
Abstract
Birth satisfaction impacts on a man’s adjustment to his new role as father. Fathers have been found to have needs similar to those of mothers during pregnancy and childbirth. Research suggests that these needs may not be being met for first-time fathers. In a quantitative survey, fathers’ birth satisfaction was similar to mothers. This study then used a phenomenological form of thematic analysis to gain an insight into the birth experiences of 155 first-time New Zealand fathers. Core themes included safety of mother and baby, understanding support role, mother in control and managing pain and care and communication after birth. Fathers commented on what impacted on their childbirth experiences and in so doing outlined their needs for a positive experience. Fathers experienced a high level of satisfaction along with a need to be involved and included.
Keywords
Introduction
Birth of a child is a major event for fathers. Research reveals that the Western World has seen social and cultural shifts in the involvement and presence of fathers. In a qualitative study of what the transition to parenthood meant Barclay and Lupton (1999) concluded that for first-time fathers, becoming a father involved changes in both self-identity and relationship with their partner. In addition, Henwood and Procter (2003) concluded that a father is expected to be caring, nurturing, understanding, approachable and supportive; able to work with his partner as part of a childrearing team; as well as willing to take an active role in the running of the household. Barclay and Lupton (1999) found that men must address complex and evolving emotions as they establish an attachment relationship with their child. This process began with the advent of their partner’s pregnancy followed by the father’s experience of childbirth. While men expressed excitement and joy about the birth of a first child, they also expressed fear about becoming a parent as they felt underprepared and unsure of the expectations their partners may have of their role (Deave et al., 2008; Hildingsson et al., 2014). Hildingsson et al. (2014) surveyed 1047 expectant fathers in Sweden using the Fear of Birth Scale. They conclude that around 14 per cent of men experienced fear, and this was associated with a negative birth experience.
One study interviewed 10 first-time fathers in Sweden and found issues included the father’s excitement tinged with concerns for the safety of the mother and birthing child, the sharing of this experience – his involvement and appreciation of midwife support to be involved, the effect the mother’s ability to cope and his delight in a safe and healthy outcome for mother and baby (Premberg et al., 2011).
In another study, 20 new fathers in England were interviewed, and analysis indicated that fathers had issues similar to those of their partners. These included the need for support mechanisms, more inclusion in antenatal activities and the need for information, including the changes they can expect in their relationships with their partners. Men felt that they were without the support mechanisms available to their pregnant partners, often leaving them feeling isolated, made worse when they were without the role models and guidelines that would have enhanced their journey into fatherhood (Deave and Johnson, 2008).
Before the child is born, men are often stressed because they are unsure of their childbirth role but are driven to be present by their perceptions of cultural expectations (Johnson, 2002). Chapman (2000) revealed that men tended to find it very difficult to cope with the changes they witnessed in their partners during childbirth, as well as with the pain they endured. Labour pain often left men feeling excluded and anxious about what was happening (Deave and Johnson, 2008). Fathers expressed their concern about feeling they had lost their partners to the pain of the labour they were experiencing (Chapman, 2000). Feeling safe has been explored from the perspective of mothers, and this might also be expected to be applicable to fathers (Howarth et al., 2010, 2013).
Deave and Johnson (2008) reported that being involved in the antenatal provisions, being well informed about what to expect during labour and birth, feeling he has a role to play during labour and birth and knowing what it is and feeling he has his own support network dedicated to his needs can enhance a father’s perception of the birth of his child. In an earlier study, Johnson (2002) reported similar findings, meeting these needs can positively influence perception of childbirth and consequently the new father’s relationship with his child.
Using quantitative methodology, Greenhalgh et al. (2000) found that how the father experienced his partner’s labour and birth may be a potential risk factor for the father’s later psychosocial well-being. Fathers who had a positive experience of childbirth were more likely to have no symptoms of depression at 6 weeks postpartum compared to those who had unmet expectations of their birthing experience. Boyce et al. (2007) also found that those first-time fathers who did not have sufficient knowledge and understanding of pregnancy, labour and birth were at risk of feeling psychological distress.
Another recent Swedish study interviewed eight first-time fathers. Their analysis resulted in one major theme ‘a transformative experience’ which had the sub-themes: preparing for childbirth, feeling vulnerable in a new situation, being confirmed as part of a unit and meeting the child for the first time. They conclude that the needs of the fathers should be given more recognition during childbirth.
In a survey of 78 UK fathers, it was found that how men experienced childbirth had a later effect on their emotional well-being (Greenhalgh et al., 2000). Added to this, men were commonly not given the opportunity to talk about their concerns, thus leaving these concerns unresolved (Friedewald et al., 2005). Similarly, Boyce et al. (2007) concluded that providing men with more information regarding pregnancy, childbirth and parenting would be a positive step in assisting these men to overcome their anxieties. Feeling better about their partner’s pregnancy and the birth of their child could assist the father make the transition from couple-hood to family with child and thus encourage him to be a supportive partner (Castle et al., 2008). This, in turn, could assist the mother in her endeavours to develop a sense of herself as an effective and loving mother. Thus, the prospect of quality relationships is enhanced, with the child more likely to develop a secure attachment (Fowles and Horowitz, 2006; Howarth et al., 2011a; Nelson, 2004).
As part of a larger study, 111 Swedish fathers commented on the birth experience, and content analysis was conducted (Johansson et al., 2012). Five categories of response were revealed and named: competence of health-care professionals, professionals approach and involvement in care, experiences of childbirth, expectations about childbirth and the organisation.
Johansson et al. (2015) conducted a meta-synthesis of how fathers experience childbirth. They found only eight studies that met criteria for inclusion: there were four from Sweden, two from England and one each from Malawi and Nepal. This reveals the lack of representative international reports published of father experiences.
This research seeks to provide more evidence about the importance of the role of first-time fathers and provide some reflection on their experiences. A qualitative study seems appropriate as there is still some uncertainty about what is important to first-time fathers witnessing the birth of their babies. Additionally, most published evidence appears to be from Sweden and the United Kingdom, so this article contributes by investigating another health system found in New Zealand.
Method
Data collection approach
This study was part of a larger research project examining the impact of childbirth preparation. Participants recruited were couples expecting their first child. A survey questionnaire was posted to fathers as part of this study.
Participants
A national sample of 155 first-time fathers aged over 18 years commented on aspects of their childbirth experiences. Couples were eligible to participate in this study if they were cohabiting and intended to parent the child together. All participants were sufficiently literate. Various advertising took place, and the participants were required to contact the researcher if they were interested. Once they had contacted the researcher, they all received information and signed consent to participate.
Materials
Participants were recruited using posters, flyers, advertisements and social media. A post-birth questionnaire provided the material for this analysis. Specifically, the Mackey Childbirth Satisfaction Rating Scale New Zealand Adaptation (adapted with permission for fathers) which is a 34-item scale measuring childbirth satisfaction was used (Goodman et al., 2004). Throughout the questionnaire, fathers were asked to write down their thoughts. Additional qualitative data the fathers included with their questionnaires were also included.
Procedure
All participants completed the enrolment documents giving their informed consent for participation in the study. Participants chose to complete either paper or online versions. Ethical approval from the New Zealand Lower South Regional Ethics Committee was gained for this study (reference number: LRS/10/11/052).
Quantitative analysis
Mackey Childbirth Satisfaction Rating Scale New Zealand Adaptation
Birth satisfaction was measured using the Mackey Childbirth Satisfaction Rating Scale (Goodman et al., 2004) New Zealand Adaptation (also adapted for fathers). The 34-item scale contains questions related to the behaviours of self, partner, baby, nurse (midwife) and physicians. A further six questions relate to expectations, whether the experience was positive/negative, and give the opportunity of commenting on the positive and negative aspects of the labour and birth experience. The higher the score, the greater the birth satisfaction.
The Mackey Childbirth Satisfaction Rating Scale (Goodman et al., 2004) was developed for women giving birth in the American maternity system. This required some minor adjustments to adapt it to the New Zealand midwifery-driven maternity system. Consideration was given to differing terminology, for example, the term nurse was altered to midwife. Adaptations to the questionnaires for fathers required wording changes which recognised his role as birth coach. For example, Your overall labour experience became Your overall experience of your partner’s labour for the father’s questionnaire. Permission was requested and given by Mackey to use this scale and make these adaptations.
A summary of responses on the Mackey Birth Satisfaction Rating Scale was created using Excel. Means of subscales were created.
Analytic procedure – phenomenological thematic analysis
A form of phenomenological thematic analysis informed by interpretative phenomenological analysis (IPA) was used to examine the data (Reid et al., 2005; Smith, 1995, 1996; Smith et al., 1999, 2009; Trochim, 2006). Thematic analysis informed by IPA provided a structure within which data could be collated and coded (Braun and Clarke, 2006; Smith et al., 2009). Once the data were entered onto a database, there was an initial reading of comments. Patterns within the data, using information coded across the data corpus, were identified. Data were then organised into meaningful patterns and groups. Data from the transcript of comments that supported each code were briefly summarised. Themes emerged from the summary. Connections between the initial themes were identified and organised into broader themes. Core themes were identified along with related sub-themes, and a pattern of hierarchy became apparent. This process continued until the primary analyst (A.M.H.) felt the themes provided a good overview of the data corpus. A second qualitative data analyst read the comments and independently organised the data into themes. These were discussed with the primary researcher, and an agreement was formed. In the following presentation of results using verbatim quotes, participants are referred to by their study numbers.
Results
Demographic characteristics
Ages ranged from 20 to 49 years with a median of 30.0 years. A total of 66 per cent of fathers were married with the others in de facto relationships. A total of 59 per cent owned their own homes, while 41 per cent were in rental accommodation. A total of 78 per cent had some form of post-secondary qualification. A total of 87 per cent were in full-time employment, 5.2 per cent were students and the others were stay-at-home or unemployed. Approximately 83 per cent of fathers were identified as of European descent and 6 per cent of Maori descent. Approximately 12 per cent of fathers had immigrated to New Zealand in the last 5 years.
An analysis of the fathers’ responses on the Mackey Childbirth Satisfaction Rating Scale was conducted. Results for fathers are presented with three comparison groups. First, mothers in this study and then published data from another study using the same scale. It can be seen that the satisfaction ratings of fathers are similar to those of mothers in this study, as well as internationally. However, satisfaction with physicians appears lower in this sample than in international samples (Table 1).
Mean scores from the Mackey Satisfaction with Childbirth Rating Scale (scores from 1 to 5).
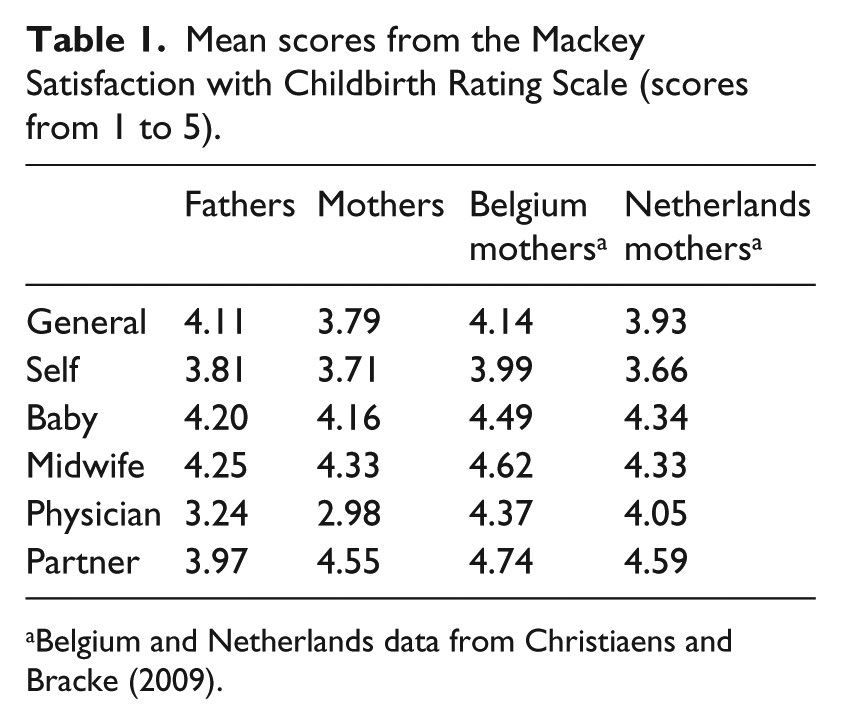
Belgium and Netherlands data from Christiaens and Bracke (2009).
Fathers’ perceptions of their childbirth experiences
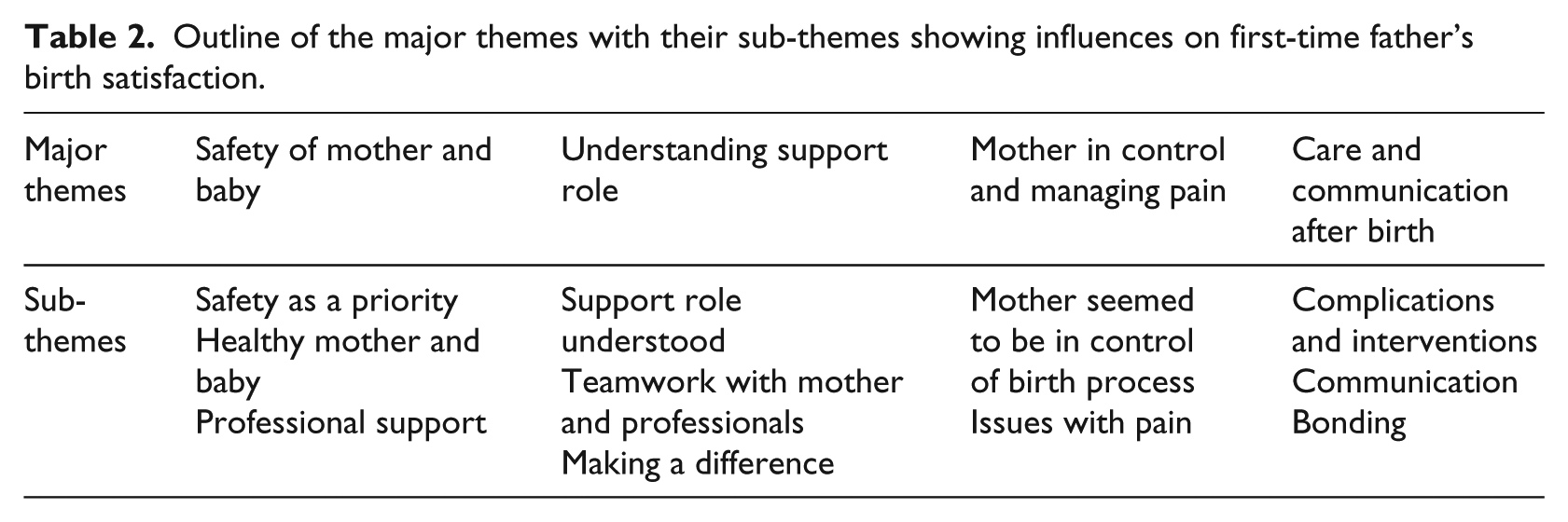
Men reported becoming a father was a life-changing experience (Table 2). Some fathers reported satisfying experiences, while others were so dissatisfied that they made comments such as
Outline of the major themes with their sub-themes showing influences on first-time father’s birth satisfaction.
Don’t think I will be present for any future children’s birth. (005)
Theme 1: safety of mother and baby
For fathers, safety was a primary concern. To facilitate safety, fathers wanted to ensure the best possible care. This involved professionalism from maternity health caregivers and a safe and controlled birth environment.
Safety as a priority
Fathers were aware that complications during labour and birth could, and did, arise. They expressed caution and concern:
My plan was to ensure mum and baby were kept as safe and comfortable as possible during the process. (099)
Fathers wished to ensure that the mothers were getting the best care available. This involved the professionalism demonstrated by the lead maternity carer and other medical professionals (obstetricians, registrars, anaesthetists, nurses and hospital midwives most commonly mentioned) and the perceived safety of the environment in which the birth was planned to take place; that is, mothers were giving birth in what the partner perceived to be a safe and controlled environment. When these conditions were met, the father expressed his satisfaction. Underlying the joy at a good outcome was the relief felt that mother and baby had come through safely as reflected in the following comments:
[the mother] survived the experience … was not how we planned but mum and baby alive and […] well and looked after well by hospital staff. (053)
Healthy mother and baby
Fathers were concerned both for a healthy baby and that the mother came through unscathed and in good health. When either mother or baby suffered health complications, the father was alarmed and apprehensive, and his satisfaction was inhibited:
Didn’t enjoy it at all. Lots of worry about her and the baby … seeing the baby pretty dormant when she came out. (066) [I was] very dissatisfied as we had quite a wee shock when he came out, firstly he had his cord all wrapped around him and then he stopped breathing after he came out. (043)
When things went well, fathers expressed their satisfaction:
Little one and partner were healthy in the end, so it was a win. (042) Very happy that she was healthy … Happiest moment ever. (187)
Staff professionalism was described when individuals demonstrated a high knowledge base, a high level of skills and the competence to use these appropriately for each individual circumstance. Fathers also felt greater confidence in the professionalism of midwives and medical staff when they worked well together as a team, when they were prepared to call in someone more knowledgeable if the situation warranted and if they communicated well. They made comments such as
Dedicated midwife; Special mention to the sound reaction by the obstetrician once the baby’s heart rate started increasing. I was very impressed by how well managed the c-section was […] and how well we were looked after. (122) Excellent. Our experience ended up being very ‘medical’, however everyone – including the anaesthetist and registrar – were very personable and relaxed. (042)
Not all fathers felt their carers demonstrated professional behaviours, and this left them distressed and concerned for the well-being of their loved ones. They were dissatisfied with this aspect of their experience of the birth of their babies and expressed their concerns accordingly:
The midwife put her own interests first, didn’t provide the care we expected […]. Once baby was born the midwife was angry and was most interested in getting home. (172) Hospital staff were terrible, unhelpful, left us feeling very alone and unsure of what to do. (128)
Theme 2: understanding support role
Support role understood
Fathers wanted to feel included and involved in the mother’s labour, especially if complications occurred and plans had to change with new decisions, often unexpected, to be made. Those who felt included and involved expressed their satisfaction, while those fathers who felt excluded were dissatisfied and felt that their experience of the birth of their child had been compromised:
I asked my partner if she had asked the midwife to call me of which she stated that she had asked the midwife many times to call me and she always had an excuse to not do so … The midwife totally destroyed the experience for both of us. (111)
Those fathers who established their role in the mother’s labour and delivery of their child and prepared themselves accordingly or who simply found themselves responding positively to the labour and birth reported greater satisfaction:
I didn’t want to be very involved beforehand, but when it all started, it was just me in there with the midwife, so I ended up getting a lot more involved than I had wanted to, but it was great. (043)
than those partners who found themselves wanting to have a role to play but having no idea what it was and consequently feeling helpless:
[I] didn’t really know what to say or do, bit stunned. (185)
Teamwork
Those fathers who felt themselves included/involved commented on the sense of teamwork they experienced working with the mother to assist her to give birth to their child. This sense of teamwork, along with feeling included/involved, enhanced the family bonding process:
Wonderful feeling of teamwork and bonding between us. (051)
When the midwife and other medical professionals facilitated the fathers’ ability to support and encourage the mother, they felt a greater sense of satisfaction even when they had not initially known what their role was. Those who received advice and guidance from their professional felt that they were better supporters:
She [midwife] encouraged me and advised where the best place to be was in each situation, and really encouraged me to be part of it. (152)
When the father felt confident that he had made a difference by offering his support and encouragement to the mother he was filled with a sense of satisfaction with both himself and his overall experience of the birth of his child:
I coped far better than I thought – probably because the nerves got pushed to the background as I focused on the moment and I felt I was helping. (038)
Theme 3: mother in control and managing pain
Mother seemed in control
When the father perceived the mother to be coping, his anxiety was reduced and he felt less distress. This carried through to situations where medical interventions became essential. If the father perceived her to be handling the situation, his sense of satisfaction with the birthing process was enhanced, as was his admiration for the mother and he commented on
how well she coped throughout. Although she was clearly in a lot of pain she made it through by focusing on herself and was able to still make good decisions and was open to assistance from myself and the midwives. (038)
Fathers were sensitive to the manner in which mothers managed their birthing process. If mothers were perceived as being in control of their body and decision-making, the father felt greater satisfaction with his experience too. They also felt pride in her achievement and admiration for their partner and expressed in comments such as
The way my wife handled herself was second to none. I was so proud of her. She could not have done any better. (103)
Issues with pain
The father felt a sense of relief when the mother was able to manage the pain using the strategies she had selected and not become overwhelmed and distressed. They also felt admiration and pride in her achievement, and this enhanced the fathers’ sense of satisfaction:
Partner did very well managing her pain as much as she could. (005)
Fathers found it difficult seeing the mothers in pain, especially when over a prolonged period of time and when they felt helpless to do anything to relieve that pain. They reported less satisfaction with their experience of childbirth:
Probably one of the most harrowing experiences of my life to see and hear someone I love in that much pain and to be so helpless to do anything about it. (053)
The father felt happier when she managed to give an impression that she was not experiencing too much pain or when she was given medication to make the pain more tolerable:
One of the perks of having an epidural is not having to see your partner in pain. Despite wanting minimal medication, the epidural was unplanned, it was awesome and nice that my partner had no pain throughout the labour. (181)
Theme 4: care and communication after birth
Complications
The birth itself contributed towards the father’s satisfaction/dissatisfaction. Fathers hoped that the mother would experience a short labour which was not too painful and that the birth would be easy and without complications. For some fathers, this was the case, and it led them to make the following comments explaining why they experienced satisfaction:
It was a lot easier for her (and for me) than I expected. (092) My partner was cool, calm and collected; medical interventions were avoided; process went smoothly. (061)
Not all couples experienced a complication-free birthing process, with medical intervention becoming a necessity for some. Fathers did not want to see their partners develop such complications during labour and birth. When unexpected complications did develop, fathers were disappointed and could find these scary and distressing. If the mother was distressed, then it became even harder for the father to cope, and his satisfaction with the birth of his baby was diminished:
It was wrenching when the ventouse proved insufficient to turn the baby and a caesarian was required. […] The whole experience was horrific at the time. (040) [I felt] an emptiness, indescribable. [Mother] drugged up, unable to get baby out, on an operating theatre, awake for 25 hours, had to let the delivery occur in control of 13 people. (005)
Fathers said that they needed support, explanation, acknowledgement and reassurance and to feel that their humanity was recognised. When these needs were met, what initially was both frightening and a major disappointment had the potential to reduce the mother’s distress and calm her which consequently increased the father’s satisfaction with his birth experience:
[Was a] successful outcome in the end; competent staff gave me confidence even when medical issues arose; midwives mostly friendly and conscientious […] when needed doctors were fantastic and reassuring [ventouse delivery]. (053)
Communication
Keeping parents informed of how the birthing process was progressing was important for all couples but became particularly so when any complications occurred. In some instances, parents were not only uninformed but were excluded for the decision-making process, or doctors pressed them to agree to decisions they were not altogether comfortable with. Fathers were protective of mothers and were dissatisfied if they felt they were not being treated with empathy. Conflicting opinions aired in front of parents were also disturbing as were staff who did not communicate well with each other or the parents. Such experiences left fathers expressing their dissatisfaction with comments including
You can really feel left out of decision making in hospital especially when things go wrong … anaesthetist was great but OB registrar not so forthcoming with thoughts or letting us know what was going on. (053) Once the specialists took over Partner and I were not included in any decisions. (095) 3 groups were disagreeing/stressed (2 midwives, NICU, emergency team). (120)
Other couples felt that they had been kept very well informed by midwives and other medical professionals and that they were able to understand what was happening and take part in decision-making processes. And if that was not possible because of an emergency situation, they were appropriately debriefed afterwards. Fathers expressed their satisfaction, even when the actual experience might have been difficult:
We were both well informed during each step and I felt our midwife and others provided information fast and clearly which kept us both with the feeling that things were well under control. (099) [There was] great communication by medical staff during the birth. (040) [There was] no time for consultation but talked to us after. (177)
Bonding
Seeing baby finally arrive was a very special moment for both parents:
Then finally seeing the baby come out when he was almost there was very amazing. (043) Seeing my baby for the first time and knowing what we have been waiting for. (134)
Once baby was born, fathers were excited that they could finally hold their baby for the first time. However, fathers, while wanting to hold the baby as soon as possible, were also concerned that the mothers got the opportunity. Fathers also expressed satisfaction with their part in the first moments of baby’s life when they had the opportunity to cut the umbilical cord. Fathers also expressed satisfaction with their part in the first moments of baby’s life when they had the opportunity to cut the umbilical cord. Comments such as the following conveyed this satisfaction:
He got loads of skin on skin with his mum which was lovely. (184) [I] wasn’t sure if I wanted to cut the cord but was fine at the time and really glad I did. (93)
When fathers assisted with delivery and/or got the opportunity to hold baby for the first time, it was a very special moment for them, and they expressed their satisfaction with their experience:
Due to partner needing to be taken to theatre I was given Baby for skin to skin within 15 minutes of her being born and [I] cuddle[d] her for over 3 hours until partner was brought back. (181)
Sharing this journey of birth had the capacity to bring couples closer together and strengthen relationships. The time together with the baby immediately after the birth was important:
Our relationship is much stronger for having survived the experience. (053) Difficult journey but overall helped me appreciate and love my wife more for it. […] The chance to deliver my son helped with bonding process. (034)
New families wanted the space and privacy to begin adjusting to this life-changing event. When hospital facilities were inadequate to support, the continuation of this process distress was caused. Fathers were unhappy if mothers were transferred soon after birth to wards that meant room sharing with other new mothers. The following father clearly expressed the emotional impact being separated from his new family so soon after the birth had on him:
[It] was heart breaking when they said I couldn’t stay the night. I had been with her that whole time and suddenly I had to go. (027)
Discussion
Fathers in this study recognised that the birth of their child was a life-changing event for themselves as well as mothers. Birth satisfaction has been identified as a key element affecting fathers’ as well as mothers’ psychosocial well-being (Boyce et al., 2007; Castle et al., 2008; Deave and Johnson, 2008; Fenwick et al., 2012; Friedewald, 2007; Greenhalgh et al., 2000; Longworth and Kingdon, 2011; Lothian, 2008). Fathers in this study were clear about what enhanced their satisfaction with their birth experience and what did not. Their experiences provide an understanding of what the fathers felt they needed.
Interestingly, quantitative results from the Mackey Childbirth Satisfaction Rating Scale show fathers feel similar to mothers about childbirth satisfaction. The participants in this study were also similar to those surveyed internationally. Ledenfors and Berterö (2016) report that fathers are generally satisfied with the birth experience despite feeling like an outsider. They attribute this to feelings of gratitude and relief. Notably, the New Zealand sample was less satisfied with medical assistance than other countries, but this could be an artefact of the midwife-led system in New Zealand. Birthing mothers will only need to see medical staff when complications arise, which may lead to lower satisfaction rating of the medical staff.
In this study, the safety of mother and baby, as found by Premberg et al. (2011), was understandably of greatest of concern for the father. When fathers perceived that staff professionalism was ensuring, the mother and baby were getting the best care suited to their situation they expressed greater birth satisfaction than those fathers who perceived the care the mothers and/or babies got was inadequate. This finding supports research suggesting fathers’ concerns about safety need to be treated respectfully and empathetically (Johansson et al., 2012). Fathers helped to decide whether hospital or home was a safe option for delivery of their baby and confidence in this decision added to feelings of safety. This is similar to the Swedish study by Johansson et al. (2012) where a theme that emerged was competence of health-care professionals and encompasses similar concerns of professionalism of staff and medical care of partner. A healthy baby and healthy mother was understandably the outcome desired by all fathers, supporting the finding of Premberg et al. (2011). As Johansson et al. (2012) found, anything that threatened that outcome created stress that detracted from the perception of the whole experience for fathers in this study.
Fathers expressed satisfaction with their experience when they understood their support role. Previous research has found being included may reduce the risk of post-traumatic stress disorder for fathers following a traumatic birth (White, 2007). When the father perceived that he had really made a positive difference to the mother’s experience of labour and childbirth, he expressed greater satisfaction than those fathers who struggled to feel included and involved. These results find support from another study by Longworth and Kingdon (2011) who found men struggled to find their role in childbirth. Hildingsson et al. (2011) also reported that support from the midwife was an important factor reflecting fathers’ birth satisfaction. Johansson et al. (2012) reported several themes related to this including support by midwives, information received, treatment of father with respect and empathy and to be involved.
Mother in control and managing pain, the third theme to emerge from the data. This was similar for the participants in the Premberg et al. (2011) study. When fathers perceived that the mother felt in control of her process and that she was managing her pain effectively, he felt comforted. For the father, seeing the mother in pain was difficult and made worse when she was perceived as being overwhelmed and distressed. In their recent meta-analysis, Johansson et al. (2015) found that men particularly struggled with the pain of labour. Deave and Johnson (2008) reported that the father often felt excluded and helpless when the mother was focused internally. Poor management of pain led to lower satisfaction. This sense of satisfaction was increased when the father felt that he played a positive support role which encouraged and valued her efforts. As Chapman (2000) also found, those fathers who struggled and whose partners were given epidurals felt relief which contributed towards their sense of birth satisfaction.
Care and communication after birth was a major area of satisfaction for fathers. Typical of findings in other studies, fathers appreciated being informed that progress was normal (Hildingsson et al., 2011; Johansson et al., 2012). When complications arose and interventions were required to ensure the safety of mother and baby, fathers became anxious and worried. Medical personnel who kept the parents fully informed and welcomed their input when decisions had to be made helped with anxiety and adaptation to changes, a finding consistent with other research (Howarth et al., 2012; Johansson et al., 2012, 2015).
Fathers wanted to be able to see their new baby and hold their new baby as soon as possible. Delays because of complications were distressing and again impacted negatively on the satisfaction they felt with the whole process. Fathers also wanted to be a part of the bonding process between parents and child. When hospital accommodation resources were inadequate, so that they were forced to leave the mother and their baby before the family felt ready to part, distress was experienced by the fathers.
Taken together, these data suggest possible improvement to the maternity system which would help fathers feel greater satisfaction. Preparation is seen as a key part of experiencing birth satisfaction (Howarth et al., 2011b), perhaps more attention could be given in antenatal classes to the role of the father in delivery. Green (1999) suggests that preparation is a key area of concern for fathers who felt helpless when they did not know what they could do to assist their partners during labour and birth.
Limitations
Qualitative studies are exploratory with a number of known weaknesses including researcher bias, lack of generalisability and response bias. This study was limited to first-time fathers. Fathers who are having subsequent children may have different perspectives of the birth experience. There was little representation from socio-economically deprived groups in this study which would add a different perspective. Redshaw and Henderson (2013) reported a considerable socio-demographic variation in partner support in a large UK study. The New Zealand childbirth environment may be unique in a number of ways: there is a high level of immigration, a midwife-led system and free maternity services. Each of these factors may have a unique contribution to opinions held by this group of first-time fathers.
Conclusion
In common with other Western countries, more and more fathers are becoming an integral part of the childbirth process in New Zealand. How they experience the pregnancy and birth of their child may impact their psychological well-being (Fenwick et al., 2012; Friedewald, 2007; Longworth and Kingdon, 2011). Fathers in this study report high levels of childbirth satisfaction, despite reporting some concerns. Issues identified as relevant to fathers experience need to be prioritised in birthing care. This article suggests that many of these issues are about care and safety of mothers but also a strong need to be involved and included as participants in this process along with the birthing mothers. The findings in this study give a deeper understanding of the father’s experience of childbirth.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Preparation of this article received the support of the Graduate Research Committee, by means of the University of Otago Postgraduate Publishing Bursary (doctoral).