
Abstract
Emerging adults are at high risk of obesity but behavioral weight loss programs do not meet their needs. Emerging adults (N = 52, age = 22.3 ± 2 years, body mass index = 34.2 ± 5.5 kg/m2, 46.2% non-Hispanic White) were randomly assigned to one of three behavioral weight loss programs adapted based on formative work: face-to-face behavioral weight loss, web-based behavioral weight loss, or web plus optional community sessions (Hybrid). Assessments occurred at 0 and 3 months. Engagement and self-monitoring were highest in Hybrid. Intent-to-treat weight losses were −2.8 ± 2.9 percent in face-to-face behavioral weight loss, −2.2 ± 4.5 percent in web-based behavioral weight loss, and 4.8 ± 4.9 percent in Hybrid. Percent achieving ⩾5 percent weight loss was highest in Hybrid (63%). Findings suggest potential for adapted behavioral weight loss to promote engagement and weight loss in emerging adults.
Over 40 percent of emerging adults aged 18–25 meet criteria for overweight or obesity, with rates exceeding 50 percent in African-American and Hispanic/Latino populations (Muyle et al., 2009). Furthermore, obesity during these years is associated with increased risk of diabetes, hypertension, and hyperlipidemia (Merten, 2010). Despite being at substantial risk, emerging adults are markedly underrepresented in adult behavioral weight loss (BWL) programs, representing less than 1 percent of participants enrolled in National Institutes of Health (NIH)-funded adult BWL trials (Gokee-LaRose et al., 2009b), and recruitment of this population has been noted as a challenge (Gokee-LaRose et al., 2009b; Loria et al., 2010; Poobalan et al., 2010). Furthermore, data indicate that the small number of 18- to 25-year-olds who do enroll in standard programs do not fare as well as their adult counterparts, as evidenced by poorer engagement, retention, and weight losses (Gokee-LaRose et al., 2009b; LaRose et al., 2012). In fact, this age group in particular fares worse even relative to young adults (i.e. up to 35 years), with some studies noting retention of 18- to 25-year-olds to be as low as 25–33 percent within the context of adult weight loss programs (Gokee-LaRose et al., 2009b; LaRose et al., 2012). Evidence-based BWL programs exist for pediatric (Raynor, 2008), adolescent (Delamater et al., 2008), and adult (LaRose and Wing, 2011) populations, but an evidence-based gold standard does not exist for emerging adults despite data suggesting that extant adult programs are not meeting their needs.
In recent years, the importance of developing weight control approaches for young adults has been documented (Loria et al., 2010) and work has begun to emerge in this area. Several small pilot studies have been conducted for weight loss in young adults, including those with college students 18–29 years of age (Napolitano et al., 2013) and a community sample of young adults 21–35 years of age (Gokee-LaRose et al., 2009a), both of which documented promising short-term outcomes. Additionally, NIH funded a consortium of trials (www.earlytrials.org) focused specifically on weight control during young adulthood, defined as 18–35 years (Lytle et al., 2014b). While primary outcome papers are not available yet for most of these trials, they will address an important gap in the literature as they represent the first intervention designed specifically for young adults and have already contributed to our knowledge about how to recruit and promote engagement in young adults (Crane et al., 2016; Gupta et al., 2015; Merchant et al., 2014; Tate et al., 2014). However, many of the Early Adult Reduction of weight through LifestYle intervention (EARLY) trials focus on prevention of weight gain as opposed to weight loss (Lytle et al., 2014a; Wing et al., 2016). Of the EARLY trials targeting weight loss in a broader sample of 18- to 35-year-olds, intensive in-person treatment demonstrated clinically meaningful weight losses at 6 months (Jakicic et al., 2015), while technology-delivered approaches have demonstrated limited success (Svetkey et al., 2015). Of note, there is a relative dearth of existing trials focused on weight loss specifically for 18- to 25-year-olds, with enrollment limited to individuals in this age range.
Given developmental considerations and evidence that emerging adults aged 18–25 years fare even worse than young adults, efforts to target 18- to 25-year-olds in particular appear warranted. In fact, researchers have argued that programs should be designed specifically to target health issues during this period in the lifespan (Furstenberg, 2006; Park et al., 2006). Emerging adulthood is marked by an increased emphasis on gaining autonomy and assuming responsibility for one’s own choices, as well as significant role transitions that are generally accompanied by changes in the social and physical environment (Arnett, 2000). Extant data also indicate this transition is associated with a host of unhealthy weight-related behaviors, including sharp declines in physical activity (Gordon-Larsen et al., 2004), increased sedentary behaviors (Sidney et al., 1996), increased consumption of fast food (Duffey et al., 2007; Niemeier et al., 2006), and sugar-sweetened beverages (Huffman and West, 2007). Additionally, documented high rates of perceived stress (Arnett and Schwab, 2012), depression (Karg et al., 2014), and substance abuse (Muyle et al., 2009) during emerging adulthood signal that this is perhaps a critical time for intervention to promote healthy lifestyle behaviors.
Indeed, it makes sense that a BWL protocol for adults would need to be adapted to meet the needs of emerging adults. Yet, BWL programs developed specifically for 18- to 25-year-olds are lacking (Poobalan et al., 2010), and limited data exist to inform the development of such a program other than a formative study focused on physical activity and conducted in the United Kingdom (Poobalan et al., 2012). As such, we conducted formative work with 18- to 25-year-olds with overweight or obesity to guide our efforts in this area (LaRose et al., 2016). Findings suggest that to appeal to this population, programs should be brief and delivered using a hybrid format with some in-person contact augmented with a technology platform. Furthermore, data indicate that individual-level coaching and a focus on more comprehensive lifestyle change (e.g. stress, fitness, time management) may be key methods for facilitating program engagement. Moreover, data reflect the need to promote autonomy and provide flexibility and choice, allowing participants to individualize the program based on their needs and preferences. These findings are consistent with an increased desire for autonomy that is characteristic of the transition into young adulthood (Arnett, 2000) and underscore the need to adapt existing programs to better meet the needs of this age group.
We developed an adapted version of BWL specifically for emerging adults 18–25 years of age. Adaptions were made to content and contact type (i.e. including more opportunities for individual-level coaching). In addition, we sought to assess the utility of delivering this adapted BWL program via different modalities (in-person, web, or hybrid). To fully integrate the findings of our formative work, the hybrid delivery arm was further informed by self-determination theory (SDT, Ryan and Deci, 2002) and was designed to promote greater internalization and integration of behavioral goals, with a particular emphasis on facilitating autonomy and choice. The goal of this study was to determine the feasibility, acceptability, and preliminary efficacy of the adapted BWL program to inform future efforts in this area. Given data to suggest that if 18- to 25-year-olds can be retained, and clinically meaningful weight losses can be achieved (LaRose et al., 2012), the primary aim of this study was to establish feasibility of engaging and retaining this high-risk age group. Secondary aims were focused on the ability of the approaches tested to promote clinically meaningful weight losses.
Methods
Participants
Participants were recruited using digital and print advertisements, radio spots, email blasts, listservs, and flyers. Inclusion criteria were as follows: (1) age, 18–25 years; (2) body mass index (BMI) of 25–45 kg/m2; (3) regular Internet access; (4) English speaking; and (5) willingness to be randomized to any of the arms. Exclusion criteria included (1) uncontrolled medical condition that would pose a safety risk with weight loss or unsupervised exercise (e.g. uncontrolled hypertension); (2) current or planned use of weight loss medications or participation in another weight loss program; (3) reported heart condition, chest pain, or loss of consciousness on the Physical Activity Readiness Questionnaire (PAR-Q); (4) psychiatric hospitalization in the last 12 months; (5) pregnancy, lactation, or plans to become pregnant during the study period; (6) weight loss of >5 percent within the previous 6 months; (7) reported history of or current eating disorder. Participants who reported medical conditions that could interfere with their ability to safely complete the intervention were required to obtain written MD permission to participate.
Procedures
Recruitment procedures and materials were guided by our formative work with this population (LaRose et al., 2016). In brief, recruitment messages were positive and gain-framed, focused on overall lifestyle change as opposed to solely on weight loss, and emphasized personal volition and the active nature of behavior change. A study name, logo, and tag line were developed, which were used across all ads to enhance branding and name recognition, as well as connection to the local community. Furthermore, messages explicitly stated that the program was developed specifically for 18- to 25-year-olds and used the age range instead of the terms “emerging adults” or “young adults” to be responsive to our formative data. Additionally, we employed a multi-method recruitment plan that included a wide range of outlets (e.g. radio, email, listservs, digital media, flyers, and brochures, as well as word of mouth) and included both active and passive methods. All materials included the web address for a recruitment web site (in addition to a phone number). The recruitment website provided details about the study and was accessible to participants at any time so they could learn more at their convenience. Interested participants were able to link directly from the recruitment website to a secure platform and complete a pre-screening questionnaire to determine their initial eligibility for the program so as to reduce time and motivation barriers and minimize the need for phone contacts. Individuals who appeared eligible were invited to attend a group orientation where the details of the study were described in greater depth and informed consent was obtained. Those who signed consent were scheduled to complete their baseline assessment visit. All participants who completed baseline visits and remained eligible based on in-person screening were eligible for randomization. Procedures were approved by the Virginia Commonwealth University Institutional Review Board.
Study design
Participants were assigned with equal probability within gender using a variably sized permuted block randomization to one of three conditions: face-to-face behavioral weight loss (FBWL; N = 17), web-based behavioral weight loss (WBWL; N = 17), or Hybrid-format behavioral weight loss (Hybrid; N = 18) (see Figure 1). Intervention was delivered weekly for 3 months. There was no treatment contact of any kind during months 3–6. Assessments occurred at 0 and 3 months, with a weight-only visit at 6 months. Participants received $25 for completing the 3- and 6-month visits.
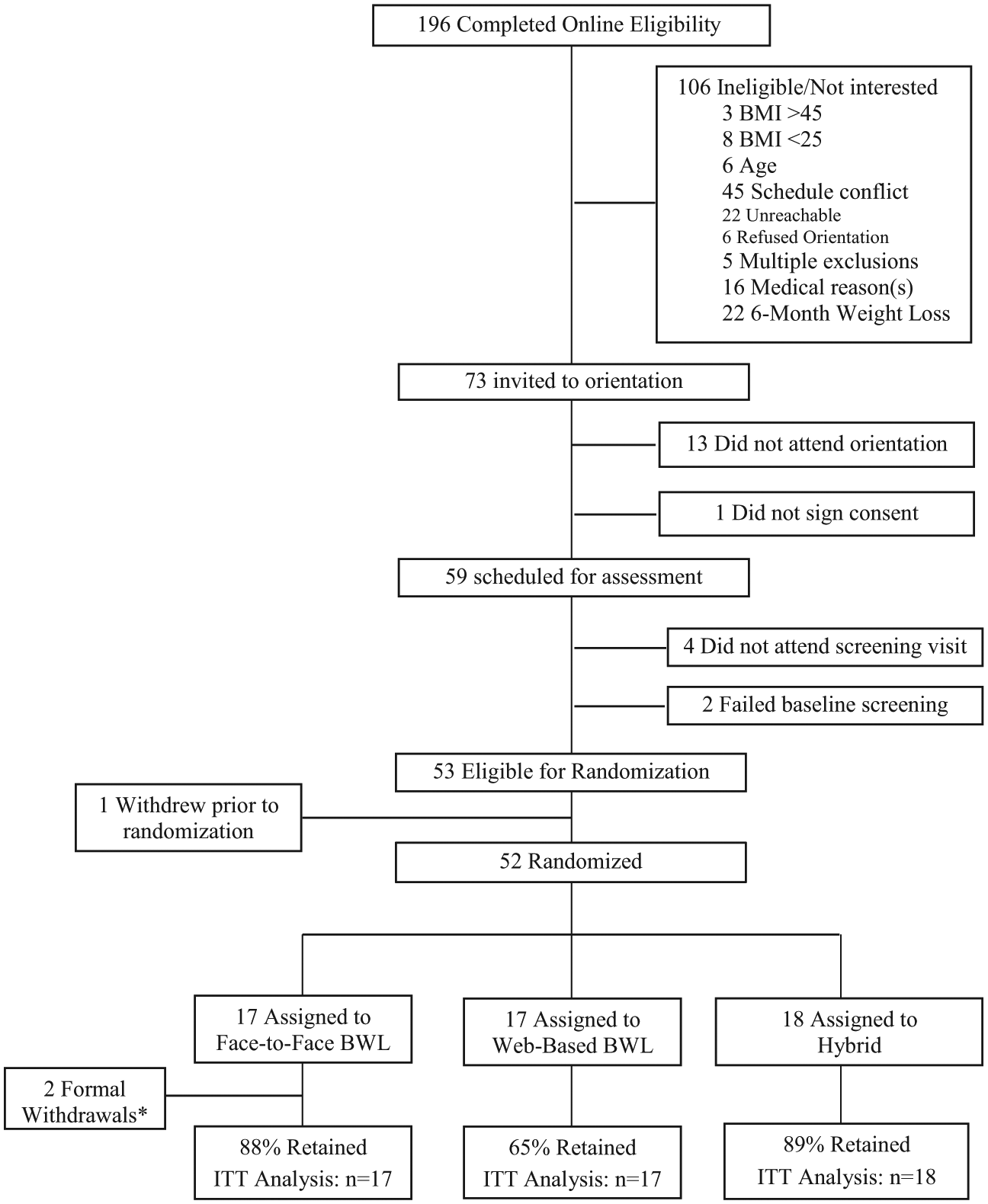
Participant flow.
Description of interventions
Components common to all conditions
Lesson content
Content was identical across groups. Participants received 12 weekly lessons consisting of evidence-based BWL content (Diabetes Prevention Program (DPP) Research Group, 2002; LaRose and Wing, 2011) adapted to emphasize goal setting and behavior change surrounding high-risk weight-related behaviors in emerging adulthood (e.g. alcohol, fast food, and sugar-sweetened beverages). These lessons have been used in our previous work with 18- to 35-year-olds (Gokee-LaRose et al., 2009a; LaRose et al., 2010) and were further adapted for this study based on our formative work to better meet the needs of emerging adults with 18–25 years of age (see Table 1).
Weekly lesson topics for the adapted BWL protocol in all conditions.

BWL: behavioral weight loss ; Traffic Light Diet: TLD.
Content added to address challenges and preferences identified by emerging adults in our formative work.
Behavioral goals and strategies
Participants received personalized calorie and fat goals based on starting weight designed to produce a 1–2 pound/week weight loss with a target of 5 percent weight loss during the 3-month program. Participants were instructed to self-monitor weight, calories, fat grams, and minutes of physical activity in an effort to meet weight loss goals. Participants were taught to consume a diet low in saturated fat and energy density (Ello-Martin et al., 2005) and received education on Traffic Light diet (Epstein et al., 1984; Temple et al., 2011) as a framework to assist them in increasing consumption of “go” foods. Participants were also encouraged to work toward a goal of 250 minutes/week of moderate-intensity physical activity, with weekly goals accumulating based on their baseline level. Core behavioral strategies that form the basis of BWL programs (DPP Research Group, 2002; LaRose and Wing, 2011) were taught to promote modification of diet and activity behaviors and assist the participants in meeting their goals (e.g. self-monitoring, stimulus control, and goal setting).
Interventionists
Two doctoral students in clinical psychology with training in BWL served as the “coaches” and were supervised by a clinical psychologist with expertise in the content area. Coaches delivered treatment across all arms; group sessions were team led and within each arm participants were randomly assigned to one of the two coaches for all individual check-ins and weekly e-coaching.
Personalized feedback on progress
Participants submitted their self-monitoring data weekly during the 3-month program for review by their coach and received personalized feedback on their progress and coaching to assist them in meeting goals. Feedback was focused on goal attainment and progress, noting specific behaviors (e.g. self-monitoring) and outcomes (e.g. weight loss), and encouraged core behavioral strategies including goal setting and problem solving. Participants were encouraged to email their coach with questions, but it was not the expectation that participants would respond to their feedback message. Although provided by live coaches and personalized, the structure of the feedback was intentionally such that it was consistent in format, content and length, and could be automated in future trials. Those participants who did not submit data were prompted to do so by their coach and reminded of the importance of the positive relationship between self-monitoring and weight loss. During the no-treatment contact follow-up period (i.e. 3–6 months), participants were encouraged to continue healthy lifestyle behaviors and self-monitoring, but did not turn in diaries, no feedback was provided, and there was no communication with intervention staff.
Intervention components that differed between conditions
A description of the differences across intervention arms is provided in Table 2. In short, the Hybrid arm was developed in response to our formative work and informed by each of the core psychological needs outlined by SDT, with a particular emphasis on autonomy and choice to promote internalization of behavioral goals (Table 3). The Hybrid condition consisted of a web-based platform with weekly e-coaching and optional competency-building group sessions. The optional groups were offered once per week and varied in terms of their focus on diet or physical activity—activity classes included circuit training, kickboxing, and yoga, whereas the nutrition classes were hands-on cooking skills and prep as well as tastings with recipes. All classes were experiential in nature and offered in order to promote practice of the skills taught in the program; new intervention content was not presented. Groups were led by community partners in existing community settings, but intervention staff attended to promote relatedness. Additionally, weekly feedback messages provided feedback on behaviors, goal attainment, and progress in an autonomy-supportive fashion, emphasizing one’s choice and volition (e.g. By choosing to keep track of your diet every day this week, you’re in the driver’s seat and are making fantastic progress toward your goals!). FBWL was the closest approximation to adult BWL and involved weekly group-based, in-person treatment sessions and bi-weekly individual check-ins. WBWL received an identical program to FBWL but delivered online. WBWL was modeled after previous web-based BWL protocols (Tate et al., 2003, 2006) and consisted of one group-based session to provide an overview of BWL and the web site, followed by a web-based program including weekly lessons, a self-monitoring platform, and weekly e-coaching.
Differences across intervention conditions.

BWL: behavioral weight loss; FBWL: face-to-face behavioral weight loss; WBWL: web-based behavioral weight loss; SDT: self-determination theory.
Self-determination theory components in Hybrid condition.

Implementation and fidelity monitoring
As noted above, interventionists had relevant experience and skills and were trained and supervised by a clinical psychologist with expertise in BWL and the adapted protocol. Manuals were developed for in-person sessions and a protocol was developed for e-coaching to standardize contact frequency and content. Sessions were audio-recorded and e-coaching messages reviewed; a fidelity checklist was used during weekly review to ensure topics were covered as planned, that interventionists delivered the material with competence and skill, and that no protocol deviations occurred. The intervention team met weekly for supervision to ensure fidelity to the protocol and address any barriers or implementation questions as they arose. Intervention fidelity was excellent, with 100 percent of in-person sessions delivered as intended with all major topics presented with high competence by the coaches. Similarly, 100 percent of feedback messages were provided as intended, with core elements included in all messages and a high degree of interventionist skill and competence.
Measures
Assessments were completed by blinded assessors trained in study procedures. Measures were obtained at 0 and 3 months, unless otherwise noted.
Demographics
At baseline, participants reported gender, age, race and ethnicity, and school status.
Height, weight, and BMI
Height was measured at baseline only to the nearest millimeter using a wall-mounted stadiometer and a standard protocol. Weight was measured to the nearest 0.01 kg in light clothes without shoes using a calibrated digital scale at 0, 3, and 6 months. BMI was calculated as weight in kilogram/height in square meters. Percent weight loss was calculated as follows: ((post-treatment weight − baseline weight)/baseline weight) × 100. Percent weight loss (as opposed to change in kg) was used as it accounts for participants’ baseline levels; parallel analyses were conducted to examine change in participants’ BMI.
Engagement
Attendance at sessions (FBWL and Hybrid), lessons viewed (Web and Hybrid), and self-monitoring (percentage of weeks self-monitoring diaries/data were submitted in all arms) was tracked.
Diet and physical activity behaviors
Items used in our previous studies (LaRose et al., 2010; Wing et al., 2016) were administered that asked participants to report on key dietary behaviors (fast food, sugar-sweetened beverages, breakfast, and alcohol); these behaviors were explicitly targeted in intervention content and have been associated with weight gain in emerging adults. Paffenbarger et al.’s (1978) Physical Activity Questionnaire was used to assess total minutes of physical activity; it has satisfactory reliability and is sensitive to change in intervention studies (Paffenbarger et al., 1978).
Acceptability
Participants reported overall program satisfaction and whether they thought the program would be relevant to others their age interested in weight loss.
Statistical analyses
We conducted all analyses using IBM SPSS Statistics for Windows, Release 20.0.0 (IBM Corp.©, 2011, Armonk, NY, www.ibm.com). We first conducted descriptive analyses to test for any group differences on baseline demographic characteristics and all baseline values of dependent variables using analysis of variance or chi-square tests for continuous or categorical variables, respectively. Given that the primary aims of this pilot trial were feasibility as evidenced by the ability to engage and retain emerging adults, pre-specified thresholds were established to determine feasibility in each of these areas. Based on our previous pilot work (Gokee-LaRose et al., 2009a; LaRose et al., 2010) and insights from our ongoing long-term weight gain prevention trial with a broader age range of young adults (Wing et al., 2016), we specified 70 percent retention at post-treatment and 70 percent attendance and weight reporting as the thresholds to determine the approach was potentially viable. Secondary analyses focused on weight change were conducted across all groups, with effect size estimates provided to guide future studies (Cohen’s f). Primary weight change analyses used an intent-to-treat (ITT) approach to compare the three groups on percent weight loss wherein non-completers were assumed to have remained at their baseline weight. Moderator analyses were also conducted to examine for any race effects (non-Hispanic White vs other races) to determine whether race should be controlled for in the final analyses. Secondary analyses were conducted using only those participants who were retained (i.e. completers). Parallel analyses were conducted on BMI change for both ITT and completers as a secondary assessment of weight change.
Results
Recruitment yield
Recruitment procedures resulted in a total of 196 individuals completing the web-based pre-screen within a 2-month period, 90 of whom appeared eligible based on initial screening (see Figure 1 for participant flow through randomization); 26.5 percent of all initial pre-screens (and 58% of eligible pre-screens) were randomized to treatment with no differential loss of men or minority participants from the point of initial pre-screening through randomization.
Participant characteristics
Participants were 22.3 ± 2.0 years old, with a mean BMI of 34.2 ± 5.5 kg/m2. They were primarily female (78.0%) and the sample was racially diverse (46.0% non-Hispanic White, 33.0% African American/Black, 11.5% Hispanic/Latino, 3.8% biracial, 1.9% Asian, and 3.8% declined to report). A majority of participants had never been married (73.0%), the sample was highly educated (94.2% had at least some college), and just over half of participants were current college students (53.8%). There were no differences between groups on demographic variables.
Engagement
A comparison of engagement data across arms is displayed in Table 4. Attendance at treatment sessions in FBWL was higher than the percentage of participants who viewed web lessons in both the WBWL and Hybrid arms (p < .001); participants in Hybrid viewed more lessons than WBWL participants (p = .04). The majority of Hybrid participants attended at least one of the optional competency-building sessions offered. FBWL and Hybrid participants reported their weight more often than WBWL participants (p = .01). Dietary self-monitoring was higher in the Hybrid arm than in FBWL and WBWL arms (p = .01).
Treatment engagement across conditions.
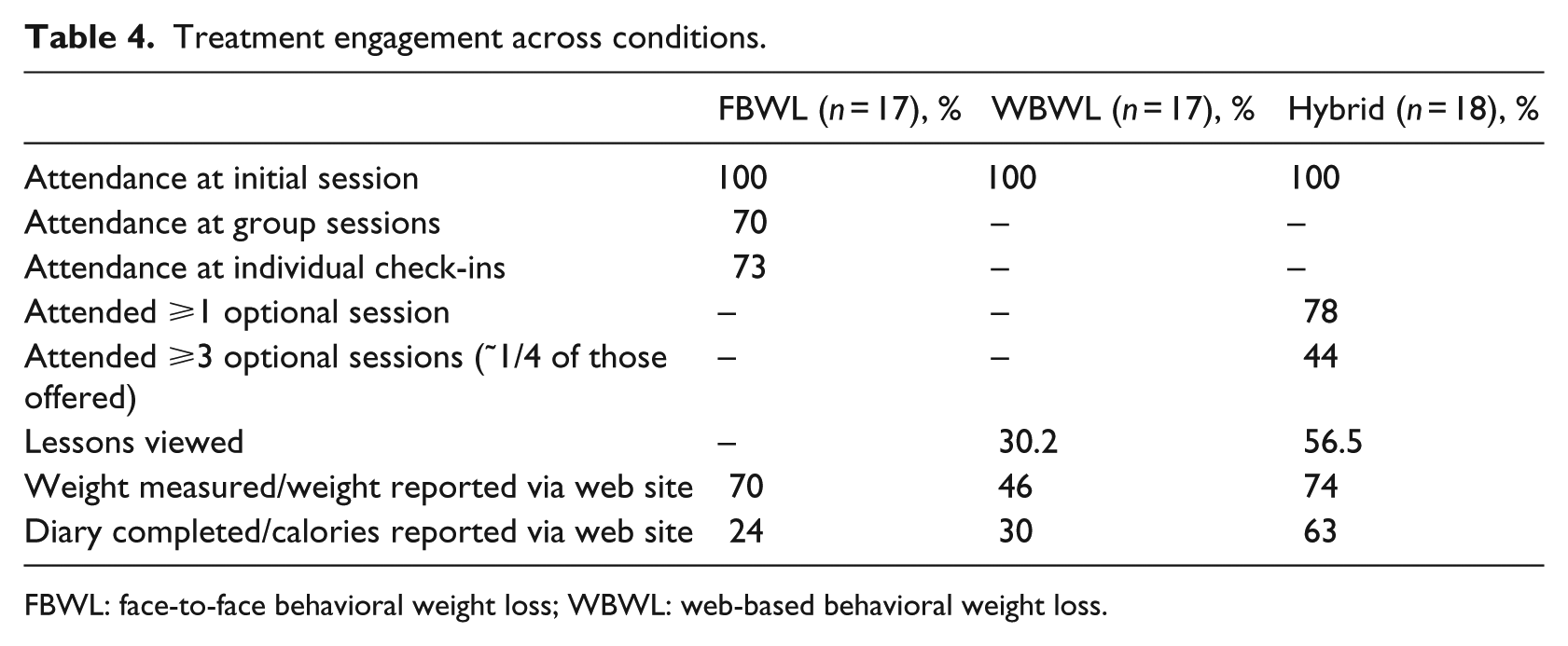
FBWL: face-to-face behavioral weight loss; WBWL: web-based behavioral weight loss.
Physical activity and dietary behaviors
At post-treatment, participants reported a decrease in fast food and sugar-sweetened beverages, with no differences between groups (p = .51 and p = .29, respectively). All groups reported a slight increase in the number of days they ate breakfast during the previous 30 days and this did not vary by arm (p = .89). Across groups, there was also a decrease in the number of days that participants consumed alcohol within the last 30 days with no group differences (p = .45). There was an overall increase in physical activity across groups (+62.8 minutes), but there were no significant group differences in change in total minutes of activity per week (p = .25). However, a greater proportion of participants in Hybrid arm met the 250 minutes/week goal at 3 months (40%) relative to both FBWL (13.3%, p = .10) and WBWL (18.2%, p = .23).
Retention
Overall retention at post-treatment was 81 percent but there was a trend for this to differ across arms (88%, 65%, and 89% in FBWL, WBWL, and Hybrid, respectively; p = .12). At the 6-month follow-up visit, retention differed across arms (88%, 53%, and 83% in the FBWL, WBWL, and Hybrid arms, respectively; p = .04).
Acceptability
More participants in the FBWL and Hybrid arms reported that they were satisfied with the program, relative to participants in WBWL (93% and 88% vs 42%, respectively, p = .01). A similar pattern emerged in terms of those who indicated that the information they learned in the program would be relevant to others their age who want to lose weight (93% for FBWL, 88% for Hybrid, 58% for WBWL, p = .02).
Weight loss at post-treatment
In ITT analyses, Hybrid arm participants lost 4.8 ± 4.9 percent of initial weight, compared with weight losses of 2.8 ± 2.9 percent and 2.2 + 4.5 percent in the FBWL and WBWL conditions, respectively (see Figure 2). Given the pilot nature of this study and the small sample size, these effects were not statistically significant (F(2, 49) = 1.84, p = .17; Cohen’s f = .27). Parallel analyses of BMI revealed similar patterns of change observed for Hybrid, FBWL, and WBWL conditions, respectively (−1.46 ± 1.5, −0.84 ± 1.0, and −0.76 ± 1.6, p = .27; Cohen’s f = .24).

Percent weight loss—intent to treat.
Completer analyses revealed a similar pattern in percent weight loss (5.3% ± 4.9% in Hybrid, 3.1% ± 2.9% in FBWL, and 3.3% ± 5.3% in WBWL; p = .32; Cohen’s f = .24) and BMI change (−1.64 ± 1.5 kg/m2 in Hybrid, −0.95 ± 1.0 kg/m2 in FBWL, and −1.17 ± 1.8 kg/m2 in WBWL, p = .41; Cohen’s f = .22). Whereas, only 27 percent of participants in the FBWL and 27 percent of those in the WBWL arm lost ⩾5 percent of their initial weight, and 63 percent of Hybrid participants lost ⩾5 percent of initial weight (p = .045).
All indicators of engagement (i.e. session attendance, lesson views, weight reporting, and self-monitoring of diet) were individually and positively associated with weight change at 3 months such that greater engagement in the program was related to greater weight losses achieved; this relationship was evident within each treatment arm and across groups as well (p < .05). Overall engagement (combining all types) was associated with greater weight loss at 3 months (p < .001).
Maintenance of weight loss at follow-up
After a 3-month no contact period, weight was reassessed. In ITT analyses, overall weight change from baseline to 6 months was greater in the Hybrid arm than the FBWL and WBWL arms (−4.6% ± 5.3%, −1.8% ± 4.6%, −1.4% ± 3.2%, p = .08; Cohen’s f = .33). Patterns were similar in completers-only analyses (−5.5% ± 5.3%, −2.0% ± 4.9%, −2.6% ± 4.1%, p = .14; Cohen’s f = .34), as well as when examining change in BMI using both ITT (p = .08, Cohen’s f = .24) and completers (p = .18, Cohen’s f = .35).
Weight change from 3 to 6 months only was also examined and data indicate that Hybrid lost additional weight over the 3-month follow-up, whereas FBWL and WBWL gained weight (ITT = −0.47% ± 2.0%, +0.99% ± 2.8%, +0.71% ± 3.5%, p = .28; Cohen’s f = .23 and Completers = −0.60% ± 2.3%, +1.13% ± 3.0%, +1.34% ± 4.9%, p = .28; Cohen’s f = .28). Similar patterns emerged for BMI change from 3 to 6 months (ITT: p = .14, Cohen’s f = .29 and Completers: p = .13, Cohen’s f = .36). Finally, to speak to clinically meaningful levels of maintenance, we used a threshold based on recent findings from Wing et al. (2016) and examined the proportion of participants in each condition who gained ≤1 lb from 3 to 6 months and found that the proportion was higher in the Hybrid arm relative to FBWL and WBWL (78.6%, 46.7%, 44.4%, p = .14).
Discussion
The aim of this randomized pilot study was to determine the feasibility and preliminary efficacy of a novel approach to engaging and retaining 18- to 25-year-olds in an adapted version of BWL. All participants received a 3-month lifestyle intervention that included calorie and activity goals, as well as evidence-based content that was adapted for this population based on formative work. Results suggest that for future efforts, utilizing an approach that maintains core elements of BWL but draws on principles of SDT, both in terms of program structure and goals, may improve engagement and weight loss with this high-risk age group. Indeed, the hybrid arm of this pilot trial that was delivered primarily via the web produced comparable engagement and better weight losses than the face-to-face program despite adapted content, well-attended weekly groups, and the addition of individualized check-ins and coaching to the face-to-face arm. The hybrid condition also appeared superior to the web-only arm in terms of engagement, retention, and weight loss, which suggests that there was something specific about the hybrid arm that promoted engagement in this age group, beyond technology-mediated intervention delivery. Given the majority of hybrid participants attended just 1–3 of the competency-building sessions offered, it is plausible that the differential emphasis on promoting autonomy and offering choice was a driving factor in the improved engagement within the hybrid arm.
Of note, the engagement and weight losses achieved by emerging adults in both the face-to-face and the web arms were considerably lower than those observed in other weight loss studies using both delivery modalities (Jakicic et al., 2012, 2015; Tate et al., 2003, 2006). Lower observed weight losses may be explained by suboptimal engagement, including low rates of dietary self-monitoring and reporting of key behaviors. Self-monitoring data were used to drive e-coaching, and thus, participants who did not complete food diaries or report summary dietary data via the web site were unlikely to receive specific feedback regarding their dietary choices. This was especially problematic in the web-only arm, given that coaches in the face-to-face arm were still able to provide individualized coaching and problem solving in-person despite the lack of self-monitoring records because in-person treatment sessions were well attended. Of note, however, relative to previous reports of emerging adults, these findings compare favorably. Napolitano et al. (2013) conducted a brief intervention in college students and reported engagement with self-monitoring data to be 68.5 percent, which is consistent with the 70 percent weight reporting in this study. Weight losses achieved in the most successful arm of that pilot trial were −2.4 ± 2.5 kg at 8 weeks (Napolitano et al., 2013), whereas weight losses in the hybrid arm of this pilot trial were −4.8 percent at 12 weeks. Furthermore, in a review of studies focused on 18- to 25-year-olds specifically, 14 pilot studies were reviewed, and of the few pilot studies that included both diet, activity and behavioral strategies, average weight losses achieved were −2.96 kg (Poobalan et al., 2010). Importantly, the sample size and randomized design of the current pilot trial as well as the use of an evidence-based BWL protocol that was adapted based on formative work are notable improvements over the pilot studies reviewed by Poobalan et al. (2010).
Although hybrid approaches in other studies are arguably of higher intensity than the one tested in this study, they have historically been unable to produce weight losses comparable to in-person treatment, unlike in this study. One study, delivered in a healthcare setting and targeting adults, used an Internet site to deliver content and for monitoring but provided behavioral coaching via telephone calls (Appel et al., 2011). Other hybrid Internet models have used weekly online group sessions with in-person group treatment sessions once per month (Harvey-Berino et al., 2010). The hybrid model used here retained the web for convenience and to respond to the expressed needs and preferences of emerging adults but also retained some of the accountability, intensity, and support by offering optional in-person competency-building sessions. Since these groups were not run by interventionists and were offered through existing community businesses, this is a model that could be easily replicated outside of an academic medical research center.
Given the documented challenges recruiting and engaging this population in weight control trials (Gokee-LaRose et al., 2009b; Loria et al., 2010; Poobalan et al., 2010), these findings are of particular interest. Indeed, retention rates in the in-person and hybrid arms surpassed those previously documented among emerging or young adults (Gokee-LaRose et al., 2009b; LaRose et al., 2010, 2012). The differential rates of self-monitoring between arms are particularly notable, with participants in the hybrid arm completing more diet monitoring than those in the face-to-face or web-only arms. Furthermore, participants in the hybrid arm weighed themselves as often as those in the face-to-face arm, but did so outside of the context of weekly weigh-ins with study staff. The emphasis on autonomy in the hybrid arm may play an important role in these differences, whereas participants in the face-to-face group may have completed diaries or weigh-ins due to perceived pressure or accountability from their coach. Although accountability certainly existed between coaches and participants in the web and hybrid arms as well, these arms lacked individual in-person check-ins, in-person weigh-ins, and full diary reviews, which may have increased perceived accountability but perhaps undermined autonomy in the face-to-face arm.
Limitations of this study include the small sample which was highly educated and predominantly female, and consisted of just a single cohort of participants, and the fact that height was not reassessed at 6 months given the potential for growth in this population. In addition, as with any comprehensive lifestyle intervention, those tested here included many components and it is difficult to determine which of the specific intervention components accounted for behavior change. This limitation is somewhat lessened by attempts to equalize evidence-based strategies across arms—all conditions received goals for diet and physical activity, identical adapted evidence-based lesson content to teach behavioral strategies, and weekly reporting of key behaviors with personalized feedback on progress. The relative emphasis on promoting autonomy and choice in goal setting and in program structure, in addition to the opportunity to practice achieving competency within a real-world setting as opposed to in the treatment group, was the key factor that differed between conditions. Although we might hypothesize that these differential factors accounted for the differences between arms observed, a major limitation of this pilot trial relates to the lack of data on potential mediators of interest consistent with SDT (e.g. autonomous self-regulation, perceived competence, and autonomy support). Given the pilot nature of this study and the attrition risk posed by this population, assessment measures were limited in scope for the purposes of this initial pilot trial, which was focused on preliminary feasibility and engagement. Future tests of the hybrid approach, which was informed by SDT, should include repeated measures of SDT constructs to determine whether change in these variables mediates weight loss outcomes. Finally, as is common in BWL trials, there was considerable variability in outcomes in this study; future work should seek to determine how best to minimize this variability and intervene as appropriate to promote better engagement and weight losses in all participants. For example, recent findings with older adults have indicated that long-term weight loss success can be predicted as early as 1 month into an intervention (Unick et al., 2014); future studies with this population should seek to examine whether non-responders can be identified early in the intervention, and if so, how interventions can be designed to adapt to better meet the needs of these individuals.
Strengths of this study include the randomized design, a racially diverse sample, an intervention well-grounded in theory and formative data, and strong retention rates in a historically challenging age group. Moreover, to our knowledge, this is one of very few trials to develop and test a BWL program for weight loss in 18- to 25-year-olds; in fact, a previous review on weight loss in 18- to 25-year-olds noted the lack of well-executed trials developed for and tested in this age group and authors noted the need for work to be done in this area (Poobalan et al., 2010). Given the rates of overweight and obesity in this age group (Muyle et al., 2009), coupled with the documented risk of additional weight gain (Lewis et al., 2000; Truesdale et al., 2006) and a host of unhealthy weight-related behaviors that spike during these years (Nelson et al., 2008), effective treatment may have substantial medical and public health benefits. The present findings, although preliminary in nature, have the potential to inform future work in this area. Findings suggest that the hybrid approach tested here may be feasible, acceptable, and efficacious for promoting engagement and retention in this high-risk population; moreover, data suggest this approach holds potential for producing clinically meaningful weight losses.
Future studies should explore whether outcomes can be replicated in a larger sample and whether these effects can be maintained longer term, and also seek to better understand whether it is the hybrid modality, the emphasis on autonomy and choices offered, or a combination of the two that drive engagement and weight loss in this population. This area of research also stands to gain important insights from testing specific strategies to enhance engagement and/or weight loss outcomes in future BWL programs designed for this population. For example, efforts might include targeting executive functioning domains that predict consumption of fruits/vegetables and high-fat foods in young adults (Limbers and Young, 2015) or explicitly offering and/or marketing “fun” experiential physical activity classes, which has been shown to decrease compensatory eating among young adult dieters (Chang and Lin, 2015) and is consistent with our formative data which indicated a desire for fun and experiential activities as part of BWL programs (LaRose et al., 2016).
Footnotes
Acknowledgements
The author(s) thank Sarah Conklin, PhD, Annalucia Bayes, and Jana Hayes for their contributions to this study. Authors also thank Kristen Polzien, PhD and Karen Erickson, MPH, RD for their time and assistance in training of research staff. They also extend their gratitude to Dr Leslie Lytle, who served as the safety officer for this project. A special thanks to the participants in the SPARK RVA program. Clinical Trials Registration#: NCT01889082.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Tate is on the Scientific Advisory Board for Weight Watchers. The other authors have no conflicts of interest to disclose.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) to J.G.L. (K23 DK083440). The content is solely the responsibility of the authors and does not necessarily represent the official views of NIDDK or the National Institutes of Health.