was inversely and significantly associated with frequency of depressive symptoms in Step 3. The interaction between body-related guilt and self-esteem was significant in Step 4; the interaction between body-related shame and self-esteem was not. The four steps accounted for 38 percent of the variance in frequency of depressive symptoms. As shown in Figure 1, and based on the simple slope analysis, the positive association between body-related guilt and frequency of depressive symptoms was significant among participants who reported lower self-esteem (β = .33, 95% confidence interval (CI) = 0.39–5.14) but not significant among those who reported higher self-esteem (β = .11, 95% CI = −0.56–1.67).
Hierarchical multivariate regression analysis examining the associations between body-related self-conscious emotions, self-esteem, and frequency of depressive symptoms controlling for age, sex, body mass index, educational attainment, and household income.
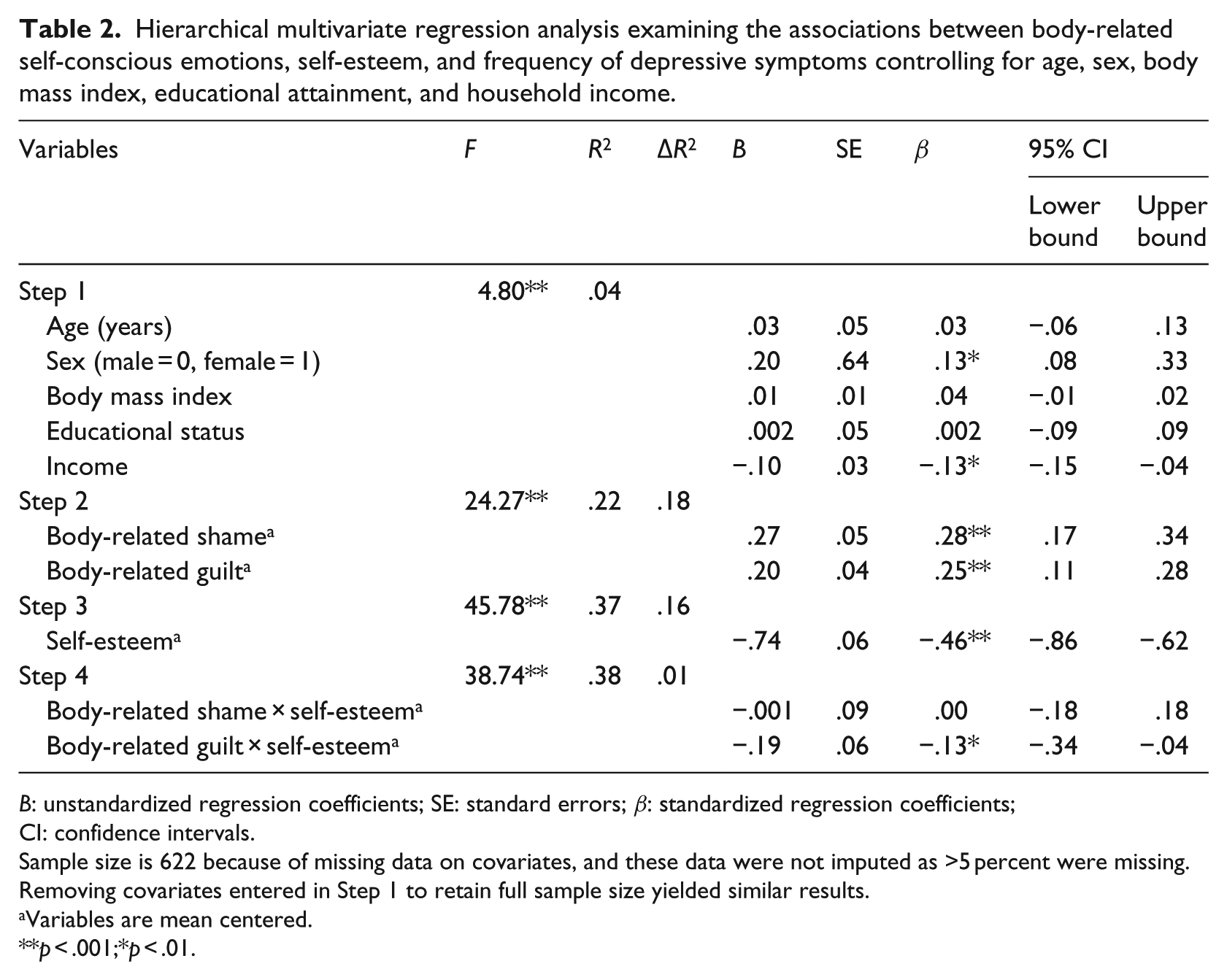
B: unstandardized regression coefficients; SE: standard errors; β: standardized regression coefficients; CI: confidence intervals.
Sample size is 622 because of missing data on covariates, and these data were not imputed as >5 percent were missing. Removing covariates entered in Step 1 to retain full sample size yielded similar results.
Variables are mean centered.
p < .001;*p < .01.
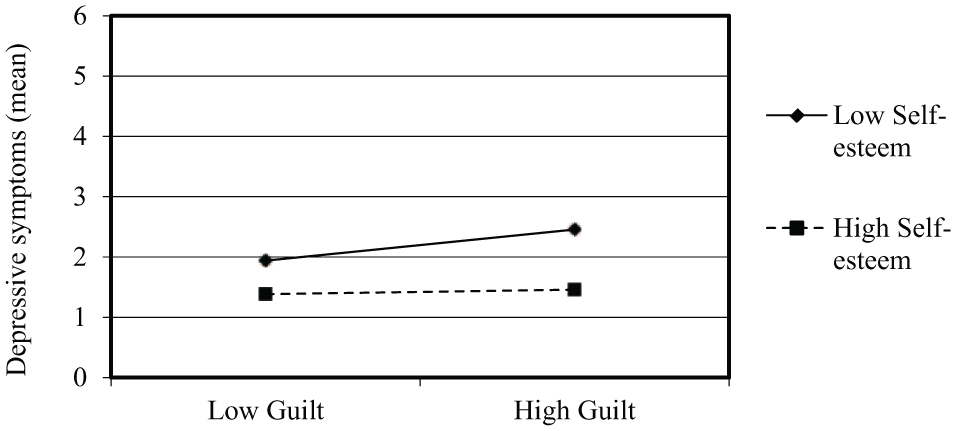
Significant two-way interaction involving body-related guilt and self-esteem on frequency of depressive symptoms.
Discussion
The objectives of this study were to extend the limited literature linking body-related self-conscious emotions of shame and guilt with depressive symptoms in young adults and determine whether self-esteem moderates these associations. As hypothesized, both body-related self-conscious emotions were positively and significantly associated with frequency of depressive symptoms even after controlling for potential confounders. The second hypothesis was also supported, albeit only partially, as the association between body-related guilt (but not body-related shame) and frequency of depressive symptoms was moderated by self-esteem. Further interpretation of the moderating effect of self-esteem indicated a stronger positive association between body-related guilt and frequency of depressive symptoms in participants with lower self- esteem compared to participants with higher self-esteem. This is an interesting discovery and offers a novel contribution to the literature in that it may help to explain variations in the magnitude of associations previously reported (Kim et al., 2010). It also provides a target for interventions seeking to reduce the negative impact of body-related guilt on depressive symptoms in young adults.
Although several researchers have reported associations between self-conscious emotions and depressive symptoms (see Kim et al., 2010, for a review), these reports are based on global measures of shame and guilt. This study is among the few that have assessed body-related self-conscious emotions (Castonguay et al., 2012, 2014; Conradt et al., 2007; Pila et al., 2015; Sabiston et al., 2010) and addresses calls to examine the link between body-related self-conscious emotions and health outcomes (Calogero and Pina, 2011; Marta-Simões and Ferreira, 2015). Specifically, these findings highlight that body-related self-conscious emotions are related to depressive symptoms and advance the current literature that is focused primarily on global self-conscious emotions (Averill et al., 2002; Gilbert, 2000; Webb, et al., 2007). Furthermore, these associations add to the scant body of the literature linking body-related self-conscious emotions to depressive symptoms (Castonguay et al., 2014) and to the literature linking other body image constructs to psychopathology (Altabe and Thompson, 1996; Tiggemann, 1996). For example, researchers have shown that negative body-related self-evaluations are associated with depressive symptoms (Hankin and Abramson, 2001; Paxton et al., 2006; Stice and Bearman, 2001). Although it is not possible to establish a causal effect of body-related shame and guilt on depressive symptoms based on this cross-sectional analysis, these results underscore the importance of considering young adults’ experiences of body-related shame and guilt to prevent and treat depressive symptoms. Based on existing interventions that have been effective in improving body image (Campbell and Hausenblas, 2009; Farrell et al., 2006; Jarry and Ip, 2005; Yager et al., 2013), cognitive-behavioral therapy, cognitive dissonance training, mindfulness-based interventions, and/or physical activity interventions could be evaluated to determine whether they are effective in reducing body-related shame and guilt and subsequently preventing or reducing depressive symptoms.
Departing from the hypothesis and from existing literature on global shame and guilt (Kim et al., 2010), the magnitude of the associations between both body-related self-conscious emotions and depressive symptoms was similar. One reason could be that body-related self-evaluations are highly relevant in young adulthood (Bucchianeri et al., 2013; Grossbard et al., 2008) and thus have a negative impact on depressive symptoms, regardless of whether they are in relation to the self as a whole (body-related shame) or in relation to one’s appearance-management behaviors (body-related guilt). Also, the significant interaction between body-related guilt and self-esteem supported the hypothesis that having a more favorable impression of oneself (higher self-esteem) may attenuate the positive associations between body-related guilt and depressive symptoms. From a theoretical perspective, this finding is consistent with previous theorizing that high self-esteem can help to counteract the negative effect of stressors on the risk for the development and/or worsening of mild to severe depression (Beck, 1967; Butler et al., 1994; Metalsky et al., 1993). As such, it points to the need to consider self-esteem when examining the association between body-related guilt and depressive symptoms. From a practical perspective, this finding suggests that young adults with more favorable global self-evaluations may be less affected by their perceived failures to enact appearance-management behaviors. This pattern implies that promoting self-esteem may help to reduce the negative effects of body-related guilt on depressive symptoms in young adults.
Contrary to the hypothesis and diathesis-stress models (Beck, 1967; Butler et al., 1994; Metalsky et al., 1993), self-esteem did not significantly moderate the association between body-related shame and depressive symptoms. A likely explanation for this finding may relate to the nature of the self-evaluations of shame. Because shame is conceptualized as a negative evaluation of self as a whole (Tangney, 1995), it is assumed to result from internal, stable, and uncontrollable attributions for failure. Thus, responses to body-related shame may be negative regardless of self-esteem because people do not believe that they can change the self as a whole. Owing to the positive association between body-related shame and depressive symptoms observed herein, researchers should seek to identify other factors that protect against depressive symptoms. In recent years, researchers have become interested in self-surveillance, social self-esteem, and reliance on external validation as potential moderating variables (Bessenoff and Snow, 2006; Choma et al., 2010). This interest appears to be driven, at least in part, by the notion that these variables may reduce body-related shame and may, therefore, provide targets for interventions developed to limit body-related shame experiences. Therefore, researchers are encouraged to consider these and other potential moderating variables and continue to distinguish between body-related shame and guilt given the observation of unique patterns of associations with depressive symptoms.
This study has limitations that should be addressed in future research. It is not possible to establish temporal sequencing between body-related self-conscious emotions, self-esteem, and depressive symptoms due to the cross-sectional analysis. To test temporal sequencing appropriately, researchers should use longitudinal or experimental study designs. Also, despite having used measures with established score reliability and validity, self-report data could be biased by social desirability or social approval, which could yield biased regression coefficients (i.e. estimates may be over- or underestimated). Finally, the relatively low proportion of non-White young adults in this sample may limit the generalizability of the current findings.
Conclusion
The findings from this study increase the understanding of the associations between body-related self-conscious emotions, self-esteem, and depressive symptoms in young adults. In particular, whereas experiences of body-related shame and guilt were positively associated with frequency of depressive symptoms, the present findings suggest divergent associations for body-related guilt may exist based on young adults’ levels of self-esteem. This study adds to the literature focused on self-conscious emotions and depressive symptoms by demonstrating that self-esteem may attenuate the positive association between body-related guilt and frequency of depressive symptoms among those reporting higher self-esteem. These findings are relevant from both theoretical and practical perspectives. Theoretically, they contribute to an increased understanding of predisposing factors for less severe forms of depression in young adults. Additionally, they provide initial evidence that self-esteem may moderate the associations between certain self-conscious emotions and depressive symptoms. Practically, they point to the potential relevance of including strategies to enhance self-esteem when developing and evaluating the efficacy or effectiveness of interventions aimed at reducing body-related self-conscious emotions to reduce depressive symptoms.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Canadian Cancer Society grant numbers 010271 and 017435 awarded to J.O. This article was prepared while J.B. was supported by a Canadian Cancer Society Career Development Award in Prevention.