
Abstract
The total and indirect effect of hostility on systolic and diastolic blood pressure was compared as a function of religious and spirituality identity in a nationally representative sample of 2971 adults aged 46.44 years. Structural equation modeling uncovered an indirect path from hostility to diastolic blood pressure via unhealthy behaviors and hostility to unhealthy behaviors via social isolation. Compared to a non-religious/non-spiritual reference group, the effect for unhealthy behaviors on diastolic blood pressure was greater for those endorsing some form of religious identity. However, the direction of the effect for hostility on social isolation and social isolation on unhealthy behaviors was reversed in those endorsing spiritual and religious identity.
Introduction
Elevated blood pressure and essential hypertension (HTN) are associated with increased risk for cardiovascular disease (CVD) mortality (Chobanian et al., 2003; Collaboration, 2002). In the US, sedentary behavior, unhealthy diet, and excessive consumption of alcohol and tobacco are amongst the top modifiable lifestyle factors that contribute to HTN and CVD (Forman et al., 2009; Geleijnse et al., 2004; He et al., 2002). It is widely observed that cynical thoughts that manifest in hostility and paranoid alienation towards others results in a predilection toward HTN and CVD (Schum et al., 2003; Sharma, 2016; Suls, 2013). Indeed, hostile individuals are more likely to smoke, engage in moderate to heavy drinking, and report less physical activity than their low-hostile counterparts, suggesting both direct and indirect paths for hostility-related CVD risk (Calhoun et al., 2001; Cougle et al., 2014; Kahler et al., 2004; Whiteman et al., 1997). In addition to these behavioral factors contemporary models suggest interpersonal consequence of hostility, i.e., interpersonal conflict and diminished social support, may also increase risk for HTN and heart disease (Kaplan and Nunes, 2003; Levenstein et al., 2001; Smith et al., 2004). This predilection toward interpersonal conflict and erosion of social support may also contribute to CVD risk via higher self-reported loneliness (Abolfathi Momtaz et al., 2011; Benotsch et al., 1997; Cacioppo et al., 2015; Gallo and Smith, 1999; Guyll and Contrada, 1998; Steptoe et al., 2004; Uchino, 2006). Those perceiving greater loneliness and lower social support show elevations in arterial blood pressure and risk for HTN (Cacioppo and Hawkley, 2003; Uchino et al., 1996), particularly with advancing age (Hawkley et al., 2006, 2010; Momtaz et al., 2012).
Religion, spirituality, and CVD
In recent years, interest has grown in the mitigating role of religious and spiritual (R/S) identity on biopsychosocial risk for CVD (Ginting et al., 2015; Lucchese and Koenig, 2013; Masters and Hooker, 2013). Before considering this body of evidence it is useful to discern what is meant for one to self-identify as religious and/or spiritual. Religiosity has been described as the organization of life doctrines and creeds around a tradition of bringing oneself closer to the Divine, that is, what may be culturally referenced as Yahweh, God, Buddha, Allah, etc., in accordance with affiliated institutions of worship. Spirituality is also described as a committed journey toward the Divine, albeit via what some describe as a more functionally dynamic and intrapersonal approach (Hill and Pargament, 2008). The vast majority of Americans identify themselves as being both religious and spiritual, suggesting the two constructs are not mutually exclusive (Marler and Hadaway, 2002). However, a growing segment of the non-secular US population self-identify as either religious but not spiritual or spiritual but not religious (Zinnbauer et al., 1997). This begs the question of what principles, beliefs or attitudes underscore these non-secular orientations and how this might translate to psychosocial functioning, behavior and cardiovascular health? Some have associated spiritual-but-not-religious identity with a devaluing or distrust of traditional norms in lieu of individualism and personal conscience (Fuller, 2001; Roof et al., 1999). Similarly, religious-but-not-spiritual individuals express a bias toward the culturally supported norms of organized religion in lieu of a more amorphous entity that is spirituality (Hill and Pargament, 2008).
Although R/S identity is a useful way to categorize non-secular cohorts, the vast majority of emperical evidence for R/S varaibles and CVD risk have compared R/S activities such as frequency of prayer, meditation, and church attendance (Baetz and Toews, 2009; Koenig, 2012; Rayburn, 2004). Nationally representative cohort studies have been particulary useful in elucidating the relationhsip between R/S factors and CVD risk. For example, frequency of prayer, religious study, and attendance at religious services were linked to lower blood pressure and reduced risk for HTN in the third National Health and Nutrition Examination Survey (Gillum and Ingram, 2006). In contrast, data collected from over 3000 adults from the Chicago Community Adult Health Study found increased likelihood for HTN with greater frequency of prayer and elevated diastolic blood pressure for those self-identified as spiritual (Buck et al., 2009). One possible approach to reconciling these disparatae findings is to consider the myriad of potential interactions between R/S factors and biopsychosocial mediators for HTN risk. For example, men with elevated risk for HTN report lower levels of spirituality and greater levels of hostility than their healthy counterparts (Sethness et al., 2005). As it pertains to health behaviors, a meta-analysis of over 100 studies found lower prevalence of smoking, alcohol consumption, and drug use in R/S individuals although the findings were not consistent for fruit, fiber, fish, and green vegetable intake (Koenig, 2014). As it pertains to interpersonal functioning, both cross-sectional and longitudinal studies support an increased number of social relationships and lower report of loneliness with greater frequency of church attendance (Koenig et al., 2012; Rote et al., 2012; Strawbridge et al., 2001). This is not to suggest that all aspects of spirituality and religion have benign psychosocial outcomes as troubled relationships with God or interpersonal conflict in the religious setting are linked to elevated levels of distress (Ellison and Lee, 2010; Krause and Wulff, 2004).
Here, we use biological, behavioral, and psychosocial data gathered from the Landmark Study of Spirituality and Health to test the moderating effect of R/S identity on the direct and indirect effects of hostility on blood pressure using a structural equation modeling (SEM) approach. We predict the effect for hostility on elevated blood pressure will be mediated via pathways through social isolation and unhealthy behaviors, while controlling for traditional risk factors for HTN and CVD. Furthermore, we predict R/S identity will moderate these paths wherein the magnitude of the effect of psychosocial and behavioral variables on blood pressure will be lower within individuals self-identified as religious and/or spiritual.
Methods
Sample
This study was approved by a review committee on the protection of human subjects at the University of Michigan. The data for this study come from the Landmark Spirituality and Health Survey (LSHS), a nationwide face-to-face survey of adults aged 18 years and older who reside in the continental United States. This survey, which was completed in 2014, was conducted by the National Opinion Research Center (NORC) (for a detailed description of the sampling procedure and questionnaire, see http://landmarkspirituality.sph.umich.edu/). The response rate for the study was 50 percent. The total number of completed interviews was 3010. The analyses that are presented below are based on a maximum-likelihood analysis on a subsample of participants in the LSHS interviews. The sample size used to create the hypothesized model (N = 2971) is smaller than the initial sample size due to the removal of 46 cases where the participant did not know (n = 33), refused to respond (n = 6), or there was missing data (n = 7). The model was tested in the full sample and in a sample that was subdivided based on response to the survey item “Which of the statements best describes you?” The distribution for the various endorsements to this item were as follows: (1) I am spiritual and religious (n = 1624), (2) I am spiritual but not religious (n = 855), (3) I am religious but not spiritual (n = 234), and (4) I am neither spiritual nor religious individuals (n = 258).
Measures
The structural model for hostility and blood pressure comprised several survey items collected during door-to-door interviewers conducted by LSHS interviews.
R/S identity
Survey respondents endorsed their religious and spiritual identity by endorsing one of the following: spiritual and religious (S+R+), spiritual but not religious (S+R–), religious but not spiritual (S–R+), and neither spiritual nor religious (S–R–).
Unhealthy behavior
Survey measures were selected for the latent factor of unhealthy health behaviors that are most salient in their link to HTN and CVD. Drinking frequency reflects the average number of days within a given month the respondent consumed an alcoholic beverage. This measure was chosen due to its documented relationship with psychosocial functioning and CVD risk. A higher number corresponds to more frequent alcohol consumption. Fruit and vegetable consumption reflects the average number of days in each week that the participant consumed at least five servings of fruits and vegetables. A high score stands for more frequent consumption of fruits and vegetables. Smoking is a single item reflecting the current smoking status of the study participant. The measure was dichotomous wherein a positive value defines a current smoker.
Hostility
We chose to focus on the cynical component of hostility as a trait construct in the context of reflecting a psychosocial risk for CVD due to its association with the frequent socially induced experience of hostility (Barefoot et al., 1983, 1989; Smith and Frohm, 1985). Five questions were selected from the Cook Medley Hostility Scale to reflect the cynical, that is, cognitive component of hostility (Cook and Medley, 1954). Hostility was assessed by combining the scores of five statements using a 4-point Likert scale ranging from strongly disagree to strongly agree. The statements include the following: I think most people would lie to get ahead, Most people make friends because friends are likely to be useful to them, Most people will use somewhat unfair means to gain profit or an advantage rather than lose it, Most people inwardly dislike putting themselves out to help other people, and I commonly wonder what hidden reason another person may have for doing something nice to me. The minimum score was 5 and the maximum score was 20. The reliability of the scale in the whole sample was α = 0.81.
Social isolation
Social isolation was assessed using a 3-point Likert scale ranging from seldom to often using three questions: How often do you feel that you lack companionship? How often do you feel left out? and How often do you feel isolated from others? Items were reverse scored so that higher numbers reflected less social isolation and greater perception of social support. The reliability of the items was α = 0.77.
Blood pressure
Systolic and diastolic blood pressure were obtained, by trained assessor, using the ihealth Wireless Blood Pressure Wrist Monitor BP7. Empirical support has been published in support of the validation for the iHealth BP7 wrist blood pressure monitor, for self-assessment, based on the European Society of Hypertension International Protocol revision 2010 (Wang et al., 2014). While there have been a number of studies suggesting wrist-cuff-derived blood pressure overestimates blood pressure recorded from the upper arm or conventional sphygmomanometry (Palatini et al., 2004; Zweiker et al., 2000), these reported inaccuracies are widely observed during home self-assessment and have mainly been attributed to arm positions held above or below the heart (Khoshdel et al., 2010; Mourad et al., 2005). Furthermore, it has been shown that recommended use of the wrist device by patients in the home setting provides accurate readings according to the British Hypertension Society protocol (Cuckson et al., 2004). To avoid these caveats, participants were asked to sit quietly in a chair with eyes forward and arms flat on the rests. The blood pressure cuff was attached to the left wrist and the participant remained seated at rest for 5 minutes. Systolic and diastolic blood pressure were assessed at 7 minutes and then again at 9 minutes. These measures were then averaged together to derive seated resting systolic and diastolic blood pressure.
Control variables
Several covariates were chosen and entered into the model based on their documented association with elevated blood pressure and risk for HTN. This included sociodemographic variables (e.g. age, male gender, and education level as a proxy for socioeconomic status) and cardiometabolic disease status (e.g. HBA1c, current diagnosis, and/or treatment for diabetes or HTN) (Chobanian et al., 2003). Age and education were scored continuously in years while sex (1 = men; 0 = women) and race (1 = Black; 0 = other race/ethnicity) were scored in a binary format. A marker of Black heritage was included in the analyses because significant interactions have been observed for religious/spiritual variables and CVD risk in African Americans (Ferraro, 2014). In addition, we controlled for cardiometabolic disease risk via (1) history or current diagnosis/treatment for HTN or high blood pressure, (2) history or current diagnosis/treatment for diabetes or high blood sugar, and (3) current HBA1c (O’Connor et al., 2009).
Statistical approach
Data were analyzed in the following steps. First, descriptive analyses were conducted to determine skew and kurtosis and the need to conduct log-transformations. A measurement model for the latent variable of unhealthy behavior was then evaluated. After testing the total effect for hostility on blood pressure, a two-stage SEM approach was used to test mediation of this effect via indirect paths through social isolation and the latent variable for health behavior, within the full sample. Next, R/S identity was tested as moderator of the full SEM model using the multiple-groups approach in the Mplus v.7.4 statistical program. This allowed for the magnitude of effects across the hypothesized paths to be formally compared between groups and evaluated by significance of the Wald test.
Means and standard deviations of all variables included in the model were compared between the religious and spiritual identity groups using an independent samples T-test in SPSS 24. Using Mplus, a SEM was specified to produce unbiased parameter estimates for the relationship among psychosocial, behavioral, and cardiovascular variables as a function of R/S identity while simultaneously accounting for sociodemographic and cardiometabolic risk factors. Factor loadings and residual error variance were evaluated for significance at the 0.05 level. Based on recommendations for SEM (Byrne, 2013), the measurement model was first estimated to examine the relationships between the health behavioral indicators for the proposed latent variable. The percentage of missing data for the exogenous variable of hostility was 3 percent, about 15 percent of subjects had missing responses on social isolation, from 0.1 to 19 percent on health behaviors and 42 percent on systolic and diastolic blood pressure due to many individuals refusing to take part in the blood pressure assessment. Full information maximum likelihood (FIML) is a feature built into Mplus (Muthén and Muthén, 2010) software that allows the operator to compute maximum likelihood parameter estimates and standard errors from data with missing values effectively allowing data from all cases to be included regardless of missing values provided that data are missing at random (Enders and Bandalos, 2001). Several fit indices were used in this study to evaluate the fit of a model. The chi-square statistic was reported; however, it is often not used to evaluate path models because of inflation issues inherent with larger sample sizes (e.g. >200; Hooper et al., 2008; Jöreskog and Sörbom, 1993). Comparative fit index (CFI), root mean square error of approximation (RMSEA), and Standardized Root Mean Square Residual (SRMR) were also reported (Bentler, 1990; Hu and Bentler, 1999; Jöreskog and Sörbom, 1993; Steiger, 1990; Weston and Gore, 2006).
Before evaluating model fit indices, we first examined a measurement model for the latent endogenous variable of unhealthy behavior. The construct need have at least three indicators wherein error terms were uncorrelated with each other in order to be retained in the final model. Based on our hypothesis and confirmed by review of covariance matrices, alcohol consumption was selected as the reference indicator for unhealthy behavior with the loading set at 1.00 for the purpose of scaling. First, a saturated model with all possible paths was examined in a measurement model. The model accounted for the complex survey design, specified with the “Type = Complex” statement, including sampling weights, clustering, and stratification provided in the data. This was followed by estimation of the proposed mediation model in order to determine whether the hostility-blood pressure path was structurally mediated by social isolation and health behaviors. Figure 1 depicts the hypothesized indirect paths from hostility to blood pressure via (1) social isolation, (2) unhealthy behaviors, and (3) unhealthy behaviors by way of social isolation. Indirect effects were calculated by multiplying the direct effects between predicting, mediating, and outcome variables. In addition, the total effect of hostility on blood pressure was evaluated after allowing the alternative paths from hostility to the proposed mediators (social isolation and unhealthy behaviors) to be freely estimated. A multiple-groups approach was taken to determine whether the structural paths of the mediation model differed pairwise as a function of R/S identity, that is, self-identification as (1) religious and spiritual, (2) spiritual, (3) religious, or (4) neither religious nor spiritual identity. To examine whether individual paths between hostility and blood pressure were moderated by religious/spiritual identity, we used the Wald test of parameter constraints feature of Mplus. The Wald statistic determines the extent to which the parameter estimates in the unconstrained model differ from that of the constraint model wherein the difference in paths is set equal to zero, taking into account sampling error. A significant Wald test statistic suggests the groups of interest differ substantially in the magnitude of the effect size for a specific pathway. A non-significant test suggests that the two groups have similar fit and therefore the collapsed estimate allows the most parsimonious model to be maintained. Based on the recommendations for testing structural mediation, the model was run with 10,000 bootstrap samples to examine the significance of indirect effects. The bootstrap standardized indirect path coefficients and 95 percent bias-corrected confidence intervals (95% CI) were reported. Indirect effects are significant if their 95 percent CI does not include zero (Mackinnon et al., 2007).
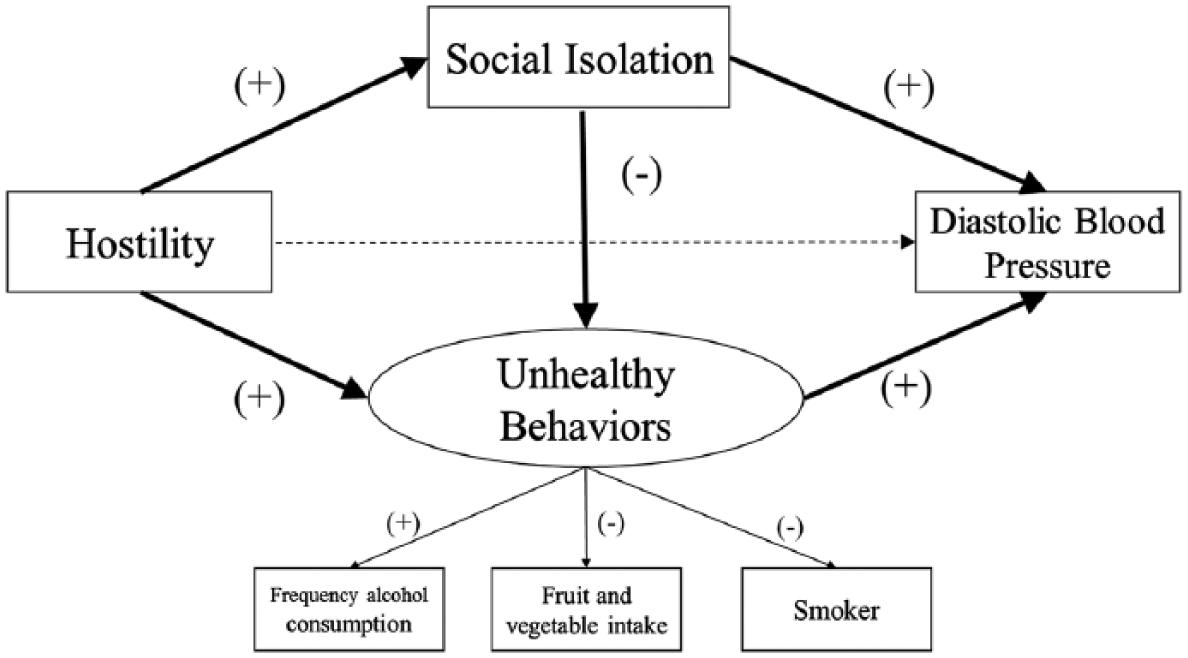
Proposed mediation model.
Results
Group descriptives
The groups differed widely across each endogenous variable and covariates used within the model with the exception of HBA1 and social isolation. The R/S group was the oldest and consisted of the highest proportion of females and fruit/vegetable intake. Moreover, over 38 percent of these individuals reported previous diagnoses or treatment for high blood pressure and 16 percent for diabetes, the largest proportion of any group. Whereas Religious and Spiritual groups were similar across a number of measures, individuals endorsing the statement “religious but not spiritual” had the highest proportion of Blacks, lowest education as well as fruit and vegetable intake, and reported the highest levels of hostility. The non-religious or spiritual group had the lowest percentage of Blacks, highest percentage of males, lowest proportion of individuals with history or treatment of high blood pressure or diabetes, and reported the highest number of days consuming alcohol (i.e. approximately 1 out of every 3 days). Table 1 shows the values reported in each group.
Descriptive for model variables based on religious/spiritual identity.
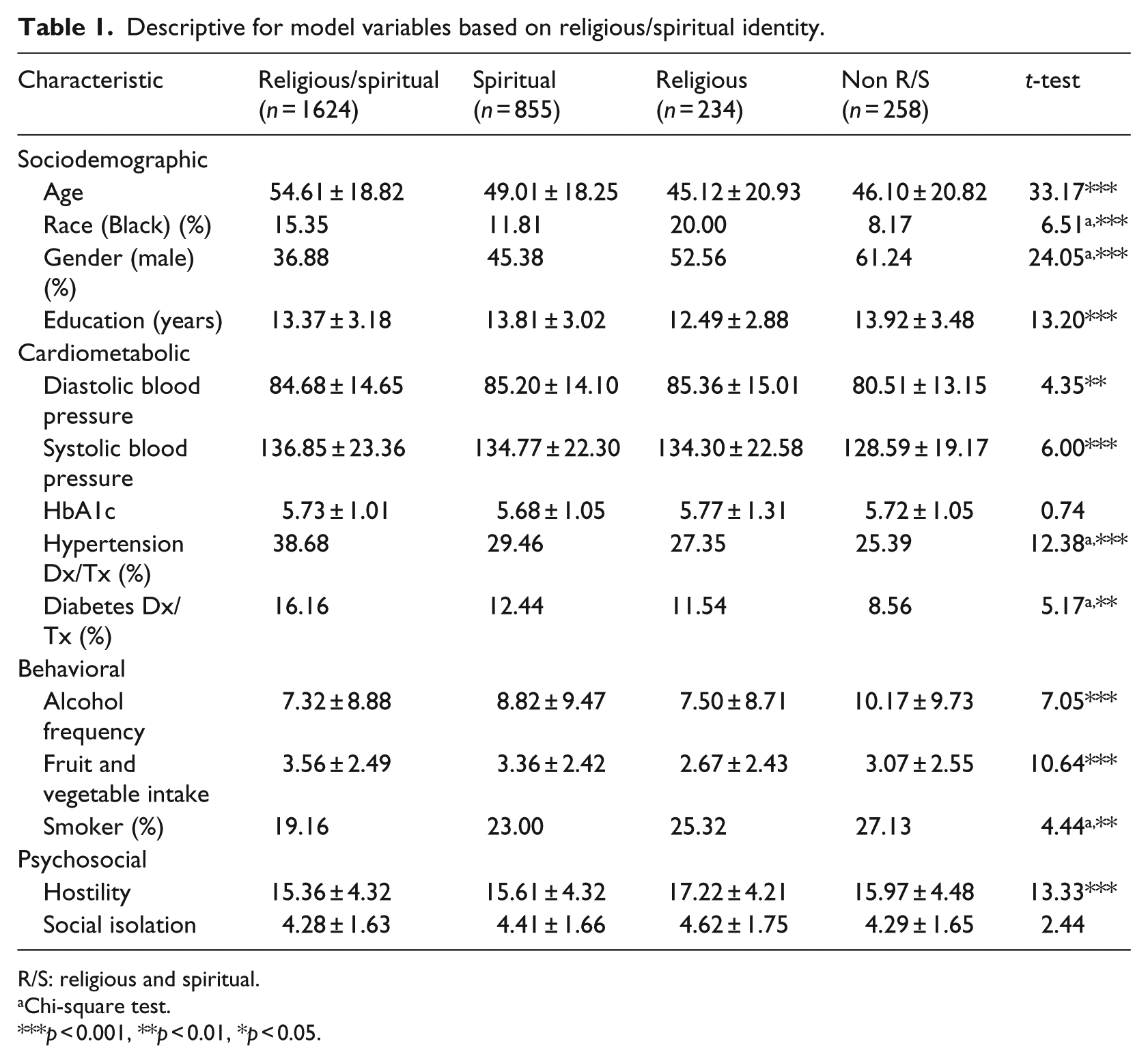
R/S: religious and spiritual.
Chi-square test.
p < 0.001, **p < 0.01, *p < 0.05.
SEM
Measurement model
Confirmatory factor analysis verified the latent variable “unhealthy behavior,” within the entire sample, measured by the variables “Drinking frequency” (β = 0.49; 95% CI: 0.41 to 0.58; p < 0.001), “fruit and vegetable consumption” (β = –0.46; 95% CI: –0.54 to −0.40; p < 0.001), and “smoking” (β = 0.44; 95% CI: 0.36 to 0.51; p < 0.001). There was no significant difference in loadings for the health behavior factor between groups.
Mediation model specification
Prior to moderated-mediation model specification, the total effect for hostility on systolic blood pressure (SBP) and diastolic blood pressure (DBP) was confirmed within the total sample. A significant total effect for hostility was present on diastolic (unstandardized β = 0.24; 95% CI: 0.06 to 0.41; p < 0.01), but not systolic (β = 0.05; 95% CI: –0.04 to 0.15; p > 0.05) blood pressure. Subsequent test of the structural model for the intermediary paths between hostility and DBP also suggests excellent model fit (CFI = 0.98; RMSEA = 0.02; SRMR = 0.01). Table 2 shows that within the full sample, hostility is associated with a higher report of social isolation and unhealthy behaviors. Unhealthy behaviors have a positive effect on DBP. Also evident was more social isolation was associated with unhealthier behaviors but had no effect on DBP, within the full sample. Indirect effects for hostility on DBP are also presented in Table 2. In the full sample, there was a significant indirect path from hostility to DBP as a function of unhealthy behaviors. Hostility was also indirectly associated with unhealthy behaviors as a function of greater social isolation.
Path estimates included in the model for the religious/spiritual groups.

DBP: diastolic blood pressure; CI: confidence interval; S+R+: religious and spiritual; S+R–: spiritual but not religious; S–R+: religious but not spiritual; S–R–: non-religious and spiritual.
p < 0.001, **p < 0.01, *p < 0.05.
Moderated-mediation model specification
A simple test for moderation of the direct path between hostility and DBP showed excellent model fit (CFI = 1.00; RMSEA < 0.01; SRMR < 0.01). The effect was greater for individuals self-identified as S+R+ (β = 0.23; 95% CI: –0.02 to 0.48; p = 0.08) and S+R– (β = 0.33; 95% CI: 0.05 to 0.62; p = 0.02) compared with S–R+ and S–R– individuals. Table 2 also presents parameter estimates for the full moderated-mediation structural model predicting DBP as a function of R/S identity. The pattern of effects for the full model most closely resembled that of the S+R+ group, likely due to the larger size of this cohort. Compared to the full model, the pattern of direct effects for hostility on social isolation and social isolation on unhealthy behavior were reversed for the S–R+, S+R–, and S–R– groups. The direct effect for social isolation on DBP was only present in the S–R+ group. The effect for social isolation on DBP was also uniquely observed in S–R+ group. The formal test for moderation of the intermediary pathways is presented using the Wald statistic in Table 3. Compared to S–R– individuals, the path from unhealthy behaviors to elevated DBP was greater for those endorsing some form of religious identity, that is, S–R+ and S+R+. Compared to S–R–, the direction of the association for the path from hostility to social isolation and from social isolation to unhealthy behaviors was reversed for persons endorsing S+R+.
Wald test for group differences in intermediary pathways.
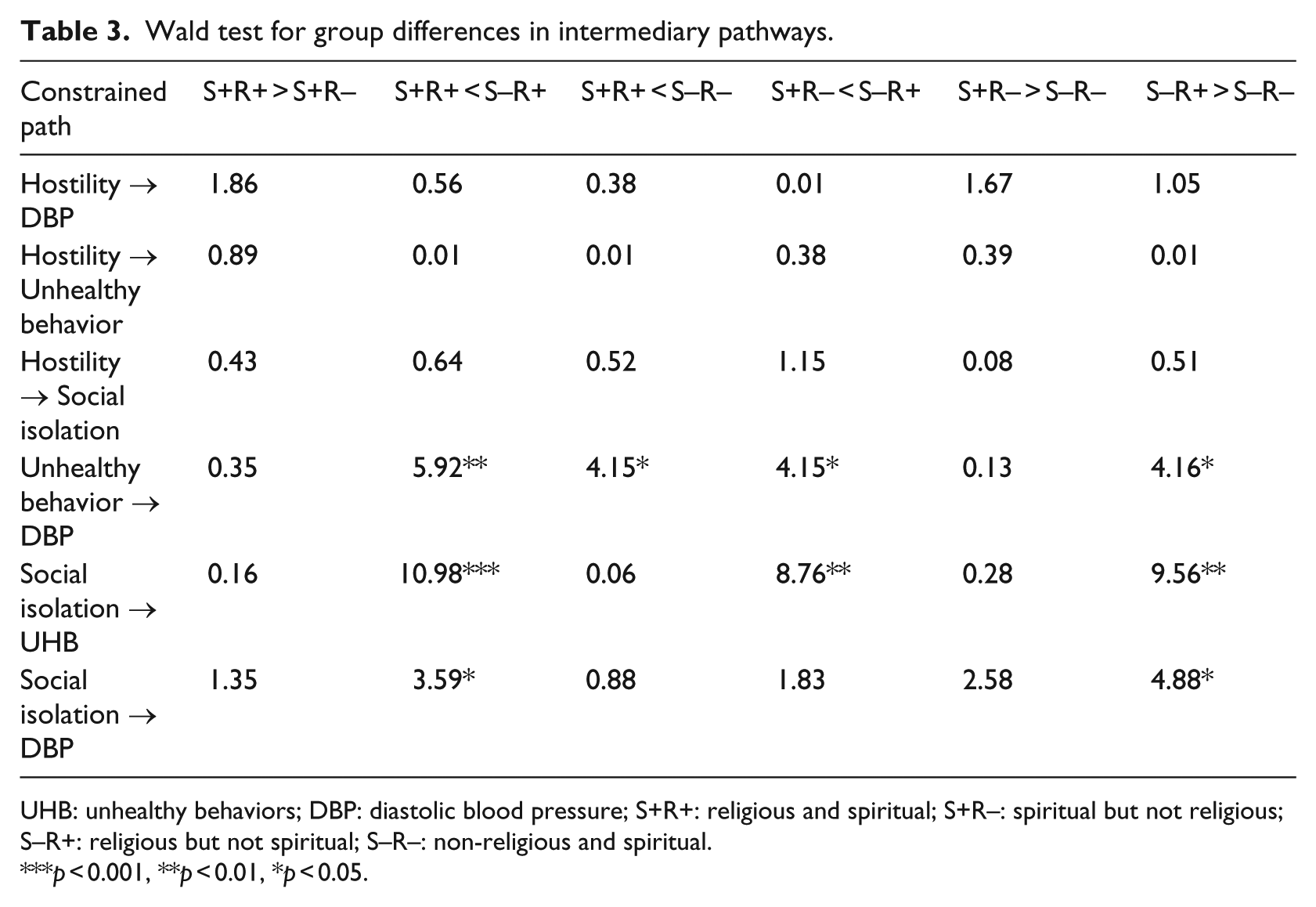
UHB: unhealthy behaviors; DBP: diastolic blood pressure; S+R+: religious and spiritual; S+R–: spiritual but not religious; S–R+: religious but not spiritual; S–R–: non-religious and spiritual.
p < 0.001, **p < 0.01, *p < 0.05.
Covariates
Prior to formal testing for moderation of the intermediary paths between hostility and DBP, the selected covariates were entered into the model in order to account for the significant effects of sociodemographic and cardiometabolic risk factors for HTN. The effect and variance accounted for each of these variables in self-report of social isolation, unhealthy behaviors, and resting DBP is presented in Table 4 as a function of R/S group affiliation. Across groups, older age was associated with a greater report of social isolation, unhealthy behaviors, and in most cases elevated DBP. Male gender was associated with unhealthier behaviors and social isolation across groups, and higher DBP for individuals self-identified as religious and spiritual. Similarly, older age was positively correlated with unhealthy behaviors, social isolation, and DBP. Blacks in both the religious and spiritual and neither religious nor spiritual groups showed elevated DBP. Lower education was consistently associated with unhealthy behaviors and for spiritual and non-R/S individuals, greater social isolation. Although HBA1c and diabetes were positively, and history of HTN negatively, related to elevated DBP in the entire sample, these associations varied widely in the subgroup models.
Total variance (R2) accounted for in each with and without the inclusion of covariates and their parameter estimates.
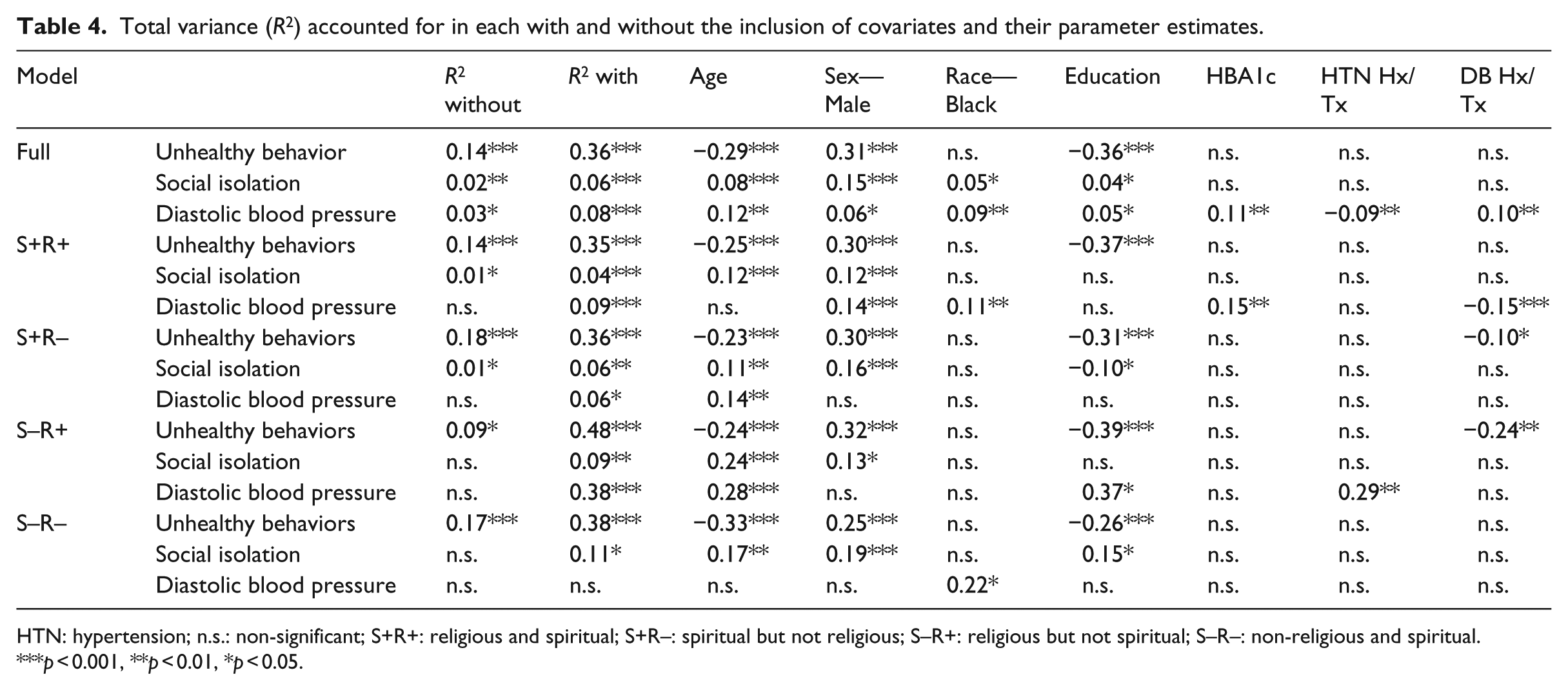
HTN: hypertension; n.s.: non-significant; S+R+: religious and spiritual; S+R–: spiritual but not religious; S–R+: religious but not spiritual; S–R–: non-religious and spiritual.
p < 0.001, **p < 0.01, *p < 0.05.
Explained variance
Total variance accounted for in the final model, with and without the inclusion of control variables, along with parameter estimates of each covariate on the endogenous variables in the model are presented in Table 4. The inclusion of covariates allowed for the explanation of at least 2× greater variance in each endogenous variable, particularly the unhealthy behavior latent factor. As it pertains to blood pressure, the final model explained 9 percent of the variance in DBP for S+R+, 6 percent of the variance in DBP for S+R–, 38 percent of the variance in DBP for S–R+ individuals, and a non-significant proportion of the variance in DBP for non-religious or non-spiritual individuals.
Discussion
The aim of this study was to evaluate the mitigating role of R/S identity on the total and indirect effect of hostility and blood pressure via psychosocial and behavioral pathways. The total effect was confirmed for hostility on DBP but not SBP. Furthermore, our modeling suggests that hostility indirectly relates to elevated DBP as a function of unhealthy behaviors and that hostility relates to unhealthy behaviors as a function of greater social isolation, findings that have been well characterized in the literature (Smith et al., 2004).
Upon examination of individual paths as a function of R/S identity the magnitude of the effect for unhealthy behaviors on elevated DBP was greater for religious-only individuals. This was unexpected given the aforementioned literature suggesting a cardioprotective role for religious activties on blood pressure and risk for HTN (Gillum and Ingram, 2006). Furthermore, although religious activities have been linked to elevated DBP in large community samples, this effect was only noted in persons endorsing spiritual identity (Buck et al., 2009). Although the literature suggests that religious affiliation largely protects against unhealthy behaviors such as drinking and smoking while facilitating abstinence and maintaining distinctive dietary habits, it should be noted that these effects are shown to be mitigated by frequency of religious attendance (Strawbridge et al., 2001). This underscores the importance of accounting for contextual behavioral R/S factors when interpreting behavioral risk for elevated blood pressure in self-identified religious individuals. Nevertheless, nationally representative studies have noted positive associations between religious activities and spirituality on blood pressure and risk for HTN (Buck et al., 2009).
Individuals self-identified as spiritual and religious showed a buffering effect for hostility on social isolation and social isolation on unhealthy behaviors that was not evident in persons identified as religious-only or spiritual-only. One possible interpretation of these findings stems from the observation that a combination of religious and spiritual affiliation engenders a better ability to cope with stress than spiritual-but-not-religious orientation (Graham et al., 2001). Therefore, it can be argued that a non-conflicting spiritual and religious orientation engenders a broad array of potential support mechanisms that may thwart loneliness due to cynical hostility. For example, fellowship with a religious support group anlong with finding meaning and purpose in one’s interpersonal interactions are common for persons endorsing religious and spirituality (Salsman et al., 2005). The inverse effect for social isolation on unhealthy behaviors in S+R+ is more intuitive. Prior literature suggests healthy social engagement in public religious activities such as prayer and church attendance relate to healthier lifestyle and eating behaviors (Zinnbauer et al., 1997, 1999). Conversely, socially isolated individuals make uninformed medical decisions, experience increases in cumulative stress due to lack of social resources, and report of unhealthier lifestyles (Cacioppo et al., 2003). It has been well documented that insecurity with respect to social attachment is not only common in religious individuals but may actually provide a developmental pathway toward religiosity (Granqvist et al., 2010). Moreover, religious tradition and the associated observances and dietary restrictions may influence positive dietary and lifestyle choices of the most devout (Eliasi and Dwyer, 2002; Meyers et al., 2017; Moscati and Mezuk, 2014; Sabate, 2004). Emergent research addressing perceived sanctification of the body, in religious and spiritual individuals, and its effect on behavioral health patterns seems poised to address questions pertaining to buffering effect of S/R identity on psychosocial risk for unhealthy lifestyle (Dittmann and Freedman, 2009; Mahoney et al., 2005; Pargament and Mahoney, 2005).
Limitations
One fundamental limitation of our interpretation of this model is the cross-sectional design does not allow us to infer causality among the paths. Longitudinal studies are required to confirm the direction of the associations presented in the model, particularly that of the relationship between hostility and DBP. Nonetheless, the psychosocial model presented suggesting CVD risk for cynical hostility is empirically supported via processes related to psychophysiological reactivity, psychosocial vulnerability, and behavioral health risk (Smith et al., 2004). Despite the robust effects for these psychosocial variables on DBP after controlling for traditional sociodemographic and cardiometabolic risk factors for HTN, there are a number of clinical and subclinical markers of CVD that underlie hypertensive risk (e.g. vascular endothelial dysfunction and left ventricular mass hypertrophy), which were unaccounted for in the model. Finally, since hypertensive diagnosis was not used as the predictor variable, the biopsychosocial model for diastolic blood pressure is likely overestimated in terms of risk for HTN.
Conclusion
The idea that religiosity and spirituality relates to blood pressure levels and risk for HTN has been around for several decades with the majority of studies citing an inverse relationship between religious involvement and diastolic blood pressure (Koenig et al., 2012; Levin and Vanderpool, 1989). This study expands the scope of these documented relationships while providing new insight into the processes through which R/S identity may relate to hypertensive risk. Unlike much of prior work within the field, religious and spiritual affiliation was modeled as a moderator of psychosocial and behavioral pathways for HTN and CV risk. Doing so affords the opportunity to identify unique psychosocial and behavioral pathways whereby R/S identity may mitigate the risk for elevated blood pressure. Conducting this analysis in a nationally representative sample recompenses for some of the methodological limitations of previous work such as age-restricted and non-representative samples. Through this approach, several unexpected findings arose from our analysis. First, a pattern emerged wherein the effect for unhealthy behavior on DBP was greater for individuals endorsing religious identity when compared with the reference group. Yet another unexpected finding was that compared to other groups religious but not spiritual individuals reporting higher levels of social isolation engaged in unhealthier behaviors. That non-religious and non-spiritual individuals did not exhibit behavioral or psychosocial risk for elevated blood pressure was unexpected when considering prior work. It is likely that the demographic characteristics of this group may have afforded some protection against CV risk. Overall, this study adds to a growing body of literature linking religious and spiritual identity to psychosocial and behavioral risk for elevated blood pressure (Calhoun et al., 2001; Cougle et al., 2013; Kahler et al., 2004; Scherwitz et al., 1992; Whiteman et al., 1997). Moreover, it adds to a growing body of literature suggesting the co-existence of religousness and spirituality is associated with a eudiamonic orientation that emphasizes warm interpersonal style, positive relationships with others, and beneficial interpersonal outcomes (Jordan et al., 2014). These interactions may protect the religious and spiritual individual from the negative consequence of hostility on social isolation as well as subsequent effect of social isolation on unhealthy behaviors. It is our hope that future research will delve more deeply into the influence of contextual factors pertaining to R/S identity such as frequency of religious activities, spiritual-religious struggles, and sanctification on behavioral health patterns and subsequent risk for HTN and CVD.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received the following financial support for the research, authorship, and/or publication of this article: Funding for this study was provided by a grant from the John Templeton Foundation.