
Abstract
For many people, the influence of believing in a higher power can elicit powerful effects. This study examined the relationship between God control, health locus of control, and frequency of religious attendance within 838 college students through online surveys. Regression analysis showed that chance and external locus of control and frequency of religious attendance were significant and positive predictors of God Locus of Health Control. The association of powerful others external locus of control and God Locus of Health Control differed by race (stronger in non-Whites than Whites) and somewhat by gender (stronger in women than men). For some people, the role of a supreme being, or God, should be considered when designing programs for improving health behaviors.
Introduction
For decades, researchers have investigated the role of locus of control (LOC) in an attempt to understand the many psychological processes underlying behaviors. In short, LOC is a theory that explains the extent to which individuals believe they can control life events (Ai et al., 2005). The LOC construct was proposed by Rotter (1954) and is considered a result of experiences that provide future expectations about behaviors. The source or motivation of LOC is either external (ELOC; e.g. other people or things) or internal (ILOC; e.g. perseverance and self-efficacy).
Health LOC refers to how much control individuals believe they have over the health events that happen in their lives. Health LOC is often studied in relation to health behaviors, and most research is based on the use of Multidimensional Health Locus of Control (MHLC) scale developed by Wallston et al. (1978), which scores an individual on ILOC and two types of ELOC—chance and powerful others. There is evidence that individuals with a higher ILOC have more desirable health behaviors and outcomes than those with a higher ELOC. For example, greater ILOC has shown to be predictive of lower rates of excessive drinking (Kuwahara et al., 2004) and smoking (Wallston et al., 1978) and has been associated with better nutritional behavior (Chen et al., 2010). Weinstein et al. (2002) found that a higher ILOC was associated with less heart and circulatory system distress. In another study, women with high ILOC had a greater belief that they could control whether or not they developed breast cancer than those with lower ILOC scores (Rowe et al., 2005).
There is also evidence that suggests higher ELOC is associated with less desirable health behaviors and outcomes. Abouserie (1994) and Gadzella (1994) found that college students with higher ELOC were more likely to report higher levels of stress than those with higher ILOC. Additionally, higher ELOC was associated with lower quality of life scores in individuals with chronic back pain (Sengul et al., 2010). Those with ELOC may be less likely to engage in preventive behaviors and more likely to experience negative health outcomes.
God as a source of control
Researchers have examined the role of religion as a source of control-related cognitions, especially within religious and spiritual populations. Gabbard et al. (1986) interpret God control as being similar to an ELOC source, but other researchers note that a belief in God is distinct from other external sources (Furnham, 1982; Jackson and Coursey, 1988; Pargament et al., 1982). The latter argue that the presence of God in one’s life might produce more internal control, such as self-efficacy, motivation, and determination. Studies on faith and LOC performed in the 1970s showed that those reporting higher levels of faith also reported higher levels of internal control (Benson and Spilka, 1973; Shrauger and Silverman, 1971). Later studies found no association (Alton, 1999; Wong-McDonald and Gorsuch, 2000), and one study found a negative association between internal control and religiosity (Shaw and Krause, 2001).
Welton et al. (1996) created one of the first LOC scales that specifically measured the presence of God as it related to control. The authors proposed “God-Control” as a fourth dimension, one that is beyond the original health LOC sources of internal, external (powerful others), or external (chance). Welton and colleagues surveyed two separate samples of college students, one from a major Midwestern State University, and another from a small Midwestern Christian liberal arts school. Within the university sample, a small negative correlation between ILOC and God Control was found. Interestingly, however, God Control was not significantly related to ELOC sources of powerful others or chance. Within the Christian school sample, correlations showed that the more favorable health habits scores were related to high ILOC scores, high God Control scores, and low powerful others LOC scores. This research demonstrated the complex interaction of religion and source of control, and that God-control may not be synonymous with ELOC source for all populations.
Wallston et al. (1999) developed the God Locus of Health Control (GLHC) scale as an extension of the original MHLC scale, specifically designed to measure the extent that individuals feel God controls health and health-related events. Wallston et al. (1999) surveyed a sample of individuals with rheumatoid arthritis and a sample of individuals with systemic sclerosis. They found that the GLHC was significantly and positively correlated with external sources from the MHLC. Internality was unrelated to GLHC in both samples. The authors then created a more general health form of the GLHC that could be used within healthy populations (wording replaced “condition” with “health”.
In 2001, researchers examined the correlations of the sources of LOC (Internal, God, Powerful Others, and Chance) in a large and diverse sample of women (Chaplin, Davidson, Sparrow, Stuhr, Van Roomsmalen, and Wallston). There were strong positive correlations between the God, Chance, and Powerful Others LOC subscales; however, positive associations were also found between the God and ILOC subscale, although the magnitude was not as strong. Other authors have found a significant positive correlation between an awareness of God and ILOC, as well as a positive correlation between God LOC and ILOC (Ryan and Francis, 2012), although a different and less utilized LOC scale was used. These authors argue that individuals with a greater belief in God believe that God will protect and guide them, which leads to more optimism and confidence from the individuals, endorsing higher ILOC.
Within the LOC literature, studies that have measured the element of God control have inconsistent findings. Therefore, practitioners and educators must question the generalizations of the LOC research to the more spiritual and religious populations. It is important to continue the research on how God is perceived as a source of control, especially for design and implementation of health behavior programs that may include religious and spiritual individuals or programs conducted in faith-based settings. Therefore, the purpose of this study was to determine whether a belief or faith in God is more highly associated with an internal or external source of control for health. Specifically, this study examined the relationship between GLHC and subscales of the MHLC and frequency of religious attendance within a college student population, and whether these relationships differed by gender or race.
Methods
Procedure
This study used Internet-based surveys from a volunteer sample of college students in two southeastern universities in the United States, conducted between July 2013 and September 2013. The surveys used in this article consisted of 3 different scales, with 32 total items. The study was approved by each university’s institutional review board, and participants were given a written statement at the beginning of the surveys and directed to complete the survey if they consented to be in the study.
Participants
Participants were recruited for this study via the following methods: student listserv emails, flyers, and announcements in classes and organizations. Willing participants completed the survey through a link in these emails, flyers, and handouts. The sample used for any analysis included 838 students (see Table 1). The majority of the sample was female (n = 614; 73.4%), and White (n = 543; 64.1%) or Black/African American (n = 195; 23.0%).
Sample characteristics.
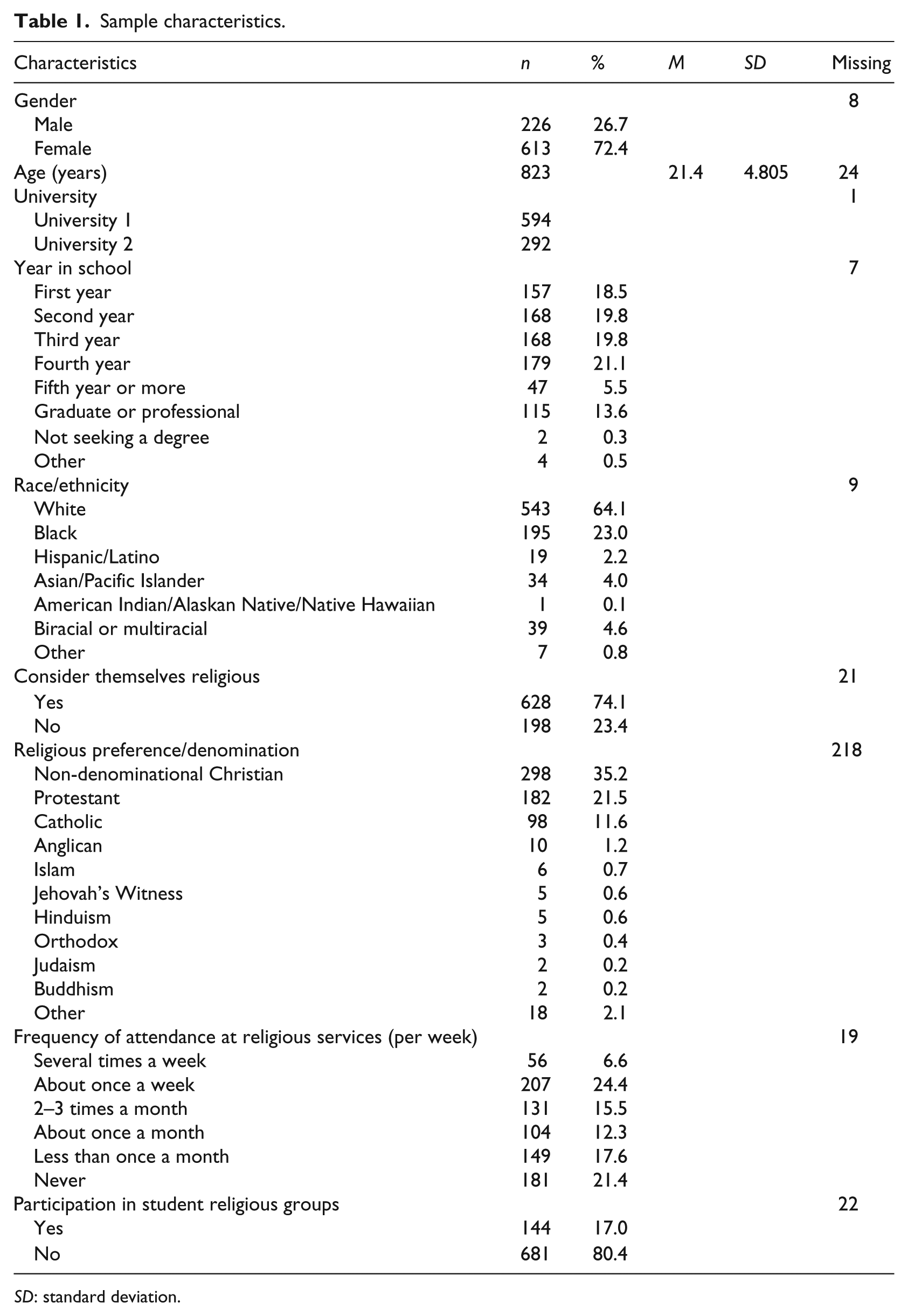
SD: standard deviation.
Instrumentation
All assessments for this study were conducted through an online survey tool, Survey Monkey (2013). Demographic information was assessed with questions from the 2012 American College Health Association (ACHA)—National College Health Assessment (NCHA) II: age, gender, height and weight, year in school, enrollment status, race/ethnicity, marital status, and on/off campus residence.
Health LOC was measured with the 18-item MHLC scale (Wallston et al., 1978). For this study, MHLC Form B was administered. Examples of MHLC items are as follows: “I am directly responsible for my health” and “Health professionals keep me healthy.” Items within each subscale showed moderately high internal consistencies for internal health locus of control (ILOC; α = .70), external health locus of control-chance (chance ELOC; α = .64), and external health locus of control-powerful others (powerful others ELOC; α = .69). Items for each subscale were summed for a total subscale score, and scores ranged from 6 to 36 for each subscale, with higher scores demonstrating higher health LOC for that subscale. Similar reliability of the MHLC has been reported as α = .64–.78, as well as strong concurrent, construct, and discriminant validity (Furnham and Steele, 1993 ).
GLHC was assessed through a six-item scale to measure the influence individuals believe that God has over their health and included statements such as “Whatever happens to my health is God’s will” (Wallston et al., 1999). Responses for items were answered on a six-point Likert scale, ranging from strongly disagree (1) to strongly agree (6). Total scores were summed and ranged from 6 to 36, with higher score representing a greater belief in God as a LOC. Internal consistency for the GLHC was high in this study (α = .96), which is comparable to a previous study that also showed acceptable convergent validity and high alpha reliability (Wallston et al., 1999). The use of GLHC and MHLC scales was part of a larger data collection. Participants were asked to provide consent before answering religious questions, and therefore, all religious-based questions were grouped together. For that reason, the GLHC was not interspersed within the MHLC scale. Table 2 describes the sample values for the variables of interest.
Sample values on independent, dependent, and mediating variables.

GLHC: God Locus of Health Control; MHLC: multidimensional health locus of control.
Statistical analysis
Statistical Packages for the Social Sciences (SPSS) was used for all statistical analyses. Initial analyses were conducted to describe the variables and to examine the normality of distributions (IBM Corp., 2012).
First, correlations were performed to determine the relationships between GLHC and ILOC, chance ELOC, powerful others ELOC, and frequency of religious participation. Using Cohen’s guidelines, we considered a small effect size as r = .10, a medium effect size as .30, and a large effect size as .50 (Cohen, 1988). Second, regression analyses were performed in order to predict dependent variable Y (GLHC) from the independent variables X (ILOC, chance ELOC, powerful others ELOC, and frequency of religious participation), controlling for age, gender, and race. A second regression model included additional covariates of school attended and involvement in campus religious groups. Interactions of gender and race also examined whether the associations between the independent variables (ILOC, chance ELOC, powerful others ELOC, and frequency of religious attendance) and the dependent variable (GLHC) differed by gender and by race. Within this model, if the interaction p-value > .10, that interaction was removed and the model was re-run, and the results were presented.
Results
Of the 1055 people who began the survey, 208 were excluded. Seventeen individuals were under the age of 18 years, 11 were not attending one of the two universities targeted in the study, and 181 had a high amount of missing data (>20% of responses).
Bivariate correlations showed a significant positive relationship between GLHC and both chance ELOC (p < .001) and powerful others ELOC (p < .001). Additionally, correlations showed a significant negative relationship between GLHC and ILOC (p = .003). GLHC was also significantly and positively associated with frequency of religious attendance (p < .001). Table 3 shows the correlations of GLHC, subscales of the MHLC, frequency of religious attendance, and covariates.
Correlation matrix for scales used in study.
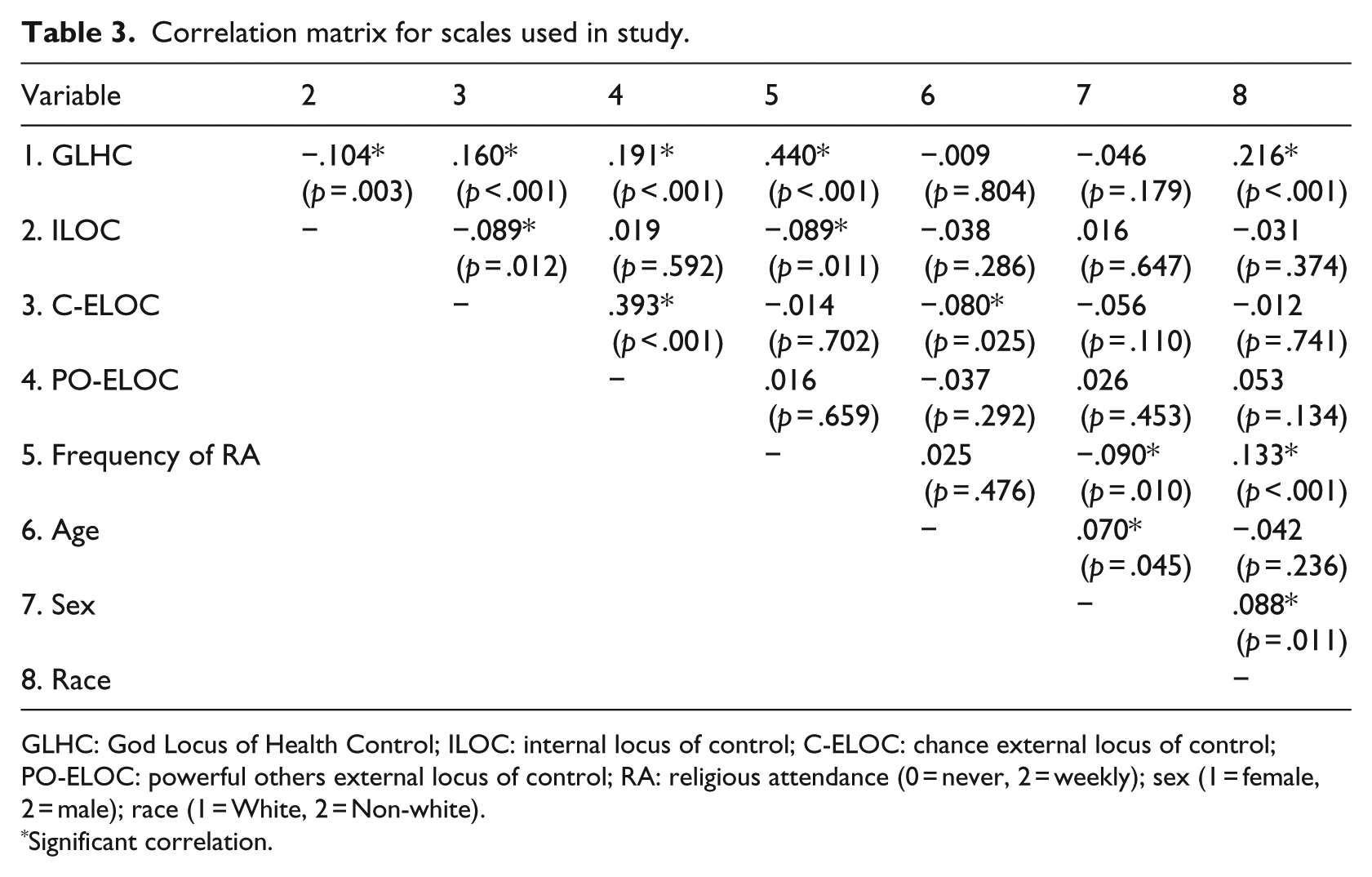
GLHC: God Locus of Health Control; ILOC: internal locus of control; C-ELOC: chance external locus of control; PO-ELOC: powerful others external locus of control; RA: religious attendance (0 = never, 2 = weekly); sex (1 = female, 2 = male); race (1 = White, 2 = Non-white).
Significant correlation.
Regression analysis showed that ILOC was not a significant predictor of GLHC (p = .239). ELOC subscales of chance and powerful others were both significant and positive predictors of GLHC (p = .004; p < .001). Those with higher ELOC scores were more likely to have a higher GLHC score, controlling for age, race, and gender. Frequency of religious attendance was also a significant and positive predictor of GLHC (p < .001), as those who attended religious services more often had higher scores of GLHC scores, controlling for age, race, and gender.
When the covariates of school attended and participation in campus religious groups and interactions (of at least p ≤ .10) were added, chance ELOC (p = .014) and frequency of religious attendance (p < .001) remained significant. ILOC (p = .388) was not significant. The interaction of powerful others ELOC and gender was significant (p = .043); the association was stronger in women (r = .222, p < .001) than in men (r = .106, p = .120). Finally, the interaction of powerful others ELOC and race was borderline significant (p = .057); the association was somewhat stronger in non-Whites (r = .194, p = .001) than in Whites (r = .180, p < .001). Table 4 shows the regression coefficients and effect sizes for the adjusted regression model.
Regression coefficients for the adjusted regression model.

Dependent variable: TotalGLHC.
Discussion
The purpose of this study was to better understand how an individual’s source of control for health relates to an individual’s reliance on God for health-related events. Specifically, we examined the relationship between GLHC, MHLC, and frequency of attendance at religious services within a college student population. We found a significant positive relationship between GLHC and chance ELOC, powerful others ELOC, and frequency of religious attendance, when controlling for age, gender, and race. The relationship of powerful others ELOC and GLHC differed by race and by gender.
These findings are consistent with previous literature that found similar correlations between a belief in God and external sources of control (Gabbard et al., 1986; Wallston et al., 1999). However, these findings are in contradiction with other studies that have found no relationship between GLHC and ELOC sources (Welton et al., 1996), and those that found significant positive relationship between God Control and ILOC (Chaplin et al., 2001; Ryan and Francis, 2012; Welton et al., 1996).
Research suggests that health LOC beliefs predict health behaviors. Specifically, those with higher ILOC tend to practice greater preventive health behaviors than those with higher ELOC, but the generalization is not clear for all populations, especially for those that are religious or spiritual. It seems plausible that religion and a belief in God or a Supreme Being would be a source of control-related cognitions. The concern with generalizations of LOC beliefs is the lack of attention focused to the religious and spiritual populations, and a lack of understanding as to the specific impact that God or Supreme Being would impose on health-related beliefs and behaviors.
Some researchers agree that God control is an ELOC (Gabbard et al., 1986), but others disagree (Furnham, 1982; Jackson and Coursey, 1988; Pargament et al., 1982). However, the presence of God in one’s life might have powerful internal effects, such as an increase in self-efficacy and perseverance. Welton et al. (1996) referred to “God-control” as a fourth dimension, one that is beyond the original three health LOC sources of internal, chance, or powerful others. In fact, even though we found significant associations between GLHC and external sources of control, the correlations were small in magnitude, indicating that while there is overlap in constructs, they are not synonymous. Therefore, we support the idea that “God-control” may not be totally internal or totally external as it relates to an LOC source. A belief in God may actually be a fourth dimension, as suggested by Welton et al. (1996).
We also found that a belief in God may affect different people in different ways, as suggested by Ai et al. (2005). Ai et al. note that conflicting evidence points to a very complex relationship between faith and LOC, one that can be judged both positively and negatively for health behaviors for different people. Our findings support this, as the relationship of powerful others ELOC and GLHC was stronger in non-Whites than Whites and somewhat stronger in women than men. While the interpretation of these differences could be subjective, it is possible that these segments of the population experience a greater reliance of God as an external influence on health in their lives. This could relate to the concept of fatalism. Fatalism is the belief that an individual’s health outcome is predetermined or purposed by a higher power and not within the individual’s control. To be specific, it is important to understand how the psychological LOC factors intertwine with religious beliefs as they relate to fatalism. How do these beliefs impact segments of the population, when not all of the religious population show the same beliefs? Previous research has indicated that fatalism and religiosity may have significantly different effects across diverse groups when viewed together rather than separately (Fiori et al., 2006; Neff and Hoppe, 1993). These different effects may be due to differences in LOC beliefs, and account for the differences in race and gender that we found within our study, but additional research within the segments of the religious population is necessary.
Greater frequency of attendance at religious services has been linked to beneficial health behaviors and a lower risk of mortality (Gillum et al., 2008). Our findings support that individuals with greater frequency of religious attendance also had greater belief that God was in control of their health. Previous research has indicated that some segments of the population have a greater religious involvement than others, specifically in African Americans and women (Levin et al., 1994; Taylor et al., 1996); however, we did not find any differences in the effect of frequency of religious attendance and belief in God control between race and gender. Since this research was conducted in the southeastern United States, it is possible that results would be different in other geographical locations.
Limitations and strengths
It is important to address the limitations of this research. A large number of participants were removed because of a high amount of missing data (17% of those who initiated the survey). Since the study was online, there was a chance that some individuals were unable to complete the survey due to technical issues. Additionally, participants with a large amount of missing data often answered the first few surveys, but ended their responses before completing all items. Responses may have also been influenced by the setting and environment as the surveys were completed online. This research also had a much higher percentage of women (72.9%) than men which could limit generalization to men. The use of a cross-sectional design limits the ability of this research to infer causation. It is worth noting that the effect sizes of the calculations were small, and therefore, differences may be considered of little practical significance.
There are several notable strengths of this study. First, this study focused on a poorly understood topic within the LOC literature. Specifically, the association of God as a source of control, either internal or external, is a topic that has received very little attention with conflicting findings. Other strengths include the large sample size and race/ethnic diversity of participants. The sample was majority Caucasian (65%), but representation among the sample within the Black/African American population was strong (22%), and was representative of the student body populations at each university. Undergraduate (all classes) and graduate students were equally represented within the entire sample studied.
Conclusion
In this study, ELOC was significantly and positively associated with GLHC, although the magnitude of the correlation was small. The association of powerful others ELOC and GLHC differed by race and somewhat differed by gender. To understand completely the impact of LOC on health behaviors, it is crucial to consider the element of God control, and to not limit the discussion to only internal, powerful others, and chance sources of control. Although relationships were significant, small effect sizes can limit the definitiveness of God control being an external source. More research is needed to better understand these relationships, especially as they relate to population segments.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.