
Abstract
This study examined associations of pre-frailty and frailty states with cognitive and functional health outcomes among community-residing older adults (N = 457) in the Bronx, New York. Results: older adults who met criteria for frailty demonstrated poorer performance in attention, verbal memory, and overall global cognitive functioning compared to healthy controls. Moreover, pre-frail and frail older adults had significantly worse health outcomes including greater perceived difficulty with lower and upper extremity functioning and perceived limitations in completing daily activities, suggesting the need for targeted interventions in the community that may ameliorate age-related health decline.
Introduction
Fried’s phenotypic frailty is well established in the literature and commonly highlighted as an adverse health condition in the aging population characterized by decreased resistance to stressors and reduced physiological function. Pre-frailty is characterized as a modifiable intermediate state of physical frailty (Fried et al., 2001). However, not all pre-frail older adults deteriorate into frailty, and some may even return to a non-frail state, making it a meaningful and complex measure of physical health in the aging population (Macuco et al., 2012).
As seen in the Cardiovascular Health Study, the prevalence of frail older adults was merely 6.3 percent, whereas 45.3 percent were pre-frail. Furthermore, previous studies have estimated that in Western societies, 18.8–50.9 percent of community-dwelling older adults are pre-frail (Ng et al., 2015). Although it is relevant to develop a comprehensive understanding of frail older adults, the majority of older adults are not frail. It is essential for research to address this gap in the literature characterizing the cognitive and health profiles associated with older adults who are both pre-frail and frail.
Recent literature has highlighted the importance of determining associations between frailty status and functional health outcomes in the aging population (Yang and Pang, 2018). Individuals who meet diagnostic criteria for frailty require the most geriatric care among the rapidly growing baby boom population in the United States (Kim et al., 2014; Yang and Pang, 2018). In relation to health, it has been demonstrated that frail older adults are at a greater risk of adverse health outcomes (Macuco et al., 2012). Moreover, older adults exhibiting both poor cognitive performance and physical frailty are at a greater risk of poor health outcomes, like disability, hospitalization, and death, than if just exhibiting physical frailty (Alexandre et al., 2014; Ávila-Funes et al., 2009; Het Veld et al., 2015; Kelaiditi et al., 2013). Therefore, distinguishing the adverse health outcomes associated with not just frailty, but the transitional state of pre-frailty, is important for developing and targeting preventative health-care efforts for this at-risk population (Lang et al., 2009). This study aimed to bridge the gap in the literature by examining associations between both pre-frailty and frailty states and targeted health outcomes, including both physical and cognitive functioning.
Previous research revealed that frailty was associated with lower global cognitive functioning among non-demented, older adults (Robertson et al., 2013). However, to our knowledge, the majority of the studies examining associations of frailty and pre-frailty with cognition have largely employed screen or global measures of cognitive function, like the Mini Mental Status Examination (MMSE). In comparison, research addressing specific cognitive domains is more limited (Robertson et al., 2013). With respect to physical health, research showed that frail older adults were at a greater risk of adverse functional outcomes that may negatively affect activities of daily living. However, the majority of frailty studies have focused on differences in health outcomes between frail and non-frail individuals excluding those who met criteria for pre-frailty status.
This study aimed to address these gaps in the literature by determining the relationship between both pre-frailty and frailty states with specific cognitive and functional health outcomes in community-residing, non-demented older adults. Identifying adverse functional and cognitive health outcomes that are differentially related to frailty and pre-frailty states is important for informing early assessment procedures and interventions for at-risk older adults (Macuco et al., 2012).
Methods
Participants
The study sample (N = 457) consisted of community-residing older adults recruited for an existing longitudinal parent study titled, “Central Control of Mobility and Aging.” Goals of this study are to determine cognitive and brain predictors of mobility performance, decline, and disability in aging. Recruitment procedures: population lists of persons aged 65 years and older living in Westchester County were used to identify potential participants who were contacted first by letter and then by telephone inviting them to participate. The structured telephone interview included verbal consent, medical history questionnaire, mobility questions, and validated cognitive screens designed to exclude dementia (Holtzer et al., 2014). Exclusion criteria included audiovisual loss that precluded compliance with study procedures, inability to speak English, inability to ambulate independently, neurological or psychiatric disorders, and dementia (Holtzer et al., 2014). Established diagnostic case conference procedures were used to determine dementia status (Holtzer et al., 2008b), and only non-demented participants were included in this study. Case conference procedures entail attendance by at least one neuropsychologist and one neurologist who review the participants’ cognitive, medical, and functional data. Dementia is diagnosed according to Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-V) criteria. Written informed consents, approved by The Albert Einstein College of Medicine Institutional Review Board, were obtained onsite.
Measures
Frailty assessment followed criteria established by Fried’s phenotype. Frailty was measured utilizing a binary scale that represented either the presence (e.g. 1) or absence (e.g. 0) of each of the five frailty traits for an individual (e.g. weight loss, low physical activity, weakness, exhaustion, slow gait). Weight loss was defined a loss of ≥10 lbs over the previous year. Low physical activity was defined by an endorsement of “Yes” to “Have you been less physically active in the past 12 months?” on a leisure scale. Weakness was defined as the average of three trials using a handgrip dynamometer. Established cut scores were adjusted for sex based on published normative data (Cho et al., 2015). Exhaustion was defined as an answer of “No,” for, “Do you feel full of energy?” on both the Geriatric Depression Scale (GDS) (Yesavage et al., 1983) and a self-report Mobility Questionnaire. Slow gait was defined as walking speed 1 SD below age- and sex-specific means based on the CCMA cohort as previously reported (Chen et al., 2017). GAITRite software was used to calculate individual gait velocity through computer-analyzed recordings of footfalls on an instrumented walkway with embedded pressure sensors measuring 6.1 m × .6 m (L × W).
All neuropsychological tests used for this study have been well validated for older adults in the previous literature (Demetriou and Holtzer, 2017). The Repeatable Battery for the Assessment of Neuropsychological Status (RBANS) is a battery for older adults that consists of 10 neurocognitive tests and was used to assess immediate and delayed memory, attention, language, and visuospatial abilities. An overall cognitive score represented a composite of the 10 RBANS tests. Raw scores were calculated by trained Research Assistants and then converted to standardize scores based on age and education. The digit symbol substitution test (DSST) was used as an assessment of complex attention from the Wechsler Adult Intelligence Scale. Participants were instructed to write down the corresponding symbol to a digit, as quickly as possible, in consecutive order, without making mistakes. The number of correctly matched digit–symbol pairs is measured after 90 seconds. The correct number of symbols completed was converted to standardized scores based on age and education. The Controlled Oral Word Association Test–Semantic and Phonemic Fluency (COWAT-FAS) was used to assess verbal fluency. In phonemic fluency, participants were instructed to verbally generate as many words in 1 minute for each of the letters F, A, and S. In semantic fluency, participants were required to verbally generate as many animal names in 1 minute (Holtzer et al., 2008a). The correct number of words was converted to standardized scores based on age and education.
The Late-Life Function and Disability Instrument—functional (LLFDI-F) and disability (LLFDI-D) components are validated measures in the older adult population that assess perceived basic lower, advanced lower extremity function, and upper extremity function of older adults (Sayers et al., 2004). For example, participants are asked to assess how difficult it is to, “walk around one floor of your home” or “unscrew the lid off a previously unopened jar, without using assistive devices.” The function and disability components are measured using a rating scale from 1 to 5, where the lower number corresponds to worse functioning. Raw summary scores were calculated and transformed to scaled scores. The LLFDI-D asks participants to report two parts of a question: how often you do an activity and to what extent do you feel limited in doing that activity? For example, participants are asked, “How often do you take care of local errands like managing and taking responsibility for shopping for food or personal items, going to the bank, library or dry cleaner?” and “To what extent do you feel limited in doing that activity?”
Statistical analysis
Data were inspected descriptively and visually. Separate linear regression analyses determined the relationships between group status and cognitive and functional outcomes. Analyses controlled for age, education, gender, global health/comorbidity score, and ethnicity. All statistical analyses were performed using SPSS version 21 (IBM, Somers, NY, USA).
Results
A total of 457 older adults (57.1% female; 79.9% Caucasian) completed measurements for baseline frailty, cognitive, and functional health outcomes. Mean age was 76.50 (±6.55) years, and mean education level was 14.5 (±3.08) years. The mean RBANS standardized total score (91.4 ± 12.04) was in the average range of cognitive function. The low disease comorbidity summary (1.64, ±1.08) indicated relatively good health. Descriptive data of demographic, cognitive, and functional variables stratified by group (non-frail, pre-frail, frail) are provided in Supplemental Table 1.
In total, 171 subjects (37.4%) were non-frail, 258 (56.5%) were pre-frail, and 28 (6.13%) were frail. For pre-frailty, 132 (51.2%) had low physical activity, 70 (27.1%) had low grip strength (weakness), and 59 (22.9%) had slow gait. For frailty, 24 (85.7%) had low physical activity, 24 (85.7%) had slow gait, and 6 (78.6%) had low grip strength.
Linear regressions compared the effect of group status on immediate and delayed verbal memory, executive functions/attention, and premorbid functioning (see Table 1). There were statistically significant differences between the non-frail and frail groups on list recall (p < .05), overall cognition (p < .001), and on executive functions and attention (p < .001). Differences between the non-frail and pre-frail groups were not significant on any of the neuropsychological tests (see Table 1).
Linear regression analyses: associations of cognitive domains, functional status, and frailty status.
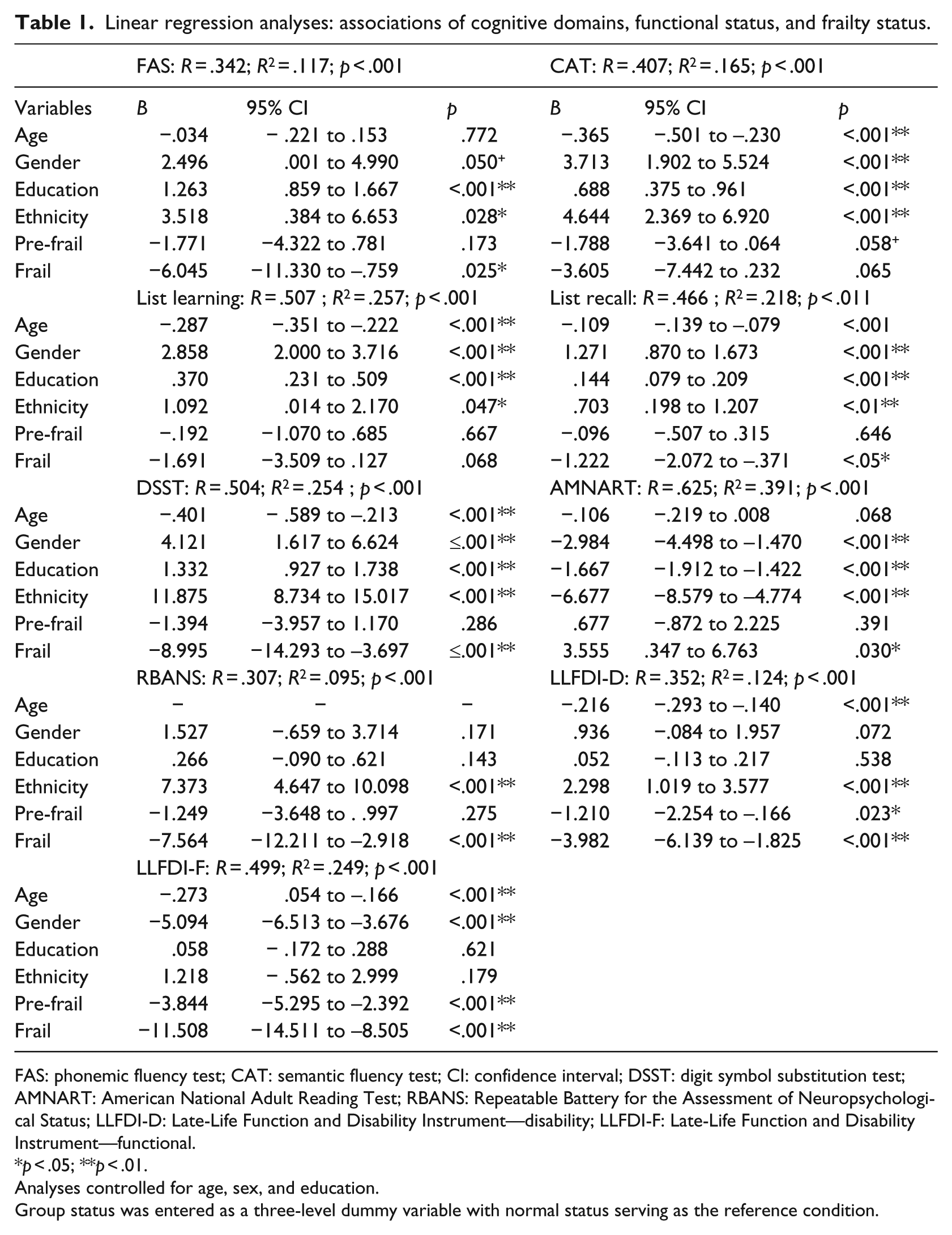
FAS: phonemic fluency test; CAT: semantic fluency test; CI: confidence interval; DSST: digit symbol substitution test; AMNART: American National Adult Reading Test; RBANS: Repeatable Battery for the Assessment of Neuropsychological Status; LLFDI-D: Late-Life Function and Disability Instrument—disability; LLFDI-F: Late-Life Function and Disability Instrument—functional.
p < .05; **p < .01.
Analyses controlled for age, sex, and education.
Group status was entered as a three-level dummy variable with normal status serving as the reference condition.
Multiple linear regression analyses revealed that worse late-life functional health, operationalized as perceived difficulty with advanced lower and upper extremity function, was significantly associated with pre-frailty (p < .001) and frailty (p < .001) as compared to the non-frail group. Similarly, worse late-life disability, operationalized as perceived physical limitations in doing every day activities, was significantly associated with pre-frail (p = .023) and frail groups (p < .001) as compared to healthy controls.
Discussion
This study determined associations between pre-frailty and frailty status with cognitive and functional health outcomes in a community sample of non-demented, older adults. Consistent with previous research examining the relationship between frailty and global cognitive functioning (Faria et al., 2013; Macuco et al., 2012), the presence of frailty was associated with worse overall cognitive function. In line with the study’s goal of further elucidating what specific cognitive domains are associated with frailty, we found that frail participants performed worse on measures of executive functions/attention, verbal memory, and premorbid ability in comparison to non-frail individuals. This finding is interesting in that it suggests the cognitive frailty model that is steadily gaining focus in the literature (Ruan et al., 2015) could be further refined because not all cognitive domains may be simultaneously impaired in all stages of physical frailty. This finding further contributes to the existing literature aiming to explore the association of frailty and pre-frailty with other cognitive domains beyond a global cognitive score. It is noteworthy that pre-frailty status was not associated with significantly worse cognitive functions in this study. Future research should focus on longitudinal studies to identify relationships between frailty and cognitive measures that may characterize and distinguish cognitive profiles between non-frail and pre-frail older adults in more diverse populations.
Findings of our study also highlighted the importance of focusing on the relationship between pre-frailty, frailty, and perceived physical functioning. We found that along with frail older adults, pre-frail older adults were performing significantly worse on functional and disability health outcomes. Targeting older adults in the transitional state of pre-frailty in geriatric medical practices may prevent further disability and cognitive impairment. Overall, our study reinforces the need to tailor risk assessment and interventions at a physical level for pre-frail older adults and at both physical and cognitive levels for frail older adults given their vulnerability to reduced physiological reserves and increased stress.
Several studies have begun to address frailty as a potentially modifiable risk factor for dementia by tailoring interventions to improve frailty status in institutionalized older adults. However, the recent literature suggests that although these interventions have been successful at increasing physical functioning and quality of life in frail older adults, there is a paucity of research examining possible interventions in pre-frail, community-dwelling older adults (Abizanda et al., 2014; Langlois et al., 2013).
Given that low physical activity and weak grip strength were the two most endorsed frail traits in our pre-frail population, increasing physical activity including cardio and strength training may be a suitable intervention. Some literature suggest combinations of physical and cognitive interventions may improve frailty status (Langlois et al., 2013; Ng et al., 2015).
The strength of this investigation lies in its comprehensive battery of cognitive tests, functional outcomes, and objective assessments of multiple study measures. A limitation is its cross-sectional design, which limits interpretations of causality. However, the associations of pre-frailty and frailty with the study outcomes are important for understanding the unique challenges each stage of frailty presents. Future research may benefit from examining subjective cognitive decline in association with pre-frailty (Ng et al., 2015; Ruan et al., 2015). The findings of this study should also be replicated in more ethnically diverse samples of older adults to determine generalizability to other populations. Finally, there is no consensus on the theoretical definition of frailty. However, phenotypic frailty is most commonly used in research settings and has shown to predict adverse health outcomes for older adults (Abizanda et al., 2014). Furthermore, assessment of phenotypic frailty may be difficult to replicate in all clinical settings and alternate methods at targeting frailty status, and risk should be considered in diverse health settings.
In conclusion, our study increases awareness of the vital need to identify and gain in-depth understanding of targeted health outcomes, such as specific domains of cognitive and functional health profiles of pre-frail and frail community-dwelling, non-demented older adults. Given the dynamic nature of the frailty syndrome, pre-frail and frail older adults targeted for treatment have a greater chance of reversing the syndrome and preventing adverse outcomes. Further research identifying factors that may influence the development of pre-frailty and frailty in older adults, such as perceived social support throughout the lifespan, may further elucidate the trajectories of this phenotype (Luger et al., 2016).
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research was supported by funding from the National Institute on Aging (R01AG036921-01A1 and R01AG044007-01A1) and the Resnick Gerontology Center at the Albert Einstein College of Medicine. The sponsors had no role in the design and conduct of the study; in the collection, analysis, and interpretation of data; in the preparation of the manuscript; or in the review or approval of the manuscript.
Supplemental material
Supplemental material is available for this article online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.