
Abstract
Depression is common among patients with diabetes, who have a higher risk of diabetes-related complications such as diabetic retinopathy, nephropathy, neuropathy and macrovascular complications. The aim of the systematic review is to determine whether cognitive behavioural therapy is effective in reducing depressive symptoms and improving glycaemic control among depressed diabetic patients. The results reveal diversified application of cognitive behavioural therapy. All studies reported that cognitive behavioural therapy had a positive impact on depressive symptoms; three found an improvement in glycated haemoglobin, and one demonstrated improved self-efficacy and self-concept related to successful diabetes management. There is a need for controlled studies with larger sample sizes and long-term follow-up.
Introduction
Depression is common among patients with diabetes (Lustman et al., 2000), and the presence of diabetes doubles the odds of co-morbid depression (Anderson et al., 2001; Egede et al., 2002). Researchers from various countries have rigorously investigated the prevalence of depression among patients with diabetes. For example, Ali et al. (2006) conducted a systematic literature review consisting of 10 randomised controlled trials, which included a total of 51,331 patients, to estimate the prevalence of clinical depression in adults with type 2 diabetes compared with those without type 2 diabetes. The review found the prevalence of depression among type 2 diabetes patients to be 8.9 per cent higher than those without diabetes.
Numerous studies have been conducted to investigate the factors that contribute to the onset of depression in diabetic patients. Empirical findings suggest that depression is more prevalent in females (Ali et al., 2006; Anderson et al., 2001; Blazer et al., 2002), those less educated (Cowie and Eberhardt, 1995; Egede et al., 2002) and of lower socioeconomic status (Anderson et al., 2001; Blazer et al., 2002). Katon et al. (2004) conducted a population-based mailed survey to determine the behavioural and clinical characteristics of diabetes that are associated with depression; 4193 participants from nine primary care clinics in Washington, DC, in the United States completed the survey. The findings indicated that independent factors such as younger age, gender (i.e. female), less education, being unmarried, body mass index (BMI) ≥30, smoking and higher non-diabetic medical co-morbidity were associated with major depression among diabetic patients. Moreover, younger age, less education, non-Caucasian status, BMI ≥30, smoking and longer duration of diabetes were associated with minor depression among diabetic patients.
Depression for those with diabetes has a negative impact on quality of life (Brown et al., 2004; Eren et al., 2008; Goldney et al., 2004; Schram et al., 2009). A large population-based study conducted in Australia by Goldney et al. (2004) found a clear difference in the quality-of-life scores for the diabetic and depression group when compared with the diabetic group without depression. The study concluded that depression for those with diabetes is a pivotal co-morbidity that requires careful management as it has a severe negative impact on quality of life.
Ciechanowski et al. (2000) conducted a study utilising a questionnaire design of 367 patients with type 1 and 2 diabetes to explore the impact of depressive symptoms in primary care patients with diabetes on diabetes self-care, adherence to medication regimens, functioning and health care costs. The results of the study found that depressed diabetic patients were less likely to adhere to oral hypoglycaemic regimens and dietary recommendations. In addition, numerous studies have found a significant association between depression and non-adherence to the diabetes treatment regimen and self-care behaviour (Egede and Osborn, 2010; Gonzalez et al., 2008). Studies have also found a significant association between depression and poor glycaemic control (Lustman et al., 2000; Roy et al., 2007).
Depressed diabetic patients have a higher risk of diabetes-related complications such as myocardial infarction (Scherrer et al., 2011) and retinopathy (Roy et al., 2007). De Groot et al. (2001) used a meta-analytical approach to examine the strength and consistency of the relationship between depression and diabetes complications in studies of type 1 and type 2 adult diabetic patients. A total of 27 studies were included within the meta-analysis. The study found a significant association between depression and a variety of diabetes-related complications, including diabetic retinopathy, nephropathy, neuropathy, macrovascular complications and sexual dysfunction. A costing analysis conducted by Egede et al. (2002) found that depression in individuals with diabetes is associated with increased health care use and expenditure. Among individuals with diabetes, total health care expenditure for individuals with depression was 4.5 times higher than that for individuals without depression.
Lehnert et al. (2011) systematically reviewed 11 studies to determine the cost of illness and the economic impact for diabetic patients with co-morbid depression. The results of the review indicated that patients with depression and diabetes incurred between 35 and 300 per cent excess costs compared to patients with diabetes and without depression. The excess cost was attributed to the treatment of diabetes.
There are various forms of treatment for depression. For example, there are approximately 30 different types of antidepressants that are available to treat depression (Royal College of Psychiatrists, 2015). However, antidepressants often have side effects (Ferguson, 2001). In addition, current evidence also suggests the usage of exercise therapy for the management of depression (Babyak et al., 2000). Rimer et al. (2012) conducted a meta-analysis of 28 trials (1101 participants) that included a comparison of exercise with either a waiting list or placebo to investigate the effect of exercise on depression. The authors concluded that exercise improved the symptoms of depression.
In recent years, a vast amount of investigations have been conducted to test the efficacy of psychological treatments in managing depression. Pampallona et al. (2004) conducted a meta-analysis to investigate the impact of combined pharmacotherapy and psychological treatment for depression. A total of 16 trials met the inclusion criteria, with 932 patients being randomised to pharmacotherapy alone and 910 to combined treatment. The authors concluded that psychological treatment combined with antidepressant therapy is associated with a higher improvement rate than drug treatment alone. There are various forms of psychological therapies that have been applied to depression management (e.g. guided self-help, cognitive behavioural therapy, counselling, peer support such as self-help, problem solving, interpersonal therapy, psychodynamic psychotherapy, group existential therapy, health education, social support and relaxation training).
Cognitive behavioural therapy (CBT) is based on the premise that there is a close connection between cognition, emotion and behaviour (Rothbaum et al., 2000). CBT aims to enable patients to correct false self-beliefs that can lead to negative moods and behaviours (Rupke et al., 2006). Various meta-analyses and systematic reviews have provided support for the efficacy of CBT in treating patients with depression (Gaffan et al., 1995; Gloaguen et al., 1998; Reinecke et al., 1998). There are various modalities that have been utilised to deliver CBT, including on a one-to-one basis and in groups (Brown et al., 2011). Furthermore, with technological advancement, new delivery modalities have emerged (Farrer et al., 2011; Ruwaard et al., 2009). In recent years, computerised CBT has gained popularity (So et al., 2013). Computerised cognitive behavioural therapy (CCBT) is an intervention that uses the computer to deliver interactive CBT sessions. The interactive programme helps the user to understand and modify their thinking. CCBT programmes guide a person through the principles of CBT as a therapist would during face-to-face sessions. An interactive CCBT programme can respond to particular circumstances, or problems, and ensure that the training of new ways of thinking and behaving is completed at a pace suited to the patient’s individual needs. One of the major advantages of CCBT is the ability to provide more treatment choices for patients and faster access to effective mental health services. CCBT has been effective in treating patients with depression (National Institute for Health and Care Excellence (NICE), 2009).
CBT has been effective in treating depressed patients with other co-morbid illnesses, such as coronary heart disease (Freedland et al., 2012; Hambridge et al., 2009), multiple sclerosis (Mokhtari et al., 2008), Parkinson’s disease (Dobkin et al., 2007), inflammatory bowel disease (Szigethy et al., 2004) and end-stage renal disease (Cukor et al., 2007). Recently, researchers have investigated the application of CBT to treat depression among diabetic patients (e.g. Georgiades et al., 2007). To date, no studies have systematically assessed the application and effectiveness of CBT among depressed diabetic patients.
Purpose and aim
The purpose of this systematic review is to explore the effectiveness of CBT for depressed diabetic patients. The aim of this review is to determine whether CBT interventions are effective in reducing depressive symptoms and improving glycaemic control among depressed diabetic patients.
Methodology
Search strategy, data sources and search terms
A systematic literature search was performed using Ovid, CINAHL, Embase, PubMed, PsycINFO, Web of Science and Cochrane Library databases for published articles (from 1995 to 2015). The search was performed between August 2015 and December 2015. The results obtained from the searches were screened to identify studies that met the inclusion criteria of this review.
The search terms used were as follows:
Diabet* or
Diabetes or
Diabetic
AND
Cognitive therapy or
Behaviour therapy or
Behaviour therapy or
Cognitive behavioural therapy or
Cognitive behavioural therapy or
AND
Depression
Depressive
Study selection criteria
Inclusion criteria were set out to identify studies for this review. All publications that met the inclusion criteria were included regardless of the study design. Studies included had to fulfil all criteria set out below.
Participants
Depressed diabetic patients (types 1 and 2)
Studies of adults and adolescents (13–16 years old) with mild to moderate depression were included in this review. Mild to moderate depression is defined with the Beck Depression Inventory (BDI; Beck et al., 1961) score of 1–28.
Interventions
Included studies had evaluated CBT interventions aimed at depressed diabetic patients. This review included studies that used CBT only as a sole form of treatment.
Types of outcome measures
Studies that reported depressive symptoms and glycaemic control were included in this review.
Studies that focused on postnatal depression, bipolar disorder, depression with psychotic symptoms or current major depression, or serious suicidal thoughts did not fall under the scope of this review. Published studies that used CBT in combination with other forms of intervention, such as exercise prescription, pharmacological intervention or holistic treatments, were excluded from this review.
A bibliographical search was conducted on studies identified to retrieve additional studies that met the inclusion criteria of this review.
Study selection
The electronic database search identified 136 studies. A bibliographic search was also conducted on identified studies. In total, 141 studies were identified. A total of 52 studies were excluded based on the title alone. The remaining 89 abstracts were reviewed. A further 76 papers were excluded for failing to meet the inclusion criteria of this review. The remaining 13 papers were subjected to a full article review. Six studies met all of the inclusion criteria of this review (Figure 1).
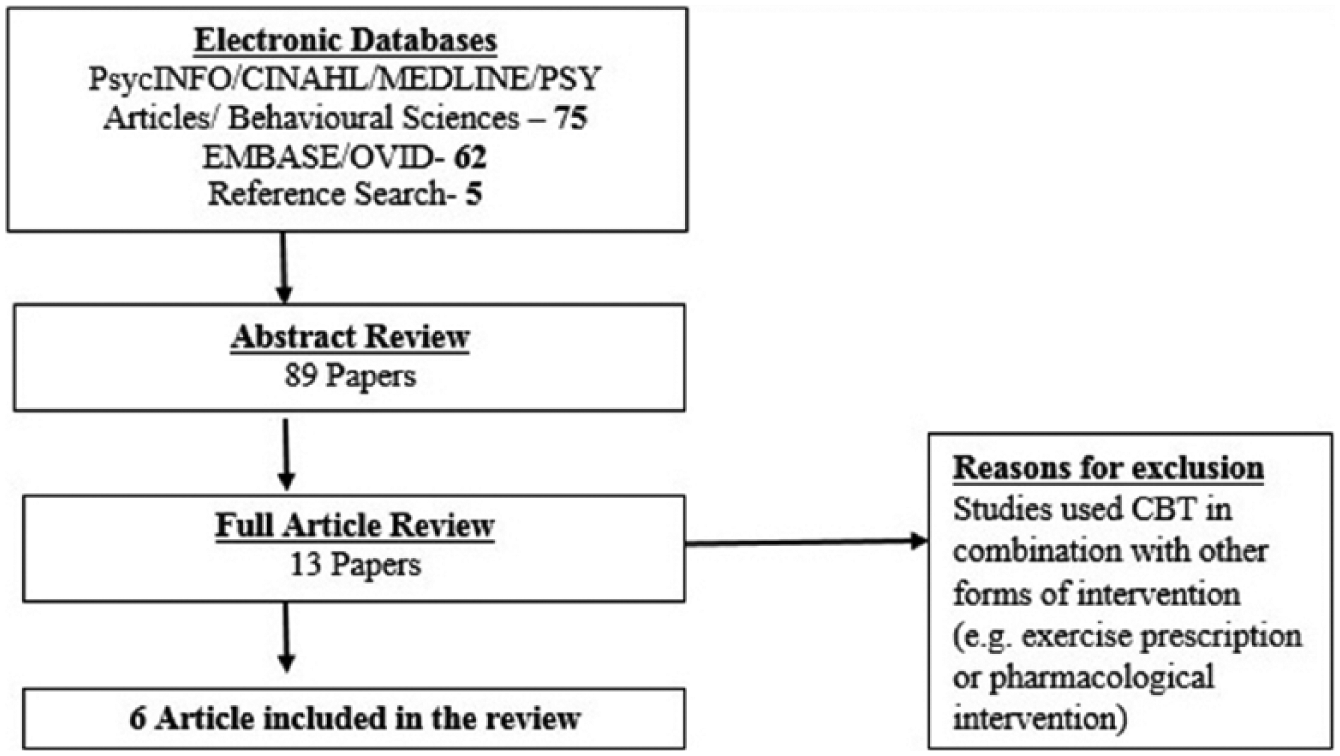
Study selection.
Data extraction
A data extraction sheet was developed based on the Cochrane Handbook for Systematic Reviews of Interventions, Version 5.1.0. Data were extracted by the main review author and checked by an independent reviewer. Information was extracted from each included study on (1) type of intervention (whether there was sufficient detail, such as the format of CBT intervention, session details and duration), (2) study design (i.e. randomised controlled trial, quasi-experimental and case series), (3) number of participants, (4) results on glycated haemoglobin (HbA1c) (i.e. whether a significant decline for HbA1c was found), (5) results on depressive symptoms (i.e. whether a significant decrease in depressive symptoms was found) and (6) other significant findings (i.e. whether any other significant findings were found). The data extraction is presented in Table 1.
Data extraction.
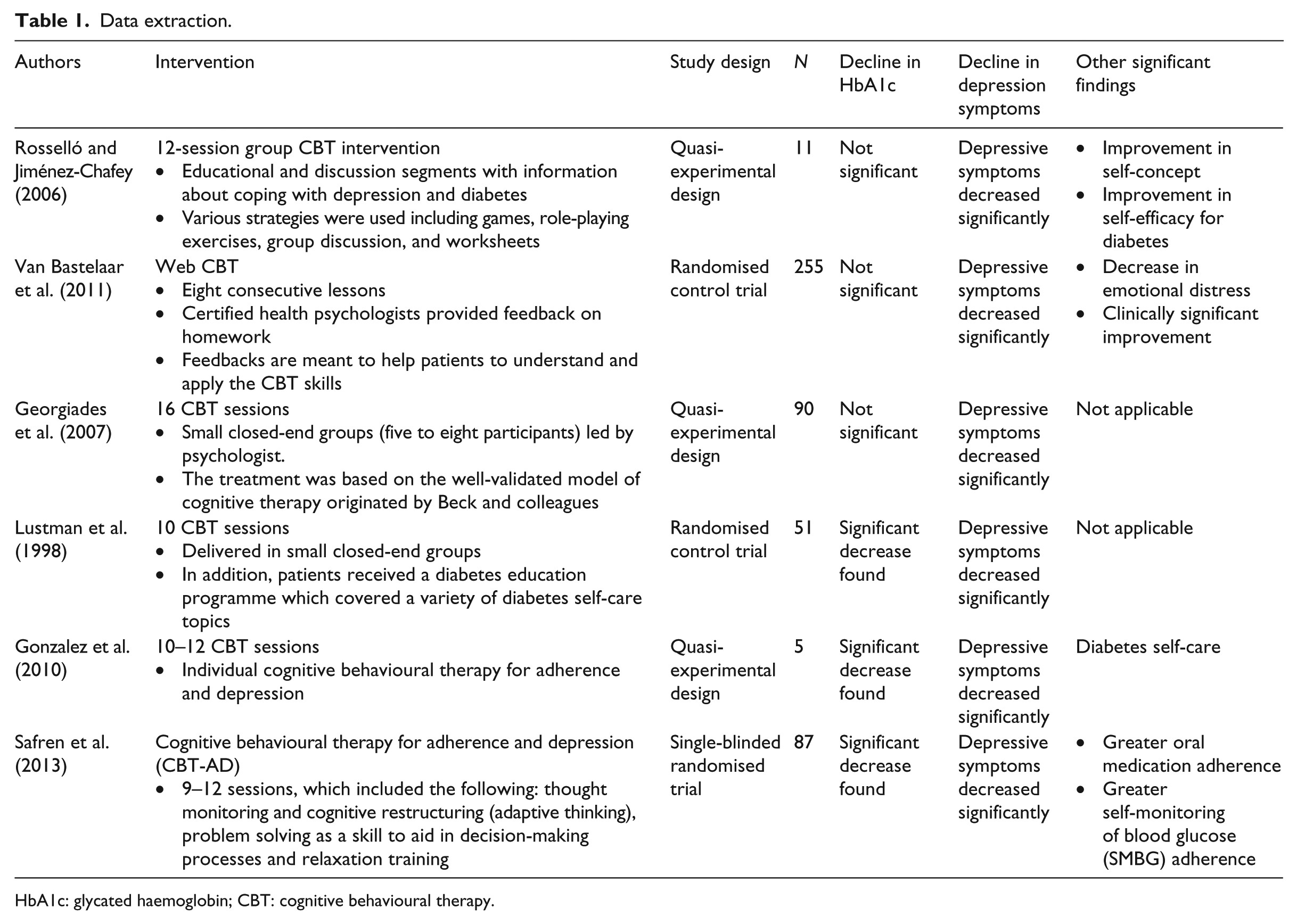
HbA1c: glycated haemoglobin; CBT: cognitive behavioural therapy.
Methodological quality assessment
The quality of the studies was assessed by two reviewers: the author and an independent reviewer. Disagreements were resolved through discussion. Two reviewers (J.K. and P.K.) reviewed all of the papers based on the criteria below:
Description criteria: Eligibility criteria specified; Description of intervention; Long-term follow-up (>6 months post-intervention); Similar baseline data.
Internal validity criteria: Randomisation performed; Method of randomisation performed; Blind assessment reported; Drop-out rates reported.
Statistical criteria: Power analysis conducted; Point estimates and measure of variability.
One point was allocated for each item of the methodology quality if the study fulfilled the criteria. If the study did not fulfil the criteria, zero marks were allocated. Total methodology quality scores were then summed up. Studies could get a maximum of 10 points. Studies scoring above 6 points were classified as being of a high quality. Studies scoring 4 points and below were classified as being of a low quality.
Results
The electronic database search identified 136 studies. A bibliographic search was also conducted on identified studies. In total, 141 studies were identified. In total, 52 studies were excluded based on the title alone. The remaining 89 abstracts were reviewed. A further 76 papers were excluded for failing to meet the inclusion criteria of this review. The remaining 13 papers were subjected to a full article review. Six studies met all of the inclusion criteria of this review (Figure 1).
Overview of studies included
Four studies were conducted in the United States (Georgiades et al., 2007; Gonzalez et al., 2010; Lustman et al., 1998; Safren et al., 2013), and one study was conducted in Puerto Rico (Rosselló and Jiménez-Chafey 2006). Van Bastelaar et al. (2011) conducted their research in Amsterdam. The total pooled sample size comprised 504 patients. Patients ranged in age from 13 to 70 years.
Three studies (Gonzalez et al., 2010; Lustman et al., 1998; Van Bastelaar et al., 2011) focused on type 2 diabetes patients. One study (Georgiades et al., 2007) focused on type 1 and type 2 diabetes patients. One study (Rosselló and Jiménez-Chafey 2006) focused on adolescents with type 1 diabetes.
Hierarchy of research design
Three studies (Lustman et al., 1998; Safren et al., 2013; Van Bastelaar et al., 2011) were randomised controlled trials, and two studies (Georgiades et al., 2007; Rosselló and Jiménez-Chafey, 2006) were quasi-experimental studies. Gonzalez et al. (2010) conducted a case series in which an intervention was administered to a small sample (N = 5) of participants. Both of the randomised controlled studies stipulated the randomisation technique used.
Quality assessment of studies
Two independent reviewers rated the quality of the papers (Table 2). Only one study (Safren et al., 2013) fulfilled all of the quality assessment criteria. Two studies (Gonzalez et al., 2010; Rosselló and Jiménez-Chafey, 2006) demonstrated poor methodology quality. These studies scored 3 and 4 points out of a possible 10 points, respectively. Due to the heterogeneous nature of the studies and the results reporting style, it was not possible to conduct a meta-analysis on the data obtained. The findings are therefore presented in narrative form.
Methodology quality of studies included.

Depressive measures
A range of measures was used across the studies in order to assess depression among diabetic patients. Four studies (Georgiades et al., 2007; Gonzalez et al., 2010; Lustman et al., 1998; Rosselló and Jiménez-Chafey, 2006) utilised the BDI (Beck et al., 1961). Rosello and colleagues did not find a significant difference in BDI scores. Lustman et al. (1998) and Georgiades et al. (2007) found a significant decrease in BDI scores (p < .001) from baseline levels to follow-up after the CBT intervention. Gonzalez et al. (2010) found that BDI scores were slightly less responsive, with one patient showing an increase. Another patient in this study showed no change from pre- to post-assessment. The three remaining patients reported decreases on the BDI.
Gonzalez et al. (2010) used an additional depressive measure, which was administered by the clinicians. The clinicians involved in this study completed the Montgomery–Asberg Depression Rating Scale (MADRS; Montgomery and Asberg, 1979), which is a structured 10-item questionnaire. This measure was utilised to measure specific symptoms of depression and to provide a rating of severity of depression over the last 7 days. All patients experienced a decrease in their MADRS score between the baseline and post. Georgiades et al. (2007) also used an additional measure, utilising the 17-item Hamilton Depression Scale (HAM-D; Hamilton, 1960). The HAM-D measurement of depression demonstrated reductions from the baseline to follow-up after CBT intervention (p < .001). Safren et al. (2013) also used the MADRS. These researchers also utilised Clinical Global Impression (Guy, 1976). Four-month follow-up indicated that after controlling for baseline, the cognitive behavioural therapy for adherence and depression (CBT-AD) arm had 6.22 lower depression scores on the MADRS than the control arm (95% confidence interval (CI): 2.33, 10.56; p = .002) and 0.74 lower ratings on the Clinical Global Impression (95% CI: 0.16, 1.32; p = .01), where lower scores indicate less depression on both scales.
Van Bastelaar et al. (2011) utilised the Dutch validated version of the Centre for Epidemiological Studies Depression Scale (CES-D). This is a self-report screening instrument, which measures the frequency with which participants have experienced specific symptoms of depression within the preceding week. The outcome of this randomised control trial indicated that the CBT group had a lower level of depressive symptoms at 1-month follow-up (d = 0.29, p < .001). Rosselló and Jiménez-Chafey (2006) utilised the Children’s Depression Inventory (CDI). This is a 27-item self-rated symptom-oriented scale suitable for school-aged children and adolescents (Kovacs, 1992). The findings indicated that depressive symptoms significantly improved after the intervention (p < .05).
HbA1c
All papers reviewed included a HbA1c measure. However, only three papers found significant findings. In the case series conducted by Gonzalez et al. (2010), findings indicated that all patients except for one experienced a decrease in HbA1c between the baseline and post-intervention. Two patients experienced a decrease in HbA1c from above 7 to below 7, which is the treatment goal for most patients. Lustman et al. (1998) found that post-treatment HbA1c levels were not different in the CBT and control groups, but 6-month follow-up mean HbA1c levels were significantly better in the CBT group than in the control group (9.5% compared with 10.9%; p = .03). Safren et al. (2013) found that the intervention group had superior glycaemic control as indicated by a 0.72 difference in A1C compared to the control group (95% CI: 0.29, 1.15; p = .001).
Georgiades et al. (2007) determined HbA1c using ion exchange HbA1c performance liquid chromatography, a methodology that measures only the A1c fraction of glycohaemoglobin (reference range: 4.3%–6.0%). Baseline tests were conducted in a clinical laboratory that met the requirements certified by the National Glycohemoglobin Standardization Program. To obtain comparison data, patients measured fasting blood glucose before breakfast for a 7-day period before each hospital visit. The patients were given an Accu-Chek Complete meter system (Roche Diagnostics, Indianapolis, IN, USA), and they were instructed in its proper use. The data were downloaded into a computer for analysis, and the mean fasting blood glucose level was calculated as the average of the fasting measurements completed within a week of each clinic visit. There were no significant changes in glycaemic control post-intervention.
In the study conducted by Rosselló and Jiménez-Chafey (2006), glycosylated HbA1c levels were obtained at pre- and post-intervention. HbA1c provides a measure of glycaemic control for the previous 2–3 months. Values above 8 per cent are classified as being an indicator of inadequate or poor metabolic control. There were no significant changes in glycaemic control post-intervention. Van Bastelaar and colleagues obtained HbA1c data from patients’ medical charts via their treating physician. There were no significant changes in glycaemic control post-intervention.
Other measures
Some studies included in this review included other outcome measures. For example, Van Bastelaar et al. measured diabetes-specific emotional distress using the Dutch version of the Problem Areas in Diabetes (PAID) Scale (Snoek et al., 2000). A significant treatment effect was found for PAID (p < .01). Rosselló and colleagues used various other outcome measures, such as the Hopelessness Scale for Children (HSC), which is a 17-item scale designed to measure cognitions of hopelessness defined as negative expectations about oneself and the future (Kazdin et al., 1983). They also utilised the Self-Efficacy for Diabetes Scale (SED), which is a 35-item scale designed to measure the self-perception or expectations of competence, power and resources for successful management of type 1 diabetes (Grossman et al., 1987). In addition, the authors also assessed diabetes self-care behaviours using the summary of self-care activities (SSCA), which is a self-report instrument used to measure adherence to diabetes treatment (Schafer et al., 1983) and the Piers–Harris Children’s Self-Concept Scale (PHCSCS), which provides an overview of an individual’s self-perception, consisting of 79 items to be answered ‘yes’ or ‘no’ (Piers and Harris, 1984). The outcome of this study indicated a significant treatment effect for SED (p < .05) and self-concept (p < .01).
Safren et al. (2013) included adherence to medication and glucose monitoring as their outcome measure. To measure medication adherence, each patient was given a Medication Event Monitoring System electronic pill cap, which fits on a medication bottle and registers each time the patient’s medication bottle is opened. This allowed for calculation of a percentage of doses taken. To measure adherence to glucose monitoring, OneTouch Ultra meters (LifeScan, Inc., Milpitas, CA, USA) for daily glucose control also provided frequency of self-monitoring, which, compared to the individualised goals from the nurse visits, also yielded a percentage adherence score.
CBT intervention
Although all studies included in this review were CBT interventions, the nature of the interventions was not homogeneous. Two studies used individual-session CBT (Gonzalez et al., 2010; Van Bastelaar et al., 2011), while three other studies used group-session CBT (Georgiades et al., 2011; Lustman et al., 1998; Rosselló and Jiménez-Chafey, 2006). Among the studies that delivered individual sessions, one was delivered face-to-face and one study used a web delivery method (Van Bastelaar et al., 2011). Moreover, the duration of the intervention also varied from one study to another, ranging from 8 to 16 sessions. The delivery of the therapy session also varied. For example, in the study conducted by Lustman et al. (1998), sessions were delivered by one psychologist. Georgiades et al. (2011) had a team of four psychologists, although sessions were led by one psychologist. In the study conducted by Gonzalez et al. (2010), sessions were delivered by a group of professionals, including a psychologist, a nurse educator and a dietician.
The content of the CBT interventions also varied vastly. Lustman et al. (1998) did not provide details of the content covered in their intervention. Georgiades et al. (2011) provided participants with training regarding information processing biases (i.e. mood congruent interpretations of events) on behaviour and affect. Participants in this study were taught to take an empirical approach to cognitions, whereby thoughts were evaluated against substantive objective information and alternative explanations for events were articulated. In addition, participants received guidance in communication, problem-solving and goal-setting skills. Rosselló and Jiménez-Chafey (2006) also trained patients on how thoughts affect mood. In addition, patients in this study learned about planning pleasant activities, time management and goal setting. Patients were also trained on establishing social support networks, communication skills and assertiveness.
Van Bastelaar et al. (2011) included stress and relaxation techniques, physical activity, anti-rumination techniques and relapse prevention within their CBT intervention. Gonzalez et al. (2010) used CBT-AD. Within this intervention, patients were trained on monitoring blood glucose levels and tracking dietary and physical activity behaviours that influence glucose levels. Within the CBT intervention, patients were also taught problem-solving skills and provided relaxation training such as diaphragmatic breathing and progressive muscle relaxation. Given the heterogeneous application of CBT in the studies included in this review, it is not possible to establish a best-practice model of delivery.
Discussion
A definitive conclusion cannot be drawn regarding the effectiveness of CBT for depressed diabetic patients, due to the issue of heterogeneity of the data between the studies. However, this narrative review provides a holistic interpretation of the findings. All studies reported that CBT had a positive impact on depressive symptoms. Half of the studies found an improvement in HbA1c and a further study demonstrated that CBT interventions improved self-efficacy and self-concept related to the successful management of diabetes in adolescents with type 1 diabetes. As depression among diabetic patients contributes towards a poorer quality of life, improvement in depressive symptoms has the potential to result in an improvement in this domain. In addition, depressed diabetic patients have demonstrated non-adherence to the diabetes treatment regimen and self-care behaviour. Although improvements in depressive symptoms might not impact directly upon HbA1c improvement, it seems plausible that it could impact positively upon adherence to the diabetes treatment regimen and self-care behaviour.
There are various aspects of diabetes management, which include managing the relationships between food, physical activity, medication, self-monitoring of blood glucose, blood pressure and regular retinal screening. In addition, of great importance is the targeting of goals tailored to individual needs, for example, in the areas of foot care, weight loss, injection techniques and managing acute complications, such as hypoglycaemia and hyperglycaemia. Therefore, poor glycaemic control could be attributed to diabetic management factors. Only one study (Safren et al., 2013) examined these factors. Poor glycaemic control could also be attributed to poor knowledge and understanding of diabetes management. Diabetes education was only provided to patients in one study (Lustman et al., 1998). It is possible that an improvement in HbA1c was not observed across the studies due to patients’ lack of knowledge regarding diabetes management.
Studies included in this review reported various methodological issues. Only half of the studies had long-term follow-up of more than 6 months. Thus, it is difficult to establish if the impact of CBT interventions was maintained for a longer period of time. Only three studies included in this review observed a significant decrease in the HbA1c level. However, it is noteworthy that the review lacked large, long-term follow-up studies. The studies that did not find a significant decrease in the HbA1c level did not have long-term follow-up. It is possible that not enough time had elapsed between HbA1c assessments to detect a significant change.
This review clearly highlights the need for more controlled studies with longer term follow-up and with larger sample sizes, to ascertain with certainty the effectiveness of CBT for depressed diabetic patients. In addition, the cost-effectiveness of this therapy as a treatment option for depressed diabetic patients also needs investigation.
In recent years, CCBT has been used to treat depression. One of the major advantages of CCBT is the ability to provide more treatment choices for patients and faster access to effective mental health services. Increasingly, more research is being conducted on CCBT for depressed diabetic patients. Further research on the effectiveness of tailored computerised CBT for depressed diabetic patients is needed.
Conclusion
This review highlights the need for more studies that focus on CBT for depressed diabetic patients. Depression among diabetic patients is a major public health concern. Therefore, it is pivotal to conduct high-quality research to establish the most effective psychological treatment options to address this issue.
Footnotes
Acknowledgements
The authors would like to acknowledge the contribution of Dr Parmpreet Kalsi who served as a second reviewer on this systematic review.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.