
Abstract
Researchers have seldom compared how various psychological factors relate to men’s sexual health. We sought to identify whether and how psychological risk factors (i.e. anxiety sensitivity, emotion regulation, psychological distress) predict men’s sexual health (i.e. functioning, sexual quality of life, frequency of sexual activity). Men (N = 306) completed an online survey measuring emotional, psychological, and sexual outcomes. Comparisons of four path analysis models suggested that psychological risk factors are related to some but not all sexual health markers. We will highlight the factors that may place young men at risk for developing mental and sexual health difficulties.
The World Health Organization has defined sexual health as “a state of physical, emotional, mental and social well-being in relation to sexuality; it is not merely the absence of disease [or] dysfunction” (Glasier et al., 2006). Research on men’s sexual health as it relates to sexual functioning (e.g. difficulties with desire, erection) is plentiful (e.g. Patrick et al., 2005; Ponholzer et al., 2005). However, there is less research that examines multiple dimensions of men’s sexual health together. Moreover, few studies have explored the psychological and emotional variables that may underlie sexual health outcomes in men (e.g. Carvalho and Nobre, 2011; Dunn et al., 1999). Mental and sexual health are often assessed and treated as separate difficulties (Nobre and Pinto-Gouveia, 2006). However, mental and sexual health likely impact each other to a larger degree than is currently understood. Thus, assessments and interventions for these difficulties would benefit from addressing both aspects of overall health, rather than just one. Recently, we examined the role of anxiety sensitivity (AS), emotion regulation (ER), and psychological distress as psychological risk factors on young women’s sexual health (Tutino, Ouimet, & Shaughnessy, 2017). Our findings were consistent with the large body of research in which mental and sexual health relate with and predict each other (e.g. Atlantis and Sullivan, 2012; Prince et al., 2007). In this study, we sought to replicate and extend our findings to men. Specifically, the goal of our study was to identify how psychological risk factors, such as AS, emotion regulation, and psychological distress, predict distinct, but related sexual health outcomes in men.
Sexual outcomes
The term “sexual health” encompasses more than just sexual functioning. Sexual quality of life and frequency of sexual activity are additional components of sexual health that are assessed with much less frequency in men compared to sexual functioning. Sexual dysfunction is defined as the difficulty with or absence of any of the following: desire, arousal, erection, or orgasm accompanied by distress or impairment (American Psychiatric Association, 2013). Sexual quality of life involves the subjective interpretation of one’s sexual experiences in terms of satisfaction or quality. In men, higher sexual quality of life is related to factors such as greater commitment and intimacy (Yela, 2012). Frequency of sexual activity refers to the regularity with which one engages in any kind of sexual activity, be it partnered (e.g. foreplay, oral sex, penetrative sex) or solitary (e.g. masturbation, fantasizing, watching pornography alone). Although these markers of sexual health represent different facets of sexual experiences, they are not mutually exclusive and may influence one another. Indeed, men tend to report greater sexual quality of life with greater frequency of sexual activity (Muise et al., 2016; Yela, 2012) and increased sexual functioning (Nicolosi et al., 2004).
Sexual outcomes and psychological risk factors
Psychological, emotional, and environmental risk factors may place men at risk for experiencing difficulties in one or all three areas of sexual health. Research demonstrates that symptoms of psychopathology (e.g. anxiety and depression) can negatively affect sexual health and well-being (Barlow, 1986; Frohlich and Meston, 2002). Mental health difficulties such as anxiety and depression, and personality traits such as neuroticism, are more prevalent in women (e.g. Gater et al., 1998; Kessler et al., 2005; Lewinsohn et al., 1998). Therefore, the impact of these mental health difficulties on the sexual health of women may be more salient (and thus, more widely researched). However, many men who report symptoms of psychological distress also report sexual difficulties (Araujo et al., 1998; Kennedy et al., 1999). Indeed, researchers have found that men with greater symptoms of depression reported less sexual satisfaction and greater prevalence of erectile dysfunction (Nicolosi et al., 2004). Moreover, in a sample of participants with depression who were not taking antidepressant medication, Kennedy et al. (1999) found that over 40 percent of men and 50 percent of women reported decreased sexual interest and activity. Given that symptoms of psychopathology likely impact the sexual lives of men, it is possible that there are factors that place men at greater risk for the development of both mental and sexual health problems.
AS is one such risk factor. AS is the fear of the bodily sensations associated with anxiety because of their potential catastrophic outcomes (Reiss, Peterson, Gursky & McNally,1986). Although AS is a long-established risk factor for psychological distress (particularly anxiety), researchers only recently demonstrated that it also predicts sexual health problems. Specifically, Gerrior et al. (2015) found that women higher in AS reported greater sexual dysfunction and lower sexual satisfaction than women lower in AS. It is possible that the overlap in physiological sensations between anxiety and sexual arousal (e.g. increased heart rate, shallow breathing) partly explains this finding. However, our own research with women revealed that AS only predicted difficulties with arousal and pain—two facets of sexual functioning that have distinguishable physiological components (i.e. lubrication, pain sensations; Tutino et al., 2017).
No studies to date have examined the influence of AS on men’s sexual outcomes. Researchers have found that men and women responded similarly on the Anxiety Sensitivity Index (ASI; Reiss et al., 1986) overall, on the cognitive (e.g. “When my thoughts seem to speed up, I worry that I might be going crazy”) and on the social concerns (e.g. “When I begin to sweat in a social situation, I fear people will think negatively of me”) subscales (Armstrong and Khawaja, 2002; Stewart et al., 1997); however, women endorsed greater fears of physical concerns compared to men (e.g. “It scares me when my heart beats rapidly”). Given that men with high AS may focus less on the meaning of physical sensations than women, the influence of AS on sexual outcomes in men remains unclear. On one hand, AS may not predict sexual outcomes for men. On the other hand, it may be that AS still poses a risk factor for sexual difficulties in men, but to a lesser degree or in a different way than it does for women.
AS often co-occurs with difficulties regulating emotions in an adaptive way (Kashdan et al., 2008; Ouimet et al., 2016). People regulate their emotions in a variety of ways, and the strategies that they use can either be adaptive or maladaptive. If, for example, a person experiences a surge in their physiological sensations, they may engage in rumination over what these physiological sensations mean (a maladaptive emotion regulation strategy). In both men and women, maladaptive emotion regulation strategies are associated with poorer mental health outcomes (e.g. anxiety, depression; Garnefski et al., 2004; O’Neill et al., 2004). In our previous research with women, we found that the presence of higher AS and more difficulties with emotion regulation increased the likelihood of experiencing symptoms of psychopathology, and in turn, more negative sexual health outcomes (Tutino et al., 2017). Therefore, the presence of maladaptive ER strategies in conjunction with high AS may exacerbate both mental and sexual health difficulties. However, researchers have found that women engage in these maladaptive emotion regulation strategies more frequently than men (Garnefski et al., 2004). Research is needed to identify whether emotion regulation predicts the development of mental and sexual health difficulties in similar ways for men.
This study
We sought to investigate the role of three psychological risk factors (i.e. AS, emotion regulation, symptoms of psychopathology) in predicting men’s sexual health across three dimensions (i.e. sexual functioning, sexual quality of life, and frequency of sexual activity). We hypothesized that AS, psychological distress, and emotion regulation would predict all three sexual outcomes in men. We also had three research objectives: (1) to replicate and extend Gerrior et al. (2015) and Tutino et al. (2017)’s findings that AS is a significant psychological risk factor for sexual health difficulties, (2) to identify whether the relationship between AS and sexual health is mediated by symptoms of psychological distress (e.g. anxiety, depression), and (3) to explore how emotion regulation contributes to the relationship between AS, psychological distress, and sexual outcomes.
Method
Participants and procedures
Following institutional review board approval, we recruited 306 men through the undergraduate participant pool at the University of Ottawa in Canada, ranging in age from 17 to 47 years (M = 19.97, SD = 3.62). To participate, the men must have reported having engaged in partnered (i.e. caressing, foreplay, oral sex, penetrative sex) or solitary (i.e. self-stimulation, sexual fantasies) sexual activity in the 4 weeks prior to the study. Participants were compensated with course credit. All participants actively consented to the research on a webpage describing the study prior to beginning the survey. Participants reported being primarily White (68.6%), heterosexual (86.6%), and most were single (49.7%). They completed an online questionnaire package consisting of a sociodemographic questionnaire, followed by the ASI-3 (Taylor et al., 2007), Difficulties in Emotion Regulation Scale (DERS; Gratz and Roemer, 2004), Depression Anxiety Stress Scales (DASS; Lovibond and Lovibond, 1995), Male Sexual Function Index (MSFI; Kalmbach et al., 2012), Sexual Quality of Life Scale–Male Version (SQoL-M; Abraham et al., 2008), and Sexual Experiences Questionnaire (SEQ), which were presented in a randomized order. A total of 12 participants were excluded from analyses, as they did not complete one or more of the measures. Missing data on the scale scores were low, 1.6 percent on the DASS, 0.98 percent on the DERS, and no missing data on the remaining scales. Given the small amount of missing data, we used expectation maximization to impute values for these items.
Measures
Sociodemographic questionnaire
The sociodemographic questionnaire comprised 15 items related to demographic information (e.g. gender, sexual orientation) and background (e.g. number of lifetime romantic relationships).
ASI-3
The ASI-3 is a reliable and valid 18-item measure that assesses three facets of AS: cognitive concerns (e.g. “It scares me when I am unable to keep my mind on a task”), physical concerns (e.g. “It scares me when my heart beats rapidly”), and social concerns (e.g. “I worry that other people will notice my anxiety”) (Taylor et al., 2007). Participants rated the degree to which they agreed with the statements on a 5-point Likert scale (0 = very little, 4 = very much). Because research suggests that men and women differ on their ASI subscale scores (Armstrong and Khawaja, 2002; Stewart et al., 1997), we examined bivariate correlations between the total score and subscale scores of the ASI-3 on one hand and the sexual outcomes on the other hand. All correlations were significant and in the same direction for each sexual outcome. Therefore, and to be consistent with other research using the ASI-3 (e.g. Gerrior et al., 2015), we used the total score in our analyses. Higher scores indicated a higher degree of AS. We present internal consistency for all measures in the current sample in Table 2.
DASS
The DASS is a reliable and valid 42-item measure comprising three subscales (14 items each), measuring depression (e.g. “I felt I wasn’t worth much as a person”), anxiety (e.g. “I felt scared without any good reason”), and stress (e.g. “I found it hard to wind down”) (Lovibond and Lovibond, 1995). Participants rated the degree to which they agreed with statements on a 4-point Likert scale (0 = did not apply to me at all, 3 = applied to me very much, or most of the time). Higher scores indicated a greater endorsement of symptoms of psychopathology. We used total scores as a measure of general psychological distress.
DERS
The DERS is a reliable and valid 36-item measure that comprises six subscales (six items each), measuring diverse aspects of emotion regulation: Non-acceptance of Emotional Responses (e.g. “When I’m upset, I feel guilty for feeling that way”), Difficulties Engaging in Goal-directed Behavior (e.g. “When I’m upset, I have difficulty focusing on other things”), Impulse Control Difficulties (e.g. “When I’m upset, I feel out of control”), Lack of Emotional Awareness (e.g. “I am attentive to my feelings”), Limited Access to Emotion Regulation Strategies (e.g. “When I’m upset, my emotions feel overwhelming”), and Lack of Emotional Clarity (e.g. “I have no idea how I am feeling”) (Gratz and Roemer, 2004). Participants rated their degree of agreement with each statement on a scale of 1 (almost never, 0%–10%) to 5 (almost always, 91%–100%). Higher scores indicated greater difficulties with emotion regulation. We used total scores as a general measure of ER abilities.
MSFI
This reliable and valid 16-item measure comprises four subscales assessing diverse aspects of male sexual functioning: desire, arousal, erection, and orgasm (Kalmbach et al., 2012). A fifth subscale measuring sexual satisfaction was not used in this study, so as to not confound sexual satisfaction with sexual functioning difficulties. Moreover, the female version of this scale includes an additional subscale of functioning to measure sexual pain (Rosen et al., 2000); we added adaptations of these three items to measure men’s sexual pain. 1 Participants rated their degree of agreement with each statement as it applied to them over the past 4 weeks (e.g. “Over the past 4 weeks, how often did you feel sexually aroused (“turned on”) during sexual activity or intercourse?”). Each item is scored on a 5- or 6-point Likert scale. Higher scores indicated greater sexual functioning. We used total subscale scores (with the exception of sexual satisfaction) as measures of sexual functioning.
SQoL-M
This reliable and valid 11-item measure assesses aspects of sexual quality of life (Abraham et al., 2008). Sample items include “When I think about my sexual life, I feel like less of a man,” “When I think about my sexual life, I feel depressed,” and “When I think about my sexual life, I worry that my partner feels hurt or rejected.” Each item is rated on a 6-point Likert scale (1 = completely agree, 6 = completely disagree). Higher scores indicated greater sexual quality of life. We used total scores as a measure of sexual quality of life.
SEQ
The SEQ is a 12-item measure that was created for this study to assess the frequency of men’s recent sexual activity (both partnered and solitary). The items used in this survey were based on previous measures of sexual activity frequently used in research (e.g. Randall and Byers, 2003). Participants rated the number of times they had engaged in each sexual act in the past 4 weeks on a 6-point Likert scale (e.g. “I have never done this activity” to “8 times or more”). Higher scores indicated higher frequency of sexual activity. We conducted an exploratory factor analysis 2 to examine the factor structure of the scale. Items loaded onto two subscales: solitary (e.g. “Masturbated or sexually self-stimulated alone”), and partnered (e.g. “Inserted penis into vagina”) sexual activity subscales, confirmed with factor analysis.
Results
Data analysis
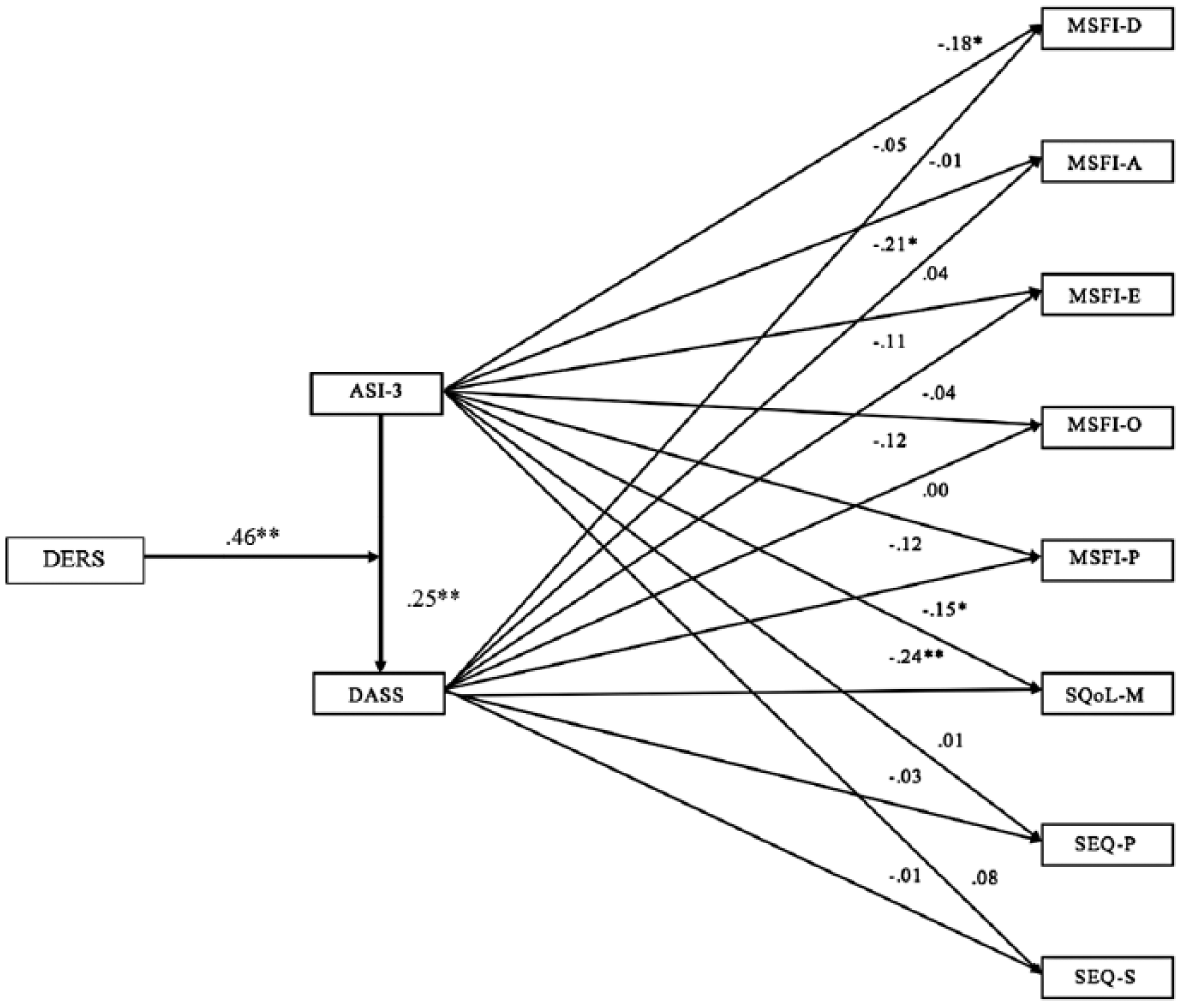
We present our sample characteristics in Table 1. Descriptive statistics for all measures included in our models are shown in Table 2. We calculated correlations (see Table 3) to assess relationship strength among all variables. We conducted path analyses using SPSS AMOS for all four models. 3 In Model 1, the predictor variable was AS. In Model 2 (see Figure 1), the predictor variables were AS and psychological distress. In Model 3 (see Figure 2), we entered ER as a mediator variable between AS and psychological distress. In Model 4 (see Figure 3), we entered ER as a moderator variable impacting the relationship between AS and psychological distress. For all four models, we entered the subscale sexual functioning scores, sexual quality of life, and frequency of partnered and solitary sexual activity separately as the outcome variables.
Sample characteristics.
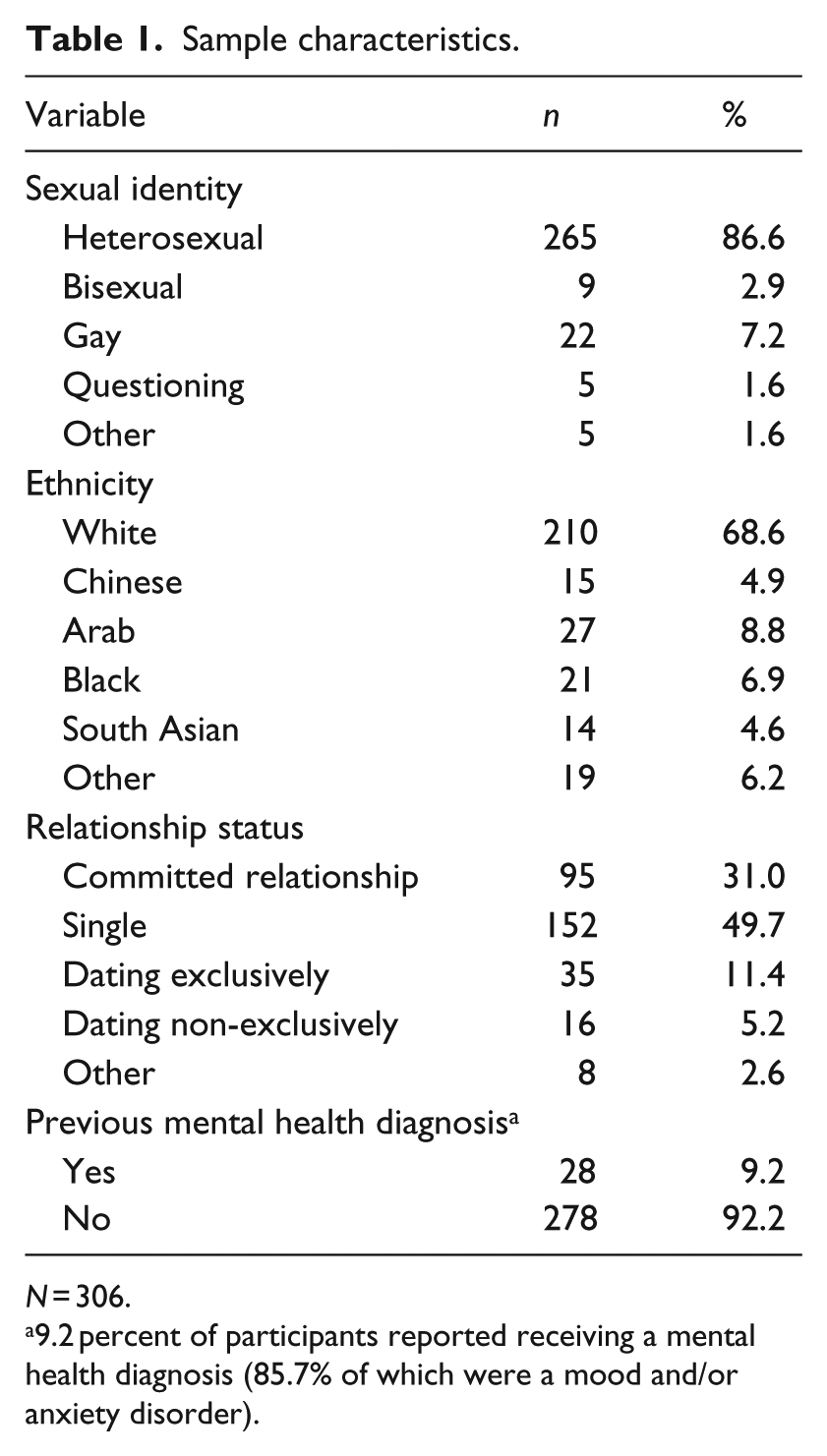
N = 306.
9.2 percent of participants reported receiving a mental health diagnosis (85.7% of which were a mood and/or anxiety disorder).
Means, standard deviations, minimum value, maximum value, and Cronbach’s alpha for study variables.
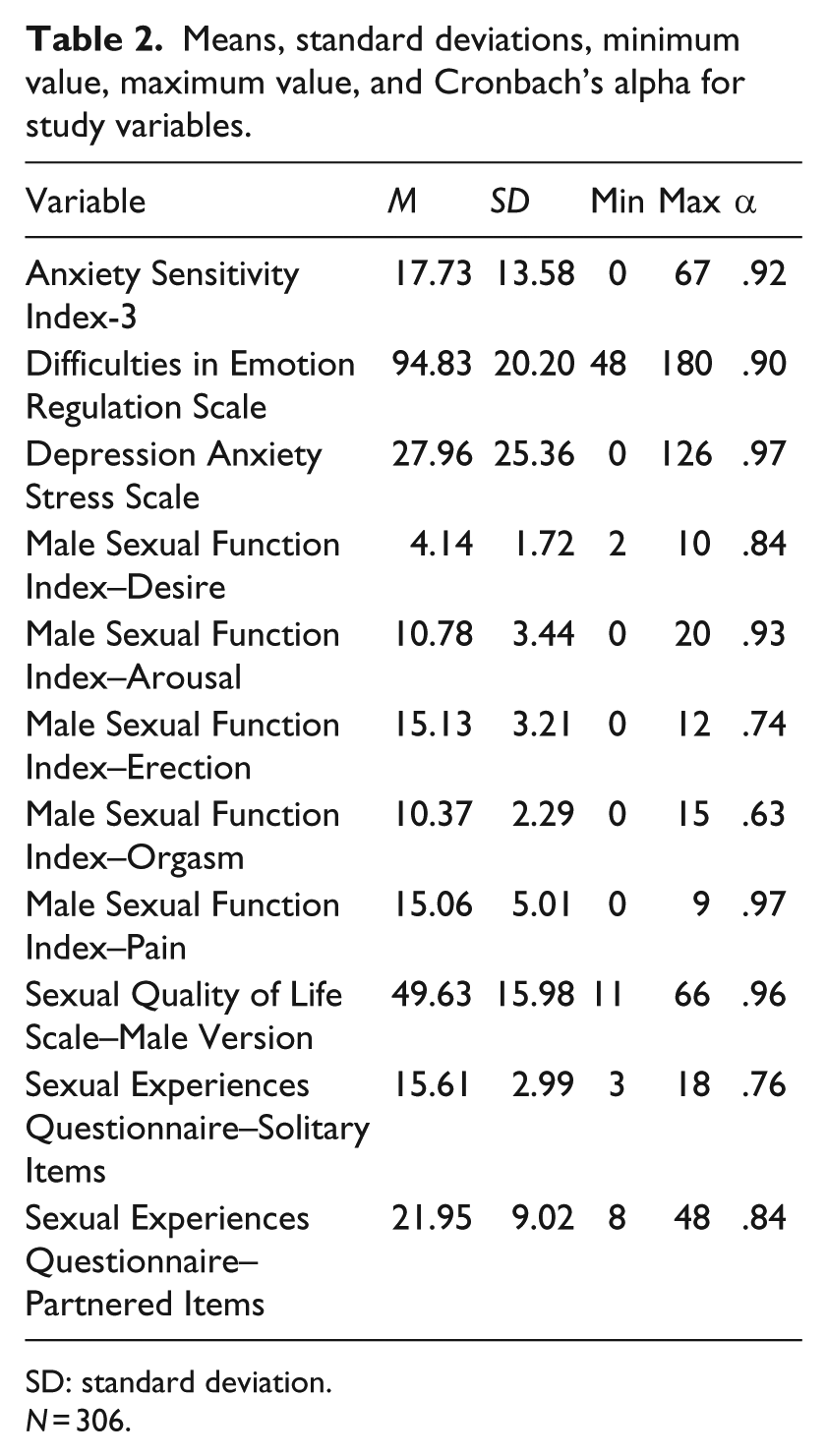
SD: standard deviation.
N = 306.
Correlation matrix.

ASI-3: Anxiety Sensitivity Index-3; DERS: Difficulties in Emotion Regulation Scale; DASS: Depression Anxiety Stress Scale; MSFI-D: Male Sexual Function Index–Desire Subscale; MSFI-A: Male Sexual Function Index–Arousal Subscale; MSFI-E: Male Sexual Function Index–Erection Subscale; MSFI-O: Male Sexual Function Index–Orgasm Subscale; MSFI-P: Male Sexual Function Index–Pain Subscale; SQoL-M: Sexual Quality of Life Scale–Male Version; SEQ-S: Sexual Experiences Questionnaire–Solitary Items; SEQ-P: Sexual Experiences Questionnaire–Partner Items.
p < .05; **p < .001.

Model 2: Anxiety Sensitivity Directly Predicting Sexual Outcomes, and Psychological Distress Indirectly Predicting Sexual Outcomes. Notes: N = 306. **p < .001; All presented effects are standardized. ASI-3 = Anxiety Sensitivity Index-3; DASS = Depression Anxiety Stress Scales; MSFI-D = Male Sexual Functioning Index, Desire subscale; MSFI-A = Male Sexual Functioning Index, Arousal subscale; MSFI-E = Male Sexual Functioning Index, Erection subscale; MSFI-O = Male Sexual Functioning Index, Orgasm subscale; MSFI-P = Male Sexual Functioning Index, Pain subscale; SQoL-M = Sexual Quality of Life Scale – Male Version; SEQ-P = Sexual Experiences Questionnaire, Partner items; SEQ-S = Sexual Experiences Questionnaire, Solitary items.

Model 3: Emotion Regulation as a Mediator Between Anxiety Sensitivity and Psychological Distress, Which Predict Sexual Outcomes. Notes: N = 306. **p < .001; All presented effects are standardized. ASI-3 = Anxiety Sensitivity Index-3; DASS = Depression Anxiety Stress Scales; DERS = Difficulties in Emotion Regulation Scale; MSFI-D = Male Sexual Functioning Index, Desire subscale; MSFI-A = Male Sexual Functioning Index, Arousal subscale; MSFI-E = Male Sexual Functioning Index, Erection subscale; MSFI-O = Male Sexual Functioning Index, Orgasm subscale; MSFI-P = Male Sexual Functioning Index, Pain subscale; SQoL-M = Sexual Quality of Life Scale – Male Version; SEQ-P = Sexual Experiences Questionnaire, Partner items; SEQ-S = Sexual Experiences Questionnaire, Solitary items.
Model 4: Emotion Regulation as a Moderator Between Anxiety Sensitivity and Psychological Distress, Which Predict Sexual Outcomes. Notes: N = 306. **p < .001; All presented effects are standardized. ASI-3 = Anxiety Sensitivity Index-3; DASS = Depression Anxiety Stress Scales; DERS = Difficulties in Emotion Regulation Scale; MSFI-D = Male Sexual Functioning Index, Desire subscale; MSFI-A = Male Sexual Functioning Index, Arousal subscale; MSFI-E = Male Sexual Functioning Index, Erection subscale; MSFI-O = Male Sexual Functioning Index, Orgasm subscale; MSFI-P = Male Sexual Functioning Index, Pain subscale; SQoL-M = Sexual Quality of Life Scale – Male Version; SEQ-P = Sexual Experiences Questionnaire, Partner items; SEQ-S = Sexual Experiences Questionnaire, Solitary items.
Path analyses
Model 1
Overall, and consistent with the correlations reported in Table 3, men who reported higher AS also reported greater difficulties with sexual desire and sexual arousal, and lower sexual quality of life, but not greater difficulties with erection, orgasm, pain, or frequency of partnered or solitary sexual activity. AS accounted for 2.1 percent of the variance in sexual desire, 2.2 percent of the variance in sexual arousal, and 9.8 percent of the variance in sexual quality of life. 4
Model 2
Overall, men who reported higher AS also reported greater severity of psychological distress. Psychological distress appeared to account for some of the relationship (partially mediated) between AS and sexual quality of life and fully mediated AS’s relationship to sexual arousal. AS continued to directly predict sexual desire. AS accounted for 46.9 percent of the variance in psychological distress. AS and psychological distress together accounted for 2.2 percent of the variance in sexual desire, 4.5 percent of the variance in sexual arousal, 2.3 percent of the variance in orgasm, and 12.9 percent of the variance in sexual quality of life.
Model 3
ER significantly mediated the relationship between AS and psychological distress, and the mediation accounted for 35.9 percent of the variance in psychological distress. AS accounted for 59.9 percent of the variance in ER. All other coefficients were identical to Model 2.
Model 4
The interaction between AS and ER explained a significant increase in psychological distress ΔR2 = .55, F(1, 305) = 186.39, p < .001 (β = .89, p < .001). The moderation accounted for 45.6 percent of the variance in psychological distress. We examined the interaction plot and found that the relationship between AS and psychological distress depended on the level of ER. Specifically, when both AS and ER were high, psychological distress was also high. However, when AS was high and ER was low, psychological distress was much lower. All other coefficients were identical to Model 2.
Discussion
Similarities and differences between men and women’s sexual health
In this study, we sought to explore the role of psychological risk factors on men’s sexual health. We replicated and extended our previous findings with women by testing the same psychological models in a sample of men (Tutino et al., 2017). The results were largely consistent with our previous findings as well as those of Gerrior et al. (2015). Overall, our results suggested that greater AS, more difficulties with emotion regulation, and more symptoms of psychological distress predicted poorer sexual outcomes for men. This indicates that the same risk factors that appear to make people vulnerable to mental health difficulties (i.e. AS, difficulties with emotion regulation) may also contribute to the development of sexual health difficulties.
Consistent with research with women (Gerrior et al., 2015; Tutino et al., 2017), the psychological risk factors were related to some, but not all of the sexual health outcomes. Specifically, of the sexual functioning markers, the psychological risk factors were related to greater difficulties with sexual arousal and orgasm (in both men and women) and desire (in men only). This finding is consistent with research that suggests that sexual arousal may be the most sensitive marker of sexual function in the presence of mental health difficulties (Kennedy et al., 1999). Perhaps this is because sexual arousal is the first phase of physiological sexual response (Masters and Johnson, 1986); disruption in arousal can similarly lead to disruptions in later phases of sexual response such as orgasm. Additionally, the psychological risk factors predicted lower sexual quality of life in both men and women. In contrast to our research with women, we did not find that psychological risk factors predicted the frequency of either partnered or solitary sexual activity.
Our findings suggest that the same psychological risk factors differentially predict markers of sexual health in men compared to women. This may have implications for assessment and treatment of sexual difficulties in men versus women. For example, these findings suggest that mental health difficulties may exert a greater impact on men’s sexual functioning and sexual quality of life than on frequency of sexual activity. In other words, men may engage in sexual activity at the same frequency even if their functioning or satisfaction are impaired. Thus, clinicians may benefit from focusing on functioning and satisfaction during assessment and treatment of men, whereas for women, frequency of sexual activity may be an important target in addition to sexual functioning and satisfaction. On average, women tend to report lower sexual desire and frequency of sexual activity in comparison to men (e.g. Beutel et al., 2008; Jones and Barlow, 1990). This may be related to a higher prevalence of sexual functioning difficulties (Simons and Carey, 2001), as well as greater difficulties with mental health (e.g. depression and anxiety; Angst et al., 2002). Therefore, clinicians should consider additional psychosocial and contextual factors that may be relevant to the individual, in order to improve their overall sexual health.
Emotion regulation as a mediator versus moderator
Another objective of this study was to identify how emotion regulation difficulties contribute to the relationship between AS, psychological distress, and thus, markers of sexual health. We found that the moderational model accounted for more of the variance in psychological distress than did the mediational model. The results of the moderation model suggest that men who have high AS and maladaptive emotion regulation skills may not only be more likely to develop symptoms of anxiety and depression, but they may also be more likely to experience sexual difficulties related to functioning and satisfaction. These findings are similar, but not identical, to the same model comparisons in women. In our sample of women (Tutino et al., 2017), mediational and moderational models appeared to be equivalent in explaining symptoms of psychological distress and then sexual health outcomes. This finding is consistent with research that demonstrated that emotion regulation moderated the relationship between AS and symptoms of anxiety; anxiety symptoms were most severe in people who had both higher AS and elevated difficulties with emotion regulation (Kashdan et al., 2008). More research is needed, particularly longitudinal studies, to improve knowledge on how AS and ER function together in predicting psychological distress, and in turn, sexual health.
The link between mental and sexual health
This is the first study to assess the role of AS in men’s sexual functioning. AS appeared to particularly affect the early stages of the sexual arousal process (i.e. desire and arousal) in our sample of men. In experiencing desire and arousal, men may become attuned to the physiological changes in their body; those high in AS may begin to experience anxiety. If they then regulate their emotions maladaptively in response to this anxiety (e.g. begin to ruminate over their symptoms of sexual arousal), they may experience further decreases in sexual desire or arousal, have difficulties with orgasm, and have a lower sexual quality of life. Thus, although men with high AS may not avoid sexual encounters due to their distressing emotional and physiological experiences, they may experience difficulties in sexual function and interpret their sexual encounters as less pleasurable.
Anxiety during sexual activity may be particularly salient among young men given societal associations between masculinity and sexual performance. Indeed, research suggests that sexuality is one of the greatest predictors of perceived masculinity (De Visser and McDonnell, 2013). It is possible that psychosocial risk factors and particularly the role of AS and ER in sexual difficulties and experiences may differ between sexually active men who identify as heterosexual, gay, bisexual, asexual, or other. Future researchers may benefit from examining similarities and differences across sexual identities.
These findings are consistent with past research that suggests that mental and sexual health may be dependent on one another (Frohlich and Meston, 2002). Moreover, these findings provide a lens from which we can understand how psychosocial risk factors may influence the sexual experiences of young, healthy men.
Research and clinical implications
This study has many strengths both in terms of research contributions and clinical implications. One strength of our study was the use of the Male Sexual Function Index (MSFI; Kalmbach et al., 2012) as a measure of male sexual functioning. The MSFI was developed from the Female Sexual Function Index (FSFI; Rosen et al., 2000) to provide better comparisons between men and women’s sexual difficulties. However, it was missing the sexual pain subscale. We added the pain subscale to the MSFI to improve the comparable interpretations between research with this scale and with the FSFI. In doing so, we contribute new evidence of the factorial validity and internal consistency of this scale, as well as an expanded tool for assessing men’s subjective sexual function, including sexual pain (an often overlooked component).
A second strength was our selection of psychological risk factors that not only play a role in multiple mental health difficulties but are also targets for intervention in a number of established treatment protocols. For example, research on AS consistently has demonstrated its ability to predict anxiety disorders and depressive disorders (Naragon-Gainey, 2010). Difficulties with emotion regulation is a well-established component of borderline personality disorder. Recent research suggests that difficulties with ER (although perhaps less severe than seen in borderline personality disorder) also contribute to the development and maintenance of symptoms of psychological distress (e.g. anxiety, depression; Aldao et al., 2010; Kashdan et al., 2008; Ouimet et al., 2016). There are empirically supported treatments that focus, at least in part, on ER (e.g. Linehan, 1993) and AS (e.g. Smits et al., 2008) Thus, more research on the role these psychological risk factors play in sexual health likely will provide fruitful information for improving clinical practice and theoretical models of sexual health.
Clinically, our findings suggest that the bigger picture of men’s sexual health—one that comes from a psychosocial perspective that includes psychological risk factors, mental health, and multiple sexual indicators—likely will improve clinicians’ assessments and interventions. Mental health professionals would benefit from assessing general psychological risk factors such as AS and emotion regulation when treating both mental and sexual health difficulties, whether these occur together or separately. Consistent with previous research calling for greater sexuality-specific training for clinical psychologists (Miller and Byers, 2012; Reissing and Giulio, 2010), our findings suggest that mental health professionals need to be aware of, and learn to address, the potential impact that men’s psychological distress has on their sexual health—even if it is not related to whether or not they engage in sexual activities. Thus, mental health practitioners would benefit from ensuring they assess global health indicators during psychological or sexological assessments and use all the information acquired to develop a treatment program that targets not only symptoms or difficulties but also the underlying factors that place people at risk for developing problems in the first place.
Limitations and conclusion
Although this study has many strengths, there are limitations that must be addressed. It included a large sample of men of diverse sexual orientations. However, the findings are limited in their generalizability to men who are primarily White, Canadian, and highly educated. Given that we did not assess clinical diagnoses in our sample, the role of psychological risk factors may occur differently in people presenting for treatment of mental and/or sexual health difficulties. Therefore, future researchers would benefit from replicating this study with a more diverse sample, and a clinical sample, to investigate whether the models replicate. Future researchers may also wish to extend the current findings using mixed-gender samples and comparing the different subscales of the ASI-3 within one statistical model framework.
In testing several predictive models of sexual health, this study has contributed to the literature on men’s sexual health by providing initial information on how psychological risk factors interact with one another to predict sexual health difficulties. Our findings point to many similarities and some differences in the role of psychological risk factors for men’s and women’s sexual health. Overall, the findings point to the importance of including multiple indicators of men’s sexual health in research and in clinical practice. Indeed, psychological risk factors likely are more relevant to men’s sexual health than is currently understood.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.