
Abstract
This study aims to explore correlates between body appreciation and mental health among a racially and ethnically diverse sample of adult women using validated measures. The sample included racially and ethnically diverse women (N = 497) from various socioeconomic levels. Linear regression results indicated that body appreciation was significantly and inversely associated with depression (b = −3.68; p < 0.001). In this sample, as body appreciation increased, depression scores decreased. Similarly, body appreciation was significantly and inversely associated with anxiety among this sample (b = −1.78; p < 0.001). This article concludes with a discussion of findings and implications.
Introduction
Body appreciation is a multifaceted construct that encompasses multiple components of body image (Tylka and Wood-Barcalow, 2015b). These elements include respect for and protection of one’s body by attending to its needs and engaging in healthy behaviors, having favorable opinions of one’s body, and acceptance of one’s body regardless of shape or size, as well as rejection of unrealistic body standards (i.e. the thin ideal; Avalos et al., 2005). Multiple studies in the growing field of body appreciation research have shown that it is not simply the inverse of body dissatisfaction but rather a separate and unique construct that should not be viewed on the same continuum as negative body image (Tylka and Wood-Barcalow, 2015a).
Studies have documented associations between positive body image and protective mental and physical health behaviors that are not solely attributed to the absence of negative body image (Andrew et al., 2016; Avalos et al., 2005; Williams et al., 2004). In sum, these studies illustrate that body appreciation is an important construct to study in relation to mental health.
Theoretical framework
Objectification and homeostasis theories provided a foundation for this study. Developed by Fredrickson and Roberts in 1997, objectification theory suggests that when women experience cultural sexual objectification, they turn this objectification theory inward, called self-objectification. Self-objectification is, according to objectification theory, associated with body shame, appearance anxiety, depression, eating disorders, and more (Fredrickson and Roberts, 1997). Homeostasis theory is also particularly relevant to this study. According to Marks (2015), obesity results from a homeostatic imbalance between body dissatisfaction, negative affect, increased body weight, and consumption, which he refers to as the circle of discontent. Conversely, when one maintains a homeostatic balance, then one is achieving a circle of content. Marks (2016) suggests there are many opportunities for intervention in this dyshomeostasis, such as promoting the acceptance of diverse bodies.
Body appreciation and mental health
While research on the health-related outcomes and positive body image is still limited, early findings suggest that it may significantly influence the mental health and well-being for women. Research suggests body appreciation is related to a number of factors associated with psychological well-being, including self-esteem, healthy coping mechanisms, positive affect, and optimism (Avalos et al., 2005; Swami et al., 2009; Tylka and Kroon Van Diest, 2015; Tylka and Wood-Barcalow, 2015a). In a cross-sectional study on the association between body appreciation and mental health indicators among a diverse sample of college students, those with higher body appreciation reported fewer depressive symptoms and higher self-esteem (Gillen, 2015). This relationship held true even when controlling for effects of body mass index (BMI). In other words, individuals with a greater degree of positive body image also experienced better mental health regardless of actual body size (Gillen, 2015).
Collectively, results from these studies suggest that body appreciation is associated with various positive indices of psychological well-being, which may also afford some level of resilience to the detrimental effects of media exposure on women’s self-image (Avalos, Tylka, and Wood-Barcalow, 2005; Jauregui-Lobera and Rios, 2011). However, few studies utilize diverse samples of women, and no known studies include anxiety as a dependent variable.
Possible confounders
Body image is a complex construct influenced by several factors, including age, race, BMI, and socioeconomic status (SES). A study on the relationships between positive body image, body dissatisfaction, and age showed that age influenced the strength of the association between positive and negative body image (Tiggemann and McCourt, 2013). As with age, other variables, such as race (Grabe and Hyde, 2006), BMI (Schwartz and Brownell, 2004), and SES (Ramseyer Winter, Cahill, and Koegler, under review), may also influence body appreciation and body dissatisfaction. A study looking at the relationship between positive body image and health indicators found Blacks, African Americans and those with lower BMI have a greater appreciation for their bodies (Gillen, 2015). Lower SES has also been associated with slightly higher levels of body appreciation among adolescents and does not change significantly with age (Van Den Berg, 2010). As such, we controlled for age, race, BMI, and SES in all analyses.
Purpose
The purpose of this study is to fill the aforementioned gaps by investigating the associations between body appreciation, depression, and anxiety among a racially, ethnically, and socioeconomically diverse sample of adult women using previously validated scales. Specifically, we hypothesized that women with greater body appreciation would report lower levels of depression and anxiety, after controlling for BMI, age, race, and SES.
Method
Participants
The sample included racially and ethnically diverse women (N = 497). The sample identified as 27.6 percent non-Hispanic White, 22.9 percent non-Hispanic Asian, 19.1 percent non-Hispanic Black, 13.1 percent Hispanic/Latina, and 17.3 percent selected Hispanic/Latina and at least one other category. The mean age was 26.24 years (range = 18–56; standard deviation (SD) = 6.15) and the mean BMI was 26.33 (SD = 7.33), which is in the “overweight” range according to the CDC (n.d.). This is possibly due to the diverse nature of the study, as Black and Latina women, on average, have a higher BMI than White women (e.g. Rahman et al., 2009). Regarding SES, 14.5 percent of the sample identified as poor, 13.9 percent as working class, 21.2 percent as lower middle class, 14.9 percent as middle class, and 35.5 percent as upper middle class/upper class/wealthy. The sample was well educated with over half reporting their highest degree or level of school as having a bachelor degree or graduate degree (54.6%), 26.7 percent had some college, 10.6 percent were high school graduates, and only 0.2 percent reported having less than a high school education. See Table 1 for a full list of participant characteristics and study indicators.
Participant’s characteristics and study indicators (N = 497).

BMI: body mass index; BAS: Body Appreciation Scale; GAD-7: sum score of the Generalized Anxiety Disorder scale; PHQ-9: sum score of the Patient Health Questionnaire.
Procedure
This study is part of a larger study focused on body image and sexual health. The first author, after receiving Institutional Review Board (IRB) approval, recruited the convenience sample during the summer of 2016 through www.reddit.com (Reddit). Reddit is an online bulletin board where members can post to thousands of subreddits (smaller “bulletin boards”) by topic area. Although the sample is not representative of the United States, every attempt was made to recruit a diverse sample of women. To recruit a racially diverse sample, the study advertisement with a link to the online survey was posted in subreddits that related to women of color, such as /r/blackladies. When participants clicked on the link, they were taken to the qualifying questions in Qualtrics. They were asked three questions to determine their eligibility before providing consent to participate. Inclusion criteria included the following: (1) 18-year-old or older, (2) identify as a woman, and (3) identify as at least one of the following races/ethnicities: White/Caucasian, Black, Hispanic/Latina, Asian American. Participants who qualified were taken to an online consent form that included additional resources on health and body image, and if they agreed to participate, they were then taken to the full survey. At the end of the survey, participants were prompted to click on a link to a separate survey where they had the option to provide their email address if they wanted to be entered in the drawing for one of 15 US$50 gift cards. Email addresses were collected in a separate survey to allow for anonymity.
Measures
Body appreciation
The independent variable, body appreciation, was assessed with the Body Appreciation Scale-2 (BAS-2; Tylka and Wood-Barcalow, 2015a). The BAS-2 is a 10-item scale including items such as “I appreciate the unique characteristics of my body” and “I feel that my body has at least some good qualities.” Response options ranged from never (1) to always (5). The reliability of the BAS-2 among the current sample is estimated to be high (α = 0.92). We computed a body appreciation score with a higher score reflecting higher body appreciation.
Depression
The first outcome variable, depression, was measured using the Patient Health Questionnaire-9 (PHQ-9; Kroenke and Spitzer, 2002). Although the PHQ-9 was designed for primary care settings, it has been validated in general population samples (Martin et al., 2006). This 9-item scale includes items such as “Over the last 2 weeks, how often have you been bothered by any of the following items? Little interest or pleasure in doing things.” Response options included not at all, several days, more than half the days, and nearly every day. A PHQ-9 score is computed by multiplying the number of times participants responded with not at all by 0, several days by 1, more than half the days by 2, and nearly every day by 3 and then summing these numbers. The possible range of the PHQ-9 score is 0–27. A score of 0–4 indicates minimal depression, 5–9 is mild depression, 10–14 suggest moderate depression, 15–19 is moderately severe depression, and a score of 20–27 indicates severe depression. The reliability of the PHQ-9 among the current sample is estimated to be acceptable (α = 0.88).
Anxiety
We measured anxiety with the Generalized Anxiety Disorder 7-item scale (GAD-7; Spitzer et al., 2006). A sample item is “Over the last 2 weeks, how often have you been bothered by the following problems? Not being able to stop or control worrying.” Response options included not at all (0), several days (1), over half the days (2), and nearly every day (3). The responses were summed to create a GAD-7 score with a higher score indicating a higher level of anxiety, such as a score of 10 indicating moderate anxiety and 15 indicating severe anxiety. The reliability of the GAD-7 among the current sample is estimated to be high (α = 0.91).
Covariates
Covariates were selected based on the literature review. We controlled for body size, race, SES, and age in the analyses.
Body size
Body size was measured by computing BMI from self-reported height and weight (weight (lb)/(height (in))2 × 703). BMI was included as a continuous variable in the models.
Race
Race was collected with one item: “How do you identify your race/ethnicity (select all that apply).” Response options included the following: White/Caucasian; Black (African American, Caribbean American, Creole, Haitian, Jamaican, West Indian, Brazilian, Ethiopian, Somali, Kenyan, and Other (please specify)); Hispanic/Latina (Mexican descent, Caribbean decent, Central American decent, South American decent, and Other (please specify)); and Asian (East Asian decent (Chinese, Japanese, Korean), Southeast Asian decent (Filipino, Vietnamese, Cambodian, Hmong), South Asian decent (Asian Indian, Pakistani, Nepalese), and Other (please specify)). Due to a lack of variance in the subcategories, we collapsed this variable to include the following race categories: White, Black, Asian, Latina, and multiracial.
SES
We measured SES with the following item: “Taking all of the income sources available to you into account, how would you describe your current economic class?” Response options included the following: poor (US$0–US$12,500 annually), working class (US$12,501–US$21,000 annually), lower middle class (US$21,001–US$41,500 annually), middle class (US$41,501–US$53,500 annually), upper middle class (US$53,501–US$150,000 annually), and upper class/wealthy (US$150,001+). These were collapsed into the following categories: poor, working class, middle class, upper middle class/upper class/wealthy.
Age
We measured age by asking participants “How old are you (in years)?” Age was included in all models as a continuous variable.
Analytical plan
Prior to running multiple regression analyses, we conducted bivariate correlation analyses. These analyses revealed a significant correlation between BAS score and PHQ-9 score (r = −0.45, p < 0.001), BAS score and GAD-7 (r = 0.28, p < 0.001). We ran two linear regressions using IBM SPSS version 24. We included all covariates in both models. Refer to Table 2 for a full list of regression statistics.
Regression results.
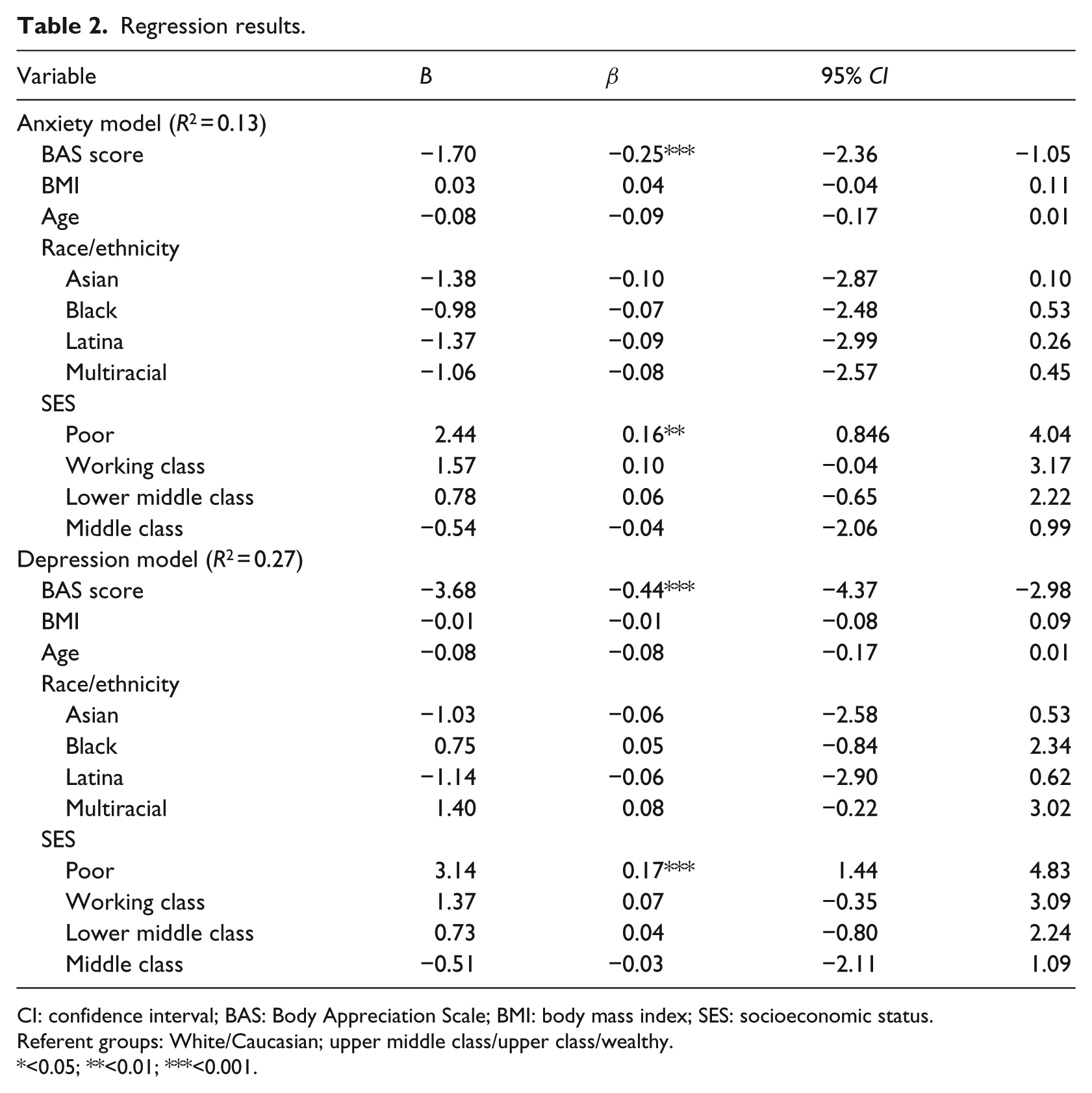
CI: confidence interval; BAS: Body Appreciation Scale; BMI: body mass index; SES: socioeconomic status.
Referent groups: White/Caucasian; upper middle class/upper class/wealthy.
<0.05; **<0.01; ***<0.001.
Results
Depression
Depression was regressed on body appreciation, body size, race, SES, and age. The regression model was statistically significant (F(11,454) = 15.02, p < 0.001) and accounted for 27 percent (R2 = 0.27) of the variance in depression among this sample. Body appreciation was significantly and inversely associated with depression (b = −3.68; β = −0.44; t(454) = −10.42; p < 0.001; confidence interval (CI) = −4.37 to −2.98). The results indicate that as body appreciation increased, depression scores decreased. Participants who reported being poor had higher depression scores (b = 3.14; β = 0.17; t(454) = 3.63; p < 0.001; CI = 1.44–4.83) than participants who identified their SES as upper middle class/upper class/wealthy. None of the other covariates were significantly related to depression among this sample.
Anxiety
Anxiety was regressed on body appreciation, body size, race, SES, and age. The regression model was statistically significant (F(11,405) = 5.45, p < 0.001) and accounted for approximately 13 percent (R2 = 0.13) of the variance in anxiety scores among this sample. Body appreciation was significantly and inversely associated with anxiety (b = −1.70; β = −0.25; t(405) = −5.09; p < 0.001; CI = −2.36 to −1.053), indicating that as body appreciation increased, anxiety scores decreased. In addition, poor participants had higher anxiety scores when compared to upper middle class/upper class/wealthy participants (b = 2.447; β = 0.16; t(405) = 2.99; p = 0.003; CI = 0.84–4.05). None of the other covariates were significantly related to anxiety among this sample.
Discussion
In this study, we examined associations between body appreciation and mental health among a community sample of racially/ethnically and socioeconomically diverse women. In support of prior work (Tylka and Wood-Barcalow, 2015b), results show that body appreciation was significantly associated with indicators of better mental health. Specifically, women who had higher body appreciation experienced less depression and anxiety. Other research has demonstrated similar negative associations between body appreciation and depression among both male and female college students from the United States (e.g. Gillen, 2015). The current findings support and extend this literature to include anxiety and by illustrating that these associations are present in a community sample of adult women from diverse racial, ethnic, and socioeconomic backgrounds.
Individuals with higher body appreciation may be more health-conscious individuals, who not only value their physical selves but also invest in their emotional health (Gillen, 2015). Self-compassion and self-care behaviors are related to body appreciation and positive body image (Tylka, 2011; Wasylkiw et al., 2012), as well as to physical and psychological well-being. For example, self-compassion may include being kind to oneself when unsuccessfully trying to eat more healthfully or exercise more. Showing compassion and understanding in this context may prevent feelings of dejection and anxiety as well as preserve or promote appreciation for one’s body. This is significant to this study as self-compassion is, in fact, linked to fewer symptoms of depression among college women (Wasylkiw et al., 2012). Self-care is also associated with physical and mental health, and may prevent negative outcomes including the onset of mental illness symptoms (Cook-Cottone, 2014).
Self-care may include behaviors such as meditation, running, engaging in personal hobbies, engaging in social activities, or preparing healthy foods. This is significant to this study due to the associations between self-care and mental health as well as self-care and body image. For example, a study conducted in a non-profit community pharmacy measured the effectiveness of self-care practices among those with existing mental health conditions and discovered the majority of participants engaged in the self-care activities listed above with over 98 percent showing improvement in mental health (Bible, 2017). Positive body image has also been associated with participating in self-care activities. In Gillen’s (2015) study, positive body image increased the likelihood of engaging in self-care activities such as preparing healthy foods, using protection against ultraviolet light exposure, and regularly getting tested for sexually transmitted infections. Self-care may also include seeking help for physical or mental health problems from a medical professional or therapist when needed. These behaviors may, in turn, prevent the onset of depression and anxiety or may lessen their severity. Thus, it is possible that through greater attentiveness to physical and mental health, individuals with higher body appreciation experience less depression and anxiety.
Furthermore, having a lower income predicted depression and anxiety. Lower income groups are at greater risk of mental health problems, including depression (Hudson, 2005). Stress related to having less income may increase feelings of dejection and hopelessness and therefore may elevate risk of depression. Interestingly, despite the fact that there are significant differences in depression by race (e.g. Lincoln et al., 2014; Shao et al., 2016; Williams et al., 2007) and that there are significant differences in body image by race (e.g. Grabe and Hyde, 2006), race and ethnicity did not contribute significantly to either model. In sum, being poor significantly increases the likelihood of experiencing depression and anxiety and, therefore, decreases the likelihood of body appreciation.
This study should be considered in the context of its limitations. Participants were recruited from users of a website who may not represent the general population of women. On this website, those who were more interested in a questionnaire about body image and sexual health self-selected to participate. Also, the correlational nature of the study cannot generate firm conclusions about the directionality of associations between body appreciation and mental health. Feeling greater appreciation for one’s body may lead to less depression and anxiety, but individuals who are less depressed and anxious may also develop higher body appreciation. In spite of these limitations, this study adds to the growing literature on positive body image through its inclusion of a large, diverse sample of community women. Results demonstrate that body appreciation is associated with indicators of better mental health among women, including less anxiety and depression. Intervention programs that aim to improve women’s appreciation for their bodies may have broader implications for their mental health.
Conclusion
Past research has described associations between body appreciation and mental health. Due to a need for more literature in this area, associations between body appreciation and mental health were further explored among a racially diverse sample of women. It was hypothesized that women with greater body appreciation will report lower levels of depression and anxiety. Our results indicate that body appreciation was significantly associated with indicators of better mental health. As body appreciation increased, anxiety and depression decreased within this sample. This research suggests that strategies to promote body appreciation in women may also improve mental health.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The author(s) received financial support from the Margaret W. Mangel Faculty Research Catlyst Fund through the College of Human Environmental Sciences at the University of Missouri.