
Abstract
The stress effect on multiple sclerosis remains unclear. Moderating psychosocial factors may be involved. This study compares some of them in people with multiple sclerosis and healthy controls, and their association with disease parameters. Coping style, social support, anxiety, alexithymia and early-life stress were measured, along with impairment and functionality. People with multiple sclerosis scored significantly higher on anxiety, alexithymia, and avoidance and instinctive coping but lower in social support. No differences were found in early-life stress. Impairment was related to avoidance, and functionality to avoidance and anxiety. Psychotherapeutic approaches focused on these psychosocial factors may improve functionality, impairment and quality of life in people with multiple sclerosis.
Introduction
Multiple sclerosis (MS) is a neurodegenerative autoimmune disease that affects 2.3 million people around the world. It is more prevalent in women than men (2:1) and is one of the main causes of non-traumatic disability in young adults (Browne et al., 2014). The aetiology involves multiple genes and environmental factors (Lutton et al., 2004). One of the proposed environmental risk factors for MS onset and exacerbation is stress. Through psychoneuroendocrinologic pathways, stress may affect autoimmune diseases (Segerstrom and Miller, 2004). Studies evaluating stress effects on MS have yielded contradictory results. Some studies found an increased risk for MS onset and exacerbation after stressful events, whereas other studies did not show any relationship (for a review, see Briones-Buixassa et al., 2015). One reason may be that stress does not affect people in a straightforward way and other psychosocial moderating factors need to be considered. According to Lazarus and Folkman’s (1984) transactional model, stress is defined as a relationship between the individual and the environment in which an individual responds through behavioural, emotional and physiological mechanisms. Stress process involves many variables and moderating factors associated with appraisal and coping processes. These factors include environmental and psychological factors, individual differences and coping (Lazarus, 1990). This study aims to study some of these psychosocial factors in people with multiple sclerosis (pwMS) and healthy controls.
Previous research comparing people with and without MS on coping styles suggests that pwMS tend to use less problem-focused coping (trying to solve the problem) and to seek less social support than people without MS (McCabe et al., 2004). Specially, those patients in an exacerbation phase showed a tendency to favour emotion-focused coping compared to those patients in a remission phase.
Of all the coping styles, seeking social support has been postulated to cause a buffering effect on stress. In pwMS, social support decreases the relationship between stress and relapse (Brown et al., 2006) and enhances positive perceptions of physical and mental health (Krokavcova et al., 2008). PwMS tend to use less social support (McCabe et al., 2004), but there are no studies showing a comparison between pwMS and healthy controls on perceived social support.
There are also psychological dispositional factors that affect appraisal and coping including anxiety and alexithymia. High trait anxiety put individuals at risk for more dramatic threats and loss appraisals, whereas low trait anxiety buffers the experience of stress (Jerusalem, 1990). In pwMS, high levels of anxiety have been associated with 2.9 times the rate of relapse (Potagas et al., 2008). Alexithymia is defined as a difficulty in experiencing and expressing emotional responses. There is some evidence that pwMS report higher levels of alexithymia than the general population (Prochnow et al., 2011). Kojima (2012) suggests that alexithymia is related to illness through biological causes and inadequate coping processes, but the link with disease parameters remains unclear.
Finally, coping and appraisal are also affected by early-life traumatic experiences. Early-life stress can have behavioural and physical consequences that may remain into adulthood (Spertus et al., 2003) promoting inadequate stress appraisal and coping later in life. In a large case-control study, Spitzer et al. (2012) observed that pwMS showed significantly higher childhood stress than people without MS, and among patients, those with histories of physical or sexual abuse had higher relapse rates than patients without early-life stress.
There are few studies focused on the psychosocial factors that may moderate the stress-MS relationship. In a recent systematic review, Briones-Buixassa et al. (2015) highlighted the importance of taking these into account, as some of the psychosocial factors mentioned above are potentially modifiable. According to literature review, we hypothesise that pwMS will show more emotion-focused and avoidant coping patterns, lower social support and perception, and higher levels of anxiety, alexithymia and early-life stress than healthy controls. Moreover, we expect that these coping patterns and higher levels of anxiety, alexithymia and early-life stress will be negatively associated with disease parameters including impairment and functionality. For this reason, this study aims to (1) compare the proposed psychosocial factors in pwMS and healthy controls and (2) to analyse their association with disease parameters in the MS group.
Methods
Participants
A total of 41 MS patients and 41 healthy participants, matched by age and gender, participated in the study from May 2014 to June 2015. MS patients were recruited from the Consorci Hospitalari de Vic. This study formed part of a larger study where some potential modifiers of disease progression were exclusion criteria. These were as follows: (1) under 18 years old, (2) pregnant, (3) abuse of alcohol or drugs, (4) Expanded Disability Status Scale (EDSS) ≥ 7 and (5) diagnosis of other neurologic or psychopathological diseases. The healthy control group was obtained through local advertisement. Exclusion criteria were the same adding (6) diagnosis of MS and other chronic illnesses. All adult patients had clinically definite relapsing-remitting MS, according to McDonald criteria (Polman et al., 2005).
Study design and procedure
This is a case-control study nested within the project called ‘PsychoMSS Study: Stress and Psychosocial Factors in Multiple Sclerosis’ developed in Osona (Catalonia, Spain). The study design consisted of an interview of 1-hour duration, conducted by a trained psychologist. Using the same protocol for all the participants, a brief semi-structured interview was conducted and a battery of standardised self-reported questionnaires was administered. Other clinical data were collected through medical records. The study was approved by the local ethics committee, FORES Foundation (23 July 2013, no. 2013841-PR71), and conducted according to the Declaration of Helsinki. All of the participants gave written informed consent.
Measures
Information about age, gender, marital status, educational level, lifestyle and family history of diseases were obtained. For the pwMS, also year of diagnosis, MS type, EDSS score, treatment and other diagnosed diseases were obtained from medical record.
Psychosocial factors
Coping processes were assessed using the Strategic Approach to Coping Scale (SACS) of Hobfoll, a 52-item scale, Spanish version (Pérez et al., 2012), assessing seven coping strategies: (1) assertive action (conflict identification and attempt to solve the problem), (2) social joining (have ‘significant others’ as collaborators), (3) seeking social support (seek external resources), (4) cautious action (leisurely assessment of threat, resources, needs and aid), (5) instinctive action (immediate, spontaneous action), (6) avoidance (avoiding conflictive elements, minimising emotional impact) and (7) aggressive/antisocial action (prioritising own needs and immediate resolution). Higher scores mean higher use of the particular coping strategy.
Perceived social support was assessed by Multidimensional Scale of Perceived Social Support (MSPSS), a 12-item scale, Spanish version (Landeta and Calvete, 2002), assessing three sources of social support: family, friends and relevant persons. Total score ranged from 12 to 84 points. A higher score means higher levels of perceived social support.
Trait anxiety was assessed by State-Trait Anxiety Inventory (STAI), a 20-item scale, Spanish version (Spielberger et al., 1982). Total score ranged from 0 to 60 points. A higher score means higher level of anxiety. High trait anxiety was considered ≥ 28 in men and ≥ 31 in women (above percentile-75 adjusted for age and gender in standardised Spanish population tables).
Alexithymia was assessed by Toronto Alexithymia Scale (TAS-20), a 20-item scale, Spanish version (Martínez-Sánchez, 1996). It evaluates three factors: difficulty identifying feelings, difficulty describing own feelings and externally oriented thinking. Total score ranged from 20 to 100 points, and cut-off scores were ≤ 51 (no alexithymia), 52–60 (possible alexithymia) and ≥ 61 (alexithymia).
Early-life stress was assessed by Childhood Trauma Questionnaire-Short Form (CTQ-SF), a 28 item-scale, Spanish version (Hernandez et al., 2013). It evaluates five child maltreatment types: emotional, physical and sexual abuse, and physical and emotional neglect. Total score ranged from 0 to 108 points. Higher scores mean higher levels of childhood trauma.
Disease parameters
Three different measures were used to assess the disease parameters. First, a neurologist-rated disease-related impairment by EDSS score (EDSS-tot). EDSS scale (Kurtzke, 1983) ranges from 0 to 10 in 0.5 unit increments that represent higher levels of impairment. A score of 7 and above means daily life support is required. Second, a relative score of EDSS progression was computed by dividing EDSS by years of disease (EDSS-relative). Third, self-reported functionality assessed by the Functional Assessment of Multiple Sclerosis (FAMS) questionnaire, validated in Spanish pwMS by Chang et al. (2002). FAMS measures seven subscale symptoms: mobility, symptoms (i.e. pain), emotional state, life satisfaction, mental activity and fatigue, family/social environment and other preoccupations (i.e. incontinence). The total score range from 0 to 236, higher score means greater functionality.
Statistical analysis
The data analyses were conducted using SPSS (version 23.0; SPSS Inc., Chicago, IL). To present descriptive data, means and standard deviations were used for continuous variables, and absolute frequencies and percentages for categorical variables. To test the data normality, Shapiro–Wilk’s test was used. To make comparisons between groups, independent t-tests were used for continuous variables and chi-square test for categorical variables. To calculate effect size, Cohen’s d was used for t-test comparisons (small: <0.2, medium: 0.2–0.5, large: >0.8), and phi-coefficient and Cramer’s V for chi-square comparisons (small: <0.1, medium: 0.1–0.3, large: >0.3). Two hierarchical regression analyses were conducted in pwMS to determine which of the psychosocial factors were related to disease parameter outcomes after controlling for relevant socio-demographic variables. Significance level was set at 5 per cent (p ≤ 0.05).
Results
Socio-demographic, lifestyle and clinical characteristics of the participants are presented in Table 1. No differences were found in socio-demographic data, but groups differed in family history and lifestyle. PwMS showed significantly fewer antecedents in autoimmune diseases (different from MS), but significantly more smoking and drug consumption (before diagnosis) than controls.
Socio-demographic, lifestyle and clinical characteristics of the participants.

MS: multiple sclerosis; pwMS: people with multiple sclerosis; EDSS: Expanded Disability Status Scale; SD: standard deviation; TC: tobacco consumption; PA: physical activity.
p < 0.05; **p < 0.01 (two-tailed).
Comparisons between pwMS and controls on all the psychosocial factors are presented in Table 2. Coping scores showed that pwMS seek significantly less social support and use more instinctive action and avoidance coping than controls when facing stressful situations. Moreover, pwMS reported significantly lower perceived social support, mainly explained by the difference in perceived social support from family and relevant persons. Trait anxiety mean scores were significantly higher in pwMS, and 36.7 per cent of pwMS had high trait anxiety, a higher percentage than control group. Regarding Alexithymia, 40 per cent of the pwMS scored higher or equal than cut-off (≥52), whereas only 19.5 per cent of the general population did. Mean scores in alexithymia were also significantly higher in pwMS. This was explained by a significant difference in difficulty identifying feelings, whereas no differences were found for the other alexithymia factors. No significant differences were found in early-life stress, but there was a tendency in pwMS to score higher in total score, emotional abuse and neglect.
Psychosocial variables scores comparing pwMS and control participants.

pwMS: people with multiple sclerosis; SACS: Strategic Approach to Coping Scale; MSPSS: Multidimensional Scale of Perceived Social Support; STAI-T: State-Trait Anxiety Inventory; TAS-20: Toronto Alexithymia Scale; CTQ-SF: Childhood Trauma Questionnaire-Short Form; P75: percentile 75; SD: standard deviation.
p < 0.05; **p < 0.01 (two-tailed).
Psychosocial factors and disease parameters
In pwMS, all psychosocial factors were correlated at the bivariate level with the disease parameters: EDSS-tot, EDSS-relative and FAMS (Table 3). EDSS-tot showed significant correlations with social joining and avoidance coping styles. FAMS showed significant correlations with social joining, cautious and avoidance coping styles, perceived social support, trait anxiety, alexithymia and early-life stress. EDSS-relative did not show any significant correlations with the psychosocial variables.
Psychosocial correlates of EDSS-tot, EDSS-relative and FAMS.
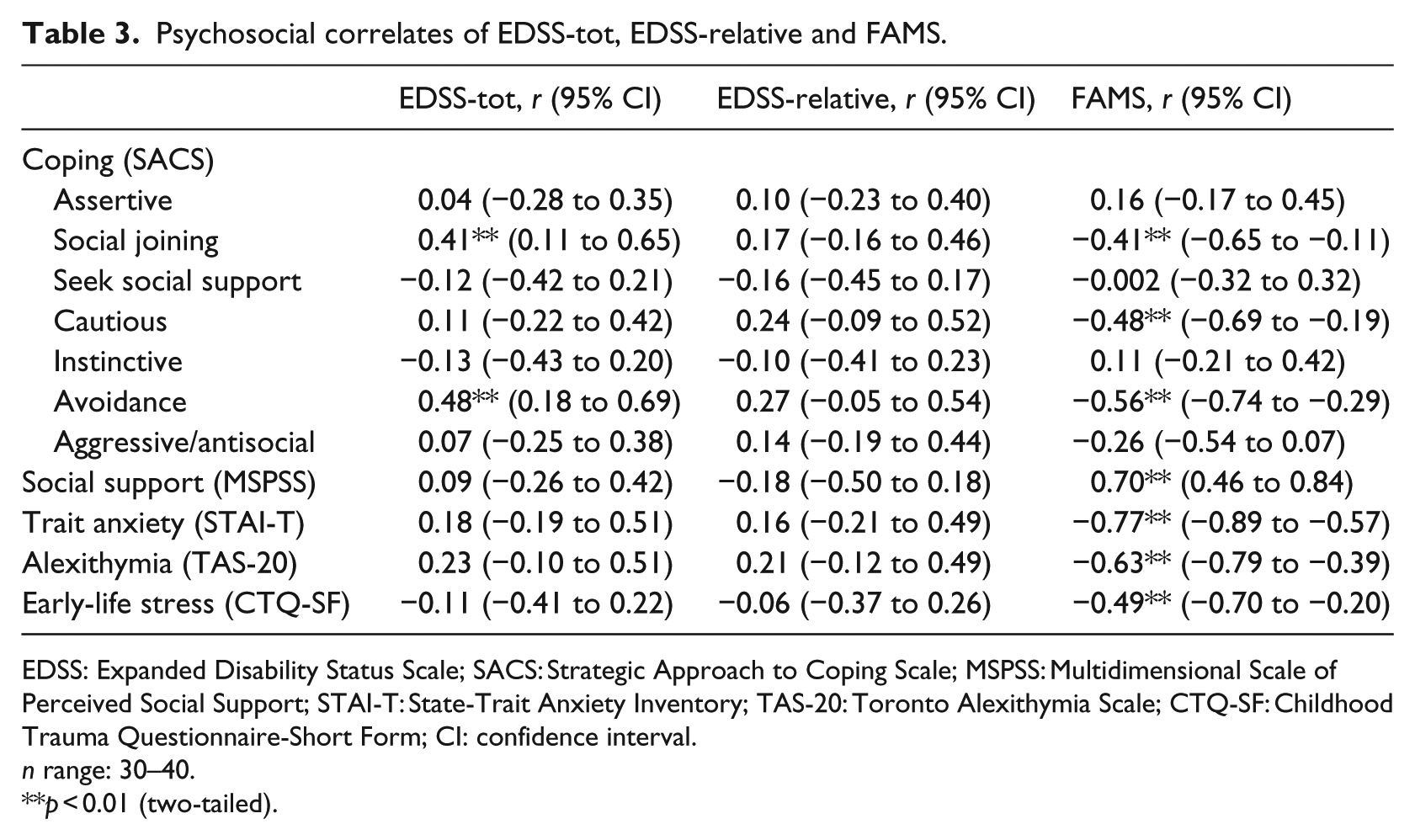
EDSS: Expanded Disability Status Scale; SACS: Strategic Approach to Coping Scale; MSPSS: Multidimensional Scale of Perceived Social Support; STAI-T: State-Trait Anxiety Inventory; TAS-20: Toronto Alexithymia Scale; CTQ-SF: Childhood Trauma Questionnaire-Short Form; CI: confidence interval.
n range: 30–40.
p < 0.01 (two-tailed).
Two hierarchical regressions were conducted using all the significantly correlated psychosocial factors as predictors, and EDSS-tot and FAMS as outcomes adjusting by age, gender and educational level (Table 4). Socio-demographic variables were entered in the first step and psychosocial factors in the second step. The first step of the hierarchical regression showed that socio-demographic variables accounted for 12 per cent (ΔF = 1.61, p = 0.21) of the variance in EDSS. Adding psychosocial factors explained a further 23 per cent (ΔF = 3.569, p = 0.01). Avoidance was the only significant predictor in the second step (B = 0.42, p = 0.02). In the second regression, socio-demographic variables accounted for 8 per cent (ΔF = 0.686, p = 0.57) of the variance in FAMS. Adding psychosocial factors explained 71 per cent of the variance (ΔF = 6.66, p < 0.001). Avoidance (B = −0.30, p = 0.05) and trait anxiety (B = −0.39, p = 0.04) were the only significant predictors in the second step.
Hierarchical regressions: psychosocial predictors of EDSS and FAMS.
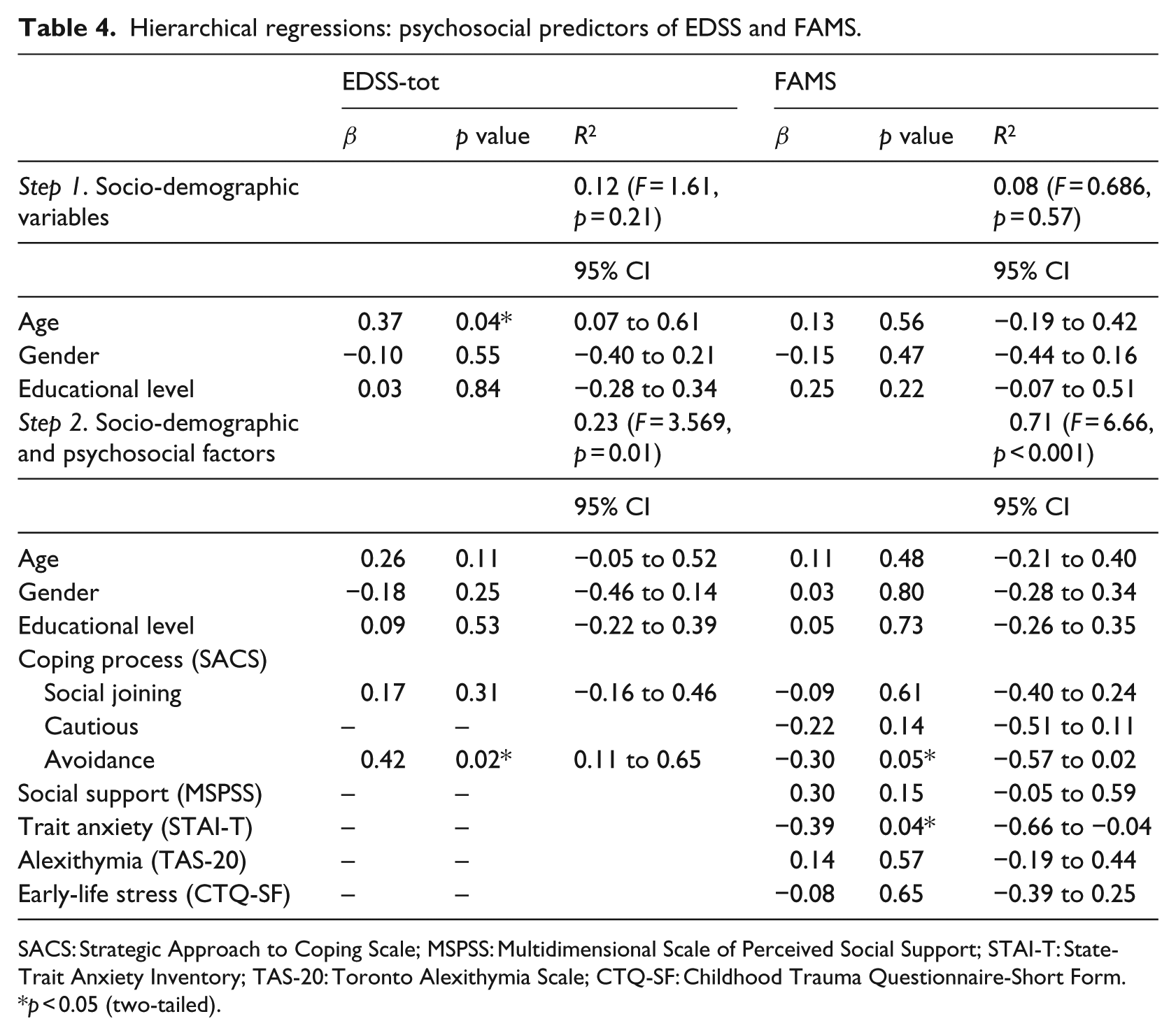
SACS: Strategic Approach to Coping Scale; MSPSS: Multidimensional Scale of Perceived Social Support; STAI-T: State-Trait Anxiety Inventory; TAS-20: Toronto Alexithymia Scale; CTQ-SF: Childhood Trauma Questionnaire-Short Form.
p < 0.05 (two-tailed).
Discussion
There are few studies addressing the study of psychosocial factors related to stress and MS. Our results showed that pwMS tend to use more passive (avoidance) and instinctive approaches to dealing with stress or problems, seek less social support and perceived less social support when compared to healthy controls. PwMS also show higher levels of anxiety and alexithymia but not greater levels of early-life stress. The disease parameters of impairment and functionality were most strongly related to anxiety and avoidance coping.
Previous literature supports our findings that avoidance is a common coping style in pwMS facing stressful situations (Hajhashemi et al., 2010), as well as less use of social support and problem-focused strategies (McCabe et al., 2004). However, this is the first study showing that pwMS not only use less social support but also that the perception of support from social network is reduced. Regarding anxiety and alexithymia, higher scores were observed in pwMS than healthy controls, in line with previous studies (Hoang et al., 2016; Prochnow et al., 2011).
This study showed different patterns of coping and personality between pwMS and healthy controls. Although we do not know whether these patterns existed before the diagnosis or are a consequence of either biological or psychological aspects of MS, some hypothesis can be made based on theoretical assumptions.
Following the transactional model (Lazarus and Folkman, 1984) where stress is considered as an outcome of the individual–environment interaction, we could hypothesise that suffering a chronic illness like MS might modify the coping strategies through altering the cognitive appraisal of stressful situations. Some disease characteristics like the unpredictability or the lack of understanding from social networks could promote these alterations. The coping styles observed (avoidance, instinctive action and less social support seeking) could be related not only to the perception of less social support but also with the higher levels of alexithymia, especially because pwMS have more difficulties identifying their own feelings. Previous studies in pwMS have shown a deficit in the recognition of emotional facial expressions and instrospection (Prochnow et al., 2011) and an impaired social cognition (Pöttgen et al., 2013), which fits with the deficits observed in alexithymia. The lack of ability to identify one’s own feelings, as well as to recognise emotions from facial expressions, is crucial for social functioning and could lead pwMS to misunderstand or be unaware of important social clues, deteriorating the social network.
According to our results, early-life stress seems not to have an important role in MS. The tentative evidence for a higher prevalence of early-life stress in pwMS (Spitzer et al., 2012) suggests that more important than occurrence is how people deal with stress. The ‘stress-resilience’ hypothesis, defined as an individual’s ability to properly adapt to stress and adversity, identified three categories that protect against stress: child dispositional attributes, family cohesion and external support (Garmezy, 1985). These resilient factors should be considered in future studies about early-life stress. Interestingly, in a recent qualitative study about resilient factors in adjustment to neurological chronic illnesses, McCabe and O’Connor (2012) found that people with high levels of adjustment showed better social support from family and friends, and this social support was used mainly to assist experiencing enjoyment more than illness-focused help.
Regarding the association between the psychosocial variables and the disease parameters, the regression analyses showed that anxiety and avoidance must be the most important ones. In previous studies, avoidance behaviour was linked to mental and physical symptoms (Ukueberuwa and Arnett, 2014) and to a poorer adjustment to MS (Dennison et al., 2009), and anxiety was linked to a greater impairment (Jones et al., 2014). Although avoidance behaviour and anxiety are related factors, in this study, they seem to be differently associated to disease parameters. Avoidance predicted both a neurologist-rated impairment and a self-reported functionality, whereas anxiety was only related to self-reported functionality. Higher levels of impairment and less functionality may lead to pwMS to use more avoidant strategies or to feel more anxiety when facing stressful situations, worsening the experience to deal with stressors. This deteriorating cycle may, in turn, amplify the stress response dysregulating the neuroendocrine system and worsening the disease progression. There is some modest evidence that coping may be related to disease progression. Mohr et al. (2002) measured disease progression through new brain lesions in magnetic resonance imaging scan. They found that emotional preoccupation (focused on emotional consequences) was marginally associated with an increased relationship between stress and disease, whereas use of distraction and instrumental coping was linked to a decreased relationship.
These results have important clinical implications since almost all the psychosocial factors considered are potentially modifiable through psychotherapeutic approaches. A recent randomised controlled trial (Moss-Morris et al., 2013) tested a cognitive behavioural therapy (CBT) for adjustment to MS. In this therapy, some coping factors were addressed. Interestingly, CBT was more effective for pwMS with low perceived social support and/or clinically defined levels of distress.
In this study, some limitations need to be addressed. The first is the sample size. Osona is a small region and few people met the inclusion criteria. The second is that only people with relapse-remitting type participated and it cannot be generalised to all MS types. The third is the low level of EDSS. Patients were recruited from different spread towns, but difficulties in displacement could have left out the most handicapped people. Finally, we did not measure stress itself. It would be interesting to study the moderating effect of these psychosocial factors in the stress–MS relationship.
Future studies should include large cohort studies, evaluating psychosocial factors in healthy subjects to see their link in the development of chronic illnesses. Moreover, more intervention studies testing psychotherapeutic approaches should be conducted to elucidate its potential benefits on disease progression. Finally, the moderating effect of the resilience factor on early-life stress should be considered to understand this complex process.
In conclusion, there are differences in the psychosocial factors related to appraisal and coping between pwMS and healthy controls and some of them are linked to disease parameters. Psychotherapeutic approaches could help to better adjust to the disease improving functionality, impairment and quality of life in pwMS.
Footnotes
Acknowledgements
The authors thank all the participants for helping us to carry out the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.