
Abstract
The purpose of this study was to explore the feasibility, acceptability, and efficacy of a telephone-based smoking cessation intervention for lung screening patients. Participants (N = 39) were enrolled in a single-arm pilot study of a four-session telephone-based intervention. Self-report measures were completed at baseline, post-intervention, and 3-month follow-up. Participants were long-term smokers; 62 percent were not motivated to quit. Twenty-three percent attempted quitting, 29 percent decreased their smoking, and 11 percent reported abstinence. Confidence increased (p < .001) and there were trends toward increased importance (p = .09) and comparative disease risk (p = .02). This intervention was acceptable and associated with improvements in smoking-related beliefs and behaviors.
Introduction
Each year in the United States, more than 220,000 individuals are diagnosed with lung cancer, and 87 percent of lung cancer deaths are attributable to smoking (American Cancer Society, 2016). The prognosis for patients with lung cancer has traditionally been poor, largely because only 15 percent of lung cancer patients are diagnosed at early stages (NCI Surveillance, Epidemiology, and End Results Program, 2017). However, the National Lung Screening Trial (NLST) demonstrated that screening with computed tomography (CT) resulted in a significant reduction in lung cancer mortality (National Lung Screening Trial Research Team et al., 2011). Lung cancer screening has been endorsed by the Centers for Medicare and Medicaid Services and the US Preventive Services Task Force (Fucito et al., 2016; McMahon et al., 2011). The increased adoption of screening with CT creates a critical opportunity to promote smoking cessation.
Smoking prevention and cessation remain the fundamental strategies to reduce the number of cases of lung cancer (Moyer, 2014), and lung screening programs should include tobacco cessation services as part of the multidisciplinary effort. However, a recent systematic review concluded that there is limited research on the efficacy of smoking cessation interventions for lung screening patients, with only six trials conducted to date (Piñeiro et al., 2016). This study seeks to address this finding and contribute to the literature centered on efficacy for lung screening programs that utilize smoking cessation interventions.
Approximately half of the patients undergoing lung screening are current smokers (Mazzone, 2012; Park et al., 2015). Research suggests that quitting smoking upon lung cancer diagnosis can improve chances for treatment efficacy, reduce chances of secondary tumors, and may double chances of survival (Parsons et al., 2010). Thus, to increase the benefits of CT, smoking cessation paired with screening is included in guideline recommendations (Marshall et al., 2013; Moyer, 2014). There is also cost-effectiveness of increased smoking cessation in the CT screening context (Evans and Wolfson, 2011). Smoking cessation programs that coincide with lung cancer screening are likely to produce better smoking cessation success rates and increase motivation to quit than just CT screening alone (Davis et al., 2015; Parks et al., 2016). Correspondingly, undergoing screening may enhance abstinence motivation and quitting among current smokers and may prevent relapse among former smokers (Tammemagi et al., 2014). Modifying health behaviors is a significant challenge and innovative approaches to behavior change increasingly require messages that are relevant and persuasive. Tailored or targeted interventions are designed to match the content to the needs of a patient (Noar et al., 2007). In fact, in a Cochrane Review, personalized tobacco cessation materials were more effective than standard materials (Lancaster and Stead, 2005).
Tobacco cessation for lung cancer screening presents a unique challenge. Patients may have a lung cancer screening CT ordered as part of an annual visit with their primary care provider, or even outside of a visit, and screenings are performed at a later time and could be done at several locations (Davis et al., 2015). There are also several options for discussing lung screening results (Parks et al., 2016). Capturing patients for tobacco cessation services when they are navigating this process can be challenging because of the diversity of patient flow through the system (An et al., 2006; Battaglia et al., 2016; Mak et al., 2015; Parks et al., 2016). It is also difficult for large hospitals and health centers to provide tobacco treatment to all lung screening patients because there is no one point of entry into the system and no one designated department to cover the costs. Protocolized interventions that provide smoking cessation counseling to patients virtually by telephone could overcome these challenges and be implemented across various healthcare settings. The purpose of this study was to explore the feasibility, acceptability, and preliminary efficacy of a telephone-based smoking cessation intervention for lung screening patients.
Materials and methods
Study design
We conducted a pilot feasibility study of a telephone-delivered smoking cessation program—Project Reach. Project Reach was a tailored risk-based smoking cessation intervention, delivered following screening via four telephone sessions. We enrolled 39 adult smokers, between February 2015 and February 2016, from a large academic medical center who had undergone lung screening or were seen in a multidisciplinary pulmonary nodule clinic (Supplemental Figure 1). Participants completed baseline and 12-week follow-up assessments. The study was approved by the human subjects committee Partners HealthCare. Eligibility criteria included any adult patient (>18 years) seen in the Pulmonary Nodule Clinic or any individual who had received low-dose computed tomography (LDCT) scan for lung screening at MGH satellite clinics, or affiliates. Adult patients had to smoke a cigarette, even a puff, in the past 30 days, speak English, be willing to consider trying to quit smoking using counseling, and have regular telephone access to be eligible for the study. Those who were ineligible did not have regular telephone access or had untreated psychiatric illness.
Eligible participants were identified after receiving an LDCT scan or attendance at the Pulmonary Nodule Clinic. Research staff approached patients in clinic or mailed patients a study information flyer and an opt-out letter. After 7 days, patients who did not opt-out were contacted by a research team member to discuss their study participation. Consent procedures were completed via telephone.
Intervention
A personalized counseling session script was created for the first session for each individual, based on responses to the lung screening survey (baseline; for example, average cigarettes a day, quit intentions, exposure to secondhand smoke, smoking-related diseases, and perceived risk of diseases). These responses were developed into a coded algorithm using logical formulas in Microsoft Excel and then generated into personalized scripts using Microsoft Word. Several aspects of the first counseling call were tailored to the patient based on baseline survey responses. For example, patients who indicated that there was no smoking allowed in their home received reinforcement and education about the benefits of a smoke-free home. Those who indicated that they smoke within 30 minutes of waking received education about nicotine dependence and ways to reduce dependence (e.g. by delaying the first cigarette of the day). In terms of risk perceptions, the counseling text was tailored to patient’s responses regarding whether they thought their risk of lung cancer and other smoking-related diseases (SRDs) was higher or lower than same-age peers or other smokers. First, participants were asked why they thought their perceived risk was higher or lower (e.g. “At your screening, you answered ‘lower’ to the question, ‘Compared to other smokers, what do you think your chance of getting a smoking-related disease is in your lifetime?’ Why do you think your risk of getting a smoking-related disease is lower than other smokers?”). They were then provided with information about their actual risk for heart disease, stroke, and lung cancer based on their sex; this information was also tailored to patients’ reported numeracy preferences on their baseline survey (e.g. presented as either “double the risk” or “2 times the risk”). Finally, patients were asked if they received their lung screening results, if they had questions about their follow-up care, and if their risk perceptions and/or motivation to quit changed as a result of lung screening.
All counseling sessions were performed by two trained counselors with specialized training in smoking cessation. As proactive telephone counseling with at least three telephone calls significantly increases the chances of quitting (Stead et al., 2006), four counseling calls were offered. The calls were delivered using a motivational interviewing style, a goal-oriented form of therapy in which therapists attempt to influence patients to consider making changes with the goal of examining and resolving ambivalence (Miller and Rollnick, 2013) and structured around the 5As, a common framework for behavioral change (Carrol et al., 2008; Glynn and Manley, 1989). Specifically, counselors asked participants about their smoking status and progress; they advised participants to quit by reflecting on values and goals aligned with smoking cessation; they assessed participants’ motivation, confidence, and readiness to quit; they assisted participants in making a quit plan, which may include advice about quit medications and management of cravings and withdrawal symptoms; and they arranged for follow-up by summarizing the treatment plan and emphasizing treatment adherence. Following an initial session guided by the individualized risk-tailored protocol (see Supplemental Figure 2 for example), sessions included information about quit medications (Session 2), social support (Session 3), and brief stress management skills to elicit the relaxation response (Session 4).
Measures
The baseline survey included measures of sociodemographics, medical history, and smoking history. Smoking status was assessed using the question, “Did you smoke a cigarette (even one puff) in the past 30 days?” Current smokers were then asked to report average number of cigarettes per day (Shen et al., 2010) and time to smoking after waking. Quit intentions were assessed using a 10-point Likert scale that assessed current stage in the process of quitting smoking (1 = “I enjoy smoking so much I will never consider quitting no matter what happens” to 10 = “I have quit and I am 100% confident that I will never smoke again”) (Garces et al., 2004; Park et al., 2009). Items were grouped into four categories to reflect quit intentions: no intentions to quit, vague plans to quit, preparing to quit, and currently quit. Participants were also asked to report the smoking status of their spouse or partner.
The baseline and follow-up survey assessed smoking/quit status, time to smoking, exposure to secondhand smoke (household smoking policy), and risk perceptions. Ten items assessed individual’s personal (individual) risk and comparative (related to others) risk perceptions for lung cancer and other SRDs. To assess lung cancer and SRD personal risk, two questions assessed the likelihood (1 = “very unlikely” to 5 = “very likely”) and danger (1 = “strongly disagree” to 5 = “strongly agree”) of developing lung cancer and SRD for that individual in general. For comparative risk, three questions asked about risk as compared with others of the same age and sex, and as compared with other smokers (lung risk, five-item scale: α = .87; SRD risk, five-item scale: α = .86; 1 = “much lower” to 5 = “much higher”) (Shen et al., 2010). At each counseling call, participants’ smoking status and any changes since the last call was recorded (e.g. quitting, change in smoking rate, and time to first cigarette). In addition, importance of quitting and confidence to quit were assessed using a single-item scale (0 = not at all important/confident to 10 = extremely important/confident).
On the follow-up survey, satisfaction questions asked about extent of the Project Reach program meeting the needs of the subjects, whether patients received the assistance they wanted, how the subjects would rate the quality of the assistance received, and how helpful the study was for the patients. Satisfaction questions also addressed what the subjects found most helpful, least helpful, challenging, and asked for recommendations.
Statistical analyses
Frequencies and descriptive statistics (mean values, SDs) were examined for baseline demographic, medical, and smoking history characteristics; smoking cessation outcomes after the intervention; and smoking behavior and confidence and importance to quit at each weekly counseling call. Inferential statistics were used to explore changes over time in dependent variables of importance to quit, confidence to quit, personal risk of lung cancer and SRD, and comparative risk of lung cancer and SRD. Given the small sample size, normality was assessed for each variable to ensure that parametric tests (i.e. repeated-measures analyses of variance (ANOVAs)) were appropriate, and sphericity was further examined for each analysis to ensure appropriateness of the test. All variables were normally distributed (skew and kurtosis around 1) and ANOVAs met the test for sphericity (p > .05) except for importance to quit, which was non-normally distributed at almost every time point (skew up to −2.05, kurtosis up to 4.97). Thus, repeated-measures ANOVAs were used to examine whether the change in confidence to quit across the four counseling calls was statistically significant, and to examine whether changes in risk perceptions from before to after the intervention were significant when controlling for actual SRD at baseline. Friedman’s chi-square test was used to examine changes in importance to quit across the four counseling sessions. We also used independent samples t test to assess whether smokers who quit or not quit at follow-up differed in terms of baseline intentions to quit.
Given the small sample size of this pilot study, p < .05 and p < .10 were considered to reflect statistical significance and meaningful trends, respectively. Partial eta-squared was reported as an estimate of effect size for the ANOVAs and interpreted as follows: .01 = small, .06 = medium, and .14 = large (Cohen, 1977). Cohen’s d was reported as an estimate of effect size for independent samples t test and interpreted as follows: .3 = small effect, .5 = medium effect, and .8 = large effect (Cohen, 1989). Content analysis was used to explore responses to open-ended satisfaction questions.
Results
Participants were, on average, 61.4 years old (SD = 7.4) and primarily men (69%) (Table 1). Almost half of participants reported a medical history of COPD or emphysema, and 23 percent had a previous cancer history. Participants had been regular smokers for an average of 45.7 years (SD = 7.7) and over half (59%) were heavy smokers (>10 cigarettes per day (cpd)). The majority of participants smoked within 30 minutes of waking (64%) and allowed smoking in the home (56%). Fifty-six percent reported that they had not made any past-year quit attempts, and 62 percent reported only vague thoughts or intentions to quit.
Demographics and medical smoking characteristics (N = 39).

COPD: chronic obstructive pulmonary disease; GED: General Equivalency Diploma.
Data were missing for history of stroke (n = 7), COPD/emphysema (n = 2), heart disease or heart attack (n = 6), family history of lung cancer (n = 2), time to smoking (n = 1), and number of quit attempts (n = 2).
Feasibility and acceptability
In total, 35 participants completed the 3-month follow-up survey (90%). In all, 25 participants (64%) completed all four counseling calls. The majority of participants responded that the program was helpful. One patient commented, I received some very helpful information about the benefits of quitting smoking. I now feel more confident about my chances of becoming a nonsmoker. Talking with someone who was supportive, nonjudgmental, and hopeful for my success was extremely important to me. I have become much more mindful of why and when I smoke.
Among participants who indicated the program had not met their needs, emotional support from the counselors and information regarding smoking cessation (e.g. positive support and quitting advice) were still reported to be helpful. Primary challenges to completing the study included difficulty committing to the study and finding time to participate. For example, one participant stated, The fault was mine. The timing was wrong for me. During the time of the trial I was extremely busy and did not give the program the time it deserved. Quitting for me is cyclical thing. I need to be in a low stress period before I feel capable of embarking upon such a drastic lifestyle change.
Another participant stated “My challenges were mental and emotional. I had to face my own fears and admit to my vulnerabilities in order for the program to be beneficial for me. And I believe I did this.” Suggested improvements to the program included adding additional counseling sessions and a longer study duration.
Changes in smoking behaviors and beliefs
For smoking outcomes (Table 2), at the final session, 16 percent of participants reported being quit at the final counseling call; all quitters had completed all four counseling sessions. At each call, more than half participants reported making changes since the previous session, which included tapering, obtaining, or beginning to use smoking cessation medications, delaying the time to smoking in the morning, and using behavioral strategies to cope with cravings. At the 3-month follow-up survey, 23 percent reported at least a 25 percent decrease in smoking. Fourteen percent of participants reported delaying their time to smoking in the morning and adopting a more restrictive household smoking policy. Nine percent (3/35) of treatment completers reported being quit for at least the past 7 days at 3-month follow-up. Participants who were quit at follow-up had reported greater quit intentions at baseline (t(42) = 2.14, p = .04; d = 1.71) as compared with participants who had not quit.
Smoking behaviors and beliefs.
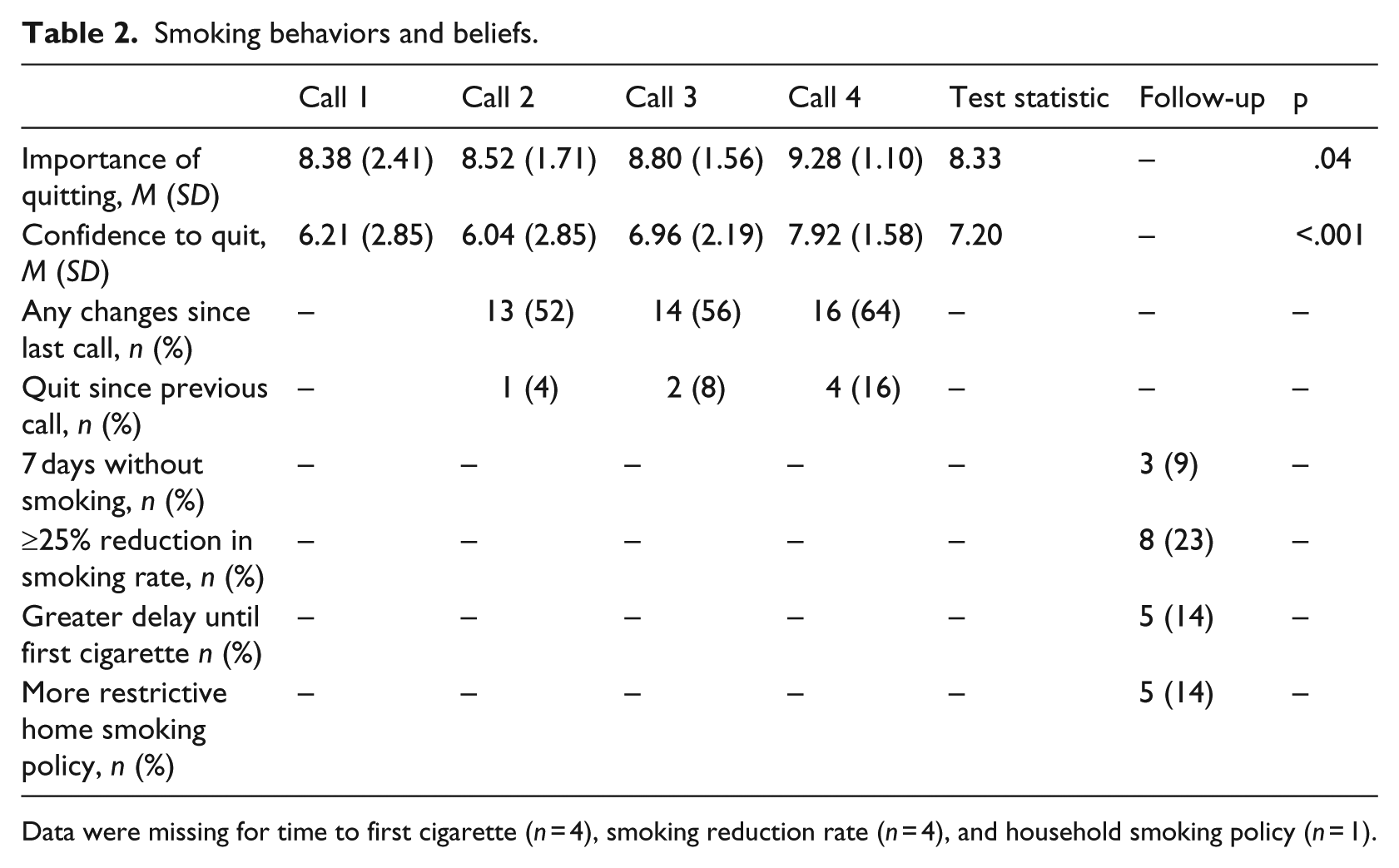
Data were missing for time to first cigarette (n = 4), smoking reduction rate (n = 4), and household smoking policy (n = 1).
Next, we examined changes in smoking-related beliefs. There was a statistically significant increase in confidence to quit from before to after the intervention (F(3,69) = 7.20, p < .001, ηp2 = .43). There was also a significant increase in importance to quit (χ2(3) = 8.33, p = .04). Personal risk of lung cancer and SRD did not change from before (M = 16.52, SD = 2.16) to after the intervention (M = 15.58, SD = 2.66) (F(1,29) = .26, p = .62, ηp2 = .01). In contrast, there was a significant increase in comparative risk of lung cancer and SRD (F(1,27) = 6.30, p = .02, ηp2 = .19) with an increase in risk perceptions from before (M = 22.41, SD = 3.59) to after the intervention (M = 23.59, SD = 4.48). Given the small sample size, we also calculated power achieved for these analyses, based on the observed effect size, sample size, alpha level of .05, number of measurements, correlation between repeated measures, and non-sphericity correction as appropriate. Results indicated achieved power for importance to quit = 96 percent, confidence to quit = 99 percent, personal risk of lung cancer and SRD = 15 percent, and comparative risk of lung cancer and SRD = 99 percent.
Discussion
The increased adoption of lung screening with LDCT creates an important opportunity for lung cancer prevention and smoking cessation. The results of this study suggest that a four-session intervention tailored to patients’ unique smoking and medical history and risk perceptions is a feasible way to promote improvements in smoking-related beliefs and behaviors, although more intensive interventions are needed to promote long-term quitting, given that smokers undergoing lung screening were long-term and addicted, and less motivated to quit.
Participants’ feedback about the program was positive, with the vast majority reporting that they found the program helpful for increasing their knowledge, motivation, and confidence about quitting. A recent systematic review concluded that there is limited research on the efficacy of smoking cessation interventions for lung screening patients, with only six trials conducted to date (Piñeiro et al., 2016). Thus, this study helps to develop the evidence base regarding the feasibility and acceptability of smoking cessation interventions, particularly telehealth interventions, for lung screening patients.
The current intervention yielded promising improvements in smoking behaviors and improvements in beliefs that underlie smoking behaviors. There was positive movement on changes in smoking beliefs that underlie smoking quit intentions and attempts, specifically in comparative risk perceptions, confidence to quit, and importance to quit (Gwaltney et al., 2009; Park et al., 2009; Piñeiro et al., 2016). Comparative risk perceptions were found to increase, which may reflect more realistic risk perceptions following lung screening results and education about smoking and SRDs. That is, comparative risk may have increased because participants learned through the lung screening process that their risk compared with others (e.g. non-smokers) was higher due to their smoking history. Comparative risk, in particular, is often underestimated by smokers (Arnett, 2000; Harris, 1996; Klein and Helweg-Larsen, 2002; Segerstrom et al., 1993; Weinstein, 1998; Weinstein and Klein, 1995) and thus it is promising that this tailored intervention appeared to have an effect. In the NLST trial, risk perceptions remained unchanged following screening (Park et al., 2013); our pilot work demonstrates an ability to effectuate these beliefs. These findings are consistent with research demonstrating the utility of motivational interviewing for smoking cessation in general (Hettema and Hendricks, 2010), and suggest the potential benefits of a motivational interviewing approach for lung cancer patients specifically.
Overall quit rates, however, remained low. A recent trial, conducted by Taylor et al. (2017), supported the efficacy of a longer duration (six-session) telephone intervention. Clinical and demographic characteristics of lung screening patients might account for the low quit rates and need for longer intervention duration. Participants in this study were older, long-term addicted smokers who initially had little motivation to quit, which is consistent with previous studies of smokers who undergo lung screening (Alberg et al., 2007; Piñeiro et al., 2016). These characteristics may make smoking cessation more difficult such that patients require greater assistance than what is provided by standard care four-session interventions (Hagerman et al., 2015). Indeed, some participants in this study expressed a need for more sessions or follow-up booster sessions, and the dose of the current intervention was shorter than other telehealth smoking cessation programs following lung screening that did show higher quit rates (Hagerman et al., 2015). Similarly, a review of smoking cessation interventions for adults older than 50 years also recently found relatively low quit rates and concluded that older adult smokers might require more targeted interventions (Zbikowski et al., 2012).
Studies in LDCT patients that did show higher quit rates tended to administer pharmacological treatment (Filippo et al., 2015; Pozzi et al., 2015). In this study, counselors provided information and advice about medication, encouraged medication use, and assisted participants in planning and problem-solving strategies to obtain medication over the counter (e.g. nicotine replacement therapy (NRT)) or by discussing prescription options with their primary care provider. We chose not to offer study medication in order to test a minimal intervention that would be most feasible across diverse real-world clinical settings. Our results suggest that it is important to identify feasible strategies to provide LDCT patients with access to pharmacological options.
Aspects of the study design might also account for the modest quit rate. Offering smoking cessation before LDCT has been associated with higher quit rates than offering smoking cessation after LDCT, as done in this study (Ferketich et al., 2012). This underscores the importance of reaching out to smokers as early as possible in the lung screening process—perhaps even as the lung screening decision is being made. In addition, our proactive approach might also have influenced the quit rate results by leading to the recruitment of patients with relatively low motivation to quit. Indeed, baseline levels of quit intentions in the present sample were quite low.
However, this proactive recruitment method reflects the realistic process that clinicians may need to utilize in clinical settings in order to engage lung screening patients in smoking cessation. Given that identifying optimal strategies for integrating smoking cessation into lung screening is an important area for future research (Piñeiro et al., 2016), the results of this study contribute to the literature by suggesting the feasibility of recruiting lung screening patients in clinic and delivering smoking cessation virtually over the phone. In this study, approximately half of eligible participants enrolled in the intervention, and the majority of those who enrolled completed the full intervention. These findings are similar if not slightly higher compared with enrollment and completion rates in other smoking cessation trials (Molyneux et al., 2003), highlighting the feasibility of our real-world recruitment approach. The use of a virtual intervention overcomes one of the central problems of integrating smoking cessation into lung screening, which is that there are a variety of ways patients can receive lung screening and in most cases smoking cessation counseling is not integrated into those settings. For example, although lung screening is integrated into primary care appointments, smoking cessation counseling often is not. Virtual interventions prevent patients from needing to physically visit another location for smoking cessation, which can make treatment engagement more feasible and less burdensome for patients. Future work should explore whether other telehealth venues that allow for a visual display (e.g. videophones or tablets) are effective, as they would offer face-to-face contact, which is otherwise difficult to arrange across lung screening settings.
Strengths and limitations of this study are worth noting. A primary strength noted above is that this study utilized a realistic recruitment process in a real-world setting. We used a single-arm trial design, given our primary aims to establish feasibility and acceptability (Kistin and Silverstein, 2015; Leon et al., 2011). Limitations also include the relatively small sample size, which limited the power of our statistical analyses to detect significant changes for some outcomes, and use of single-item measures for several outcomes, which can provide less robust assessments. The sample also included limited demographic diversity. Smoking status was assessed via self-report, yet it has been established that self-reported smoking status is a reliable means of assessing smoking status among participants undergoing lung screening (Parsons et al., 2010).
Overall, the current results suggest that it is possible to recruit lung screening patients for smoking cessation counseling in clinic settings and that telephone-based smoking cessation counseling programs may be a useful way to offer smoking cessation treatment to lung screening patients. Future research should explore more intensive smoking cessation interventions for lung screening patients that utilize a greater treatment dose and combine counseling with pharmacotherapy.
Supplemental Material
Figure_1.tiff – Supplemental material for Project reach: Piloting a risk-tailored smoking cessation intervention for lung screening
Supplemental material, Figure_1.tiff for Project reach: Piloting a risk-tailored smoking cessation intervention for lung screening by Inga T Lennes, Christina M Luberto, Alaina L Carr, Daniel L Hall, Nicole M Strauss, Colin Ponzani and Elyse R Park in Journal of Health Psychology
Supplemental Material
Figure_2.tiff – Supplemental material for Project reach: Piloting a risk-tailored smoking cessation intervention for lung screening
Supplemental material, Figure_2.tiff for Project reach: Piloting a risk-tailored smoking cessation intervention for lung screening by Inga T Lennes, Christina M Luberto, Alaina L Carr, Daniel L Hall, Nicole M Strauss, Colin Ponzani and Elyse R Park in Journal of Health Psychology
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work of Project REACH was supported by grants from the American Cancer Society Institutional Review Grant (ACS IRG-12–070–01) and a NCI K24 (E.R.P.).
Supplemental material
Supplemental material is available for this article online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.