
Abstract
This short-term longitudinal study examined whether adverse childhood experiences predicted attendance at a fitness program. We asked undergraduates participating in a group fitness program at a university to complete measures of mental health and adverse childhood experiences at the start of the semester. Attendance data were obtained from the recreational center at the end of the semester. Adverse childhood experiences predicted attendance after parental education and mental health were taken into account. To our knowledge, this is the first study to demonstrate that more adverse childhood experiences predict lower attendance at a health-promotion program. Findings suggest a need for adverse childhood experiences screening to prevent drop-out.
Adverse childhood experiences (ACEs), such as maltreatment and exposure to violence in the home or community, pose a significant public health problem (Larkin et al., 2014). With the publication of Felitti et al.’s (1998) well-known 1998 study, ACEs have been shown to have robust links to poor mental and physical health outcomes, such as obesity, eating disorders, ischemic heart disease, strokes, cancer, depression, anxiety, and substance abuse (Anda et al., 2006; Bellis et al., 2014, 2015; Downey et al., 2017; Felitti et al., 1998; Kendall-Tackett, 2002).
A number of health-risk behaviors (e.g. smoking, risky substance use and sexual behaviors, physical inactivity) have been suggested to mediate the relationship between ACEs and health (Bellis et al, 2014; Kendall-Tackett, 2002). However, failure to follow through with health-promotion programs has not yet been included among these, despite the fact that it was failure to follow through with such a program that sparked the idea for the original ACEs study. That is, Felitti’s (1993) research on ACEs stemmed from his observations in the 1980s that certain obese patients were dropping out of a weight control program at high rates, even though they were successfully losing weight. Upon interviewing and examining the patients’ medical records, Felitti found that many had childhood experiences of household dysfunction and maltreatment, especially sexual abuse. Combining this observation with previous references to the connection between emotional dysfunction and obesity in the medical literature, he concluded that obesity in these patients was not the problem but the solution to a deeper problem. This observation prompted him and colleagues from the Centers for Disease Control to further examine the emotionally damaging experiences associated with obesity as an underlying cause of many other disorders. It was this collaboration that led to the seminal 1998 ACEs study (Felitti, 1993, 2002, 2010).
Although Felitti’s research on ACEs was inspired by drop-outs from a health-promotion program, no researchers to our knowledge have published studies on the original question of ACEs as predictors of drop-out rates in health-promotion programs. Nevertheless, some studies have explored the predictive significance of childhood trauma for clinical interventions and have generally found that greater exposure predicts lower attendance or drop-out. For example, in two studies of children and adolescents receiving trauma-focused cognitive behavioral therapy (TF-CBT), experiencing a greater number of traumatic events was associated with less likelihood of completing treatment (Jensen et al., 2014; Wamser-Nanney and Steinzor, 2017). For adult patients, premature discontinuation of therapy was predicted by a history of childhood trauma in veterans receiving evidence-based treatments for post-traumatic stress disorder (PTSD) (Miles and Thompson, 2016) and by a history of childhood neglect in individuals receiving therapy for incest (Fletcher et al., 2017). The association between childhood trauma exposure and drop-out is not limited to patients receiving therapy for trauma. For instance, a history of emotional maltreatment in childhood predicted higher attrition in adults seeking pharmacotherapy for social anxiety disorder (Cohen et al., 2017), and a history of physical and emotional neglect in childhood increased the odds of drop-out in adults receiving pharmacotherapy for opioid use disorder (Kumar et al., 2016).
A history of early adversity predicts not only drop-out from psychotherapy but from other types of intervention as well. In a previous study, we asked undergraduate students whether they had sought any formal or informal interventions for any mental or physical disorders in the past 2 years (Karatekin, 2019). Students with more ACEs had sought more types of interventions but reported finding these forms of intervention less helpful. Furthermore, although 30 percent of students who scored above the median number of ACEs reported having stopped an intervention prematurely, only 16 percent of those who scored below the median reported the same. On the other hand, a meta-analysis of adult psychotherapy drop-out showed that a client diagnosis of trauma (included in 71 studies) was not a significant moderator of drop-out (Swift and Greenberg, 2012).
Although there is a clear need to increase attendance and adherence in health-promotion programs, research in this area has not focused on ACEs at all. Instead, studies have examined other factors, including mental health, as a predictor of attendance in these programs. A systematic review of 17 studies of predictors of attrition in lifestyle interventions (such as physical activities and dieting) showed that higher depression levels were related to greater attrition (Burgess et al., 2017). Similarly, in a Tai Chi program for older adults (Shah et al., 2015), a worse mental health score on the Short Form-36 predicted worse program attendance. However, in a review of 19 studies examining adherence to lifestyle interventions targeting weight management, higher levels of depression were related to greater attrition in four studies but showed no relationship in three studies (Leung et al., 2017). Nevertheless, given the robust relationship between ACEs and poor mental health observed by other researchers (Edwards et al., 2003) and by our group in the same student population (Karatekin & Ahluwalia, 2016), it would be reasonable to examine ACEs as a predictor of attendance.
Thus, despite some negative findings, the bulk of the evidence suggests that a history of early adversity predicts lower attendance in a variety of interventions, as well as health-risk behaviors and negative health outcomes, and that poor mental health predicts lower attendance in certain health-promotion programs. However, no study has yet examined the role of ACEs in predicting attendance in health-promotion programs. In this short-term longitudinal study, we predicted that ACEs in undergraduate students would be associated with lower attendance at a university health-promotion program. Given the evidence that better mental health predicts adherence to health-promotion programs, we examined whether ACEs predicted attendance even after controlling for initial level of mental health. If individuals with more ACEs are less likely to follow through with health-promotion programs, even after they have signed up and paid for these programs, these findings would have implications for designing targeted interventions to improve attendance and adherence to such programs and possibly clinical interventions as well.
Method
Participants
Participants were 28 undergraduates from a public Midwestern university who were enrolled in a semester-long group fitness program for the first time at the University’s Recreation and Wellness center. They were recruited using fliers posted throughout campus. Although participation was open to both males and females, all participants were female. They had a mean age of 19.9 years (SD = 2.0, range = 18–27). The majority identified as White (89%), with 11 percent identifying as Asian. In terms of year in school, 50 percent were freshman, 11 percent sophomores, 21 percent juniors, 7 percent seniors, and 11 percent other. Two participants were excluded because we were not able to obtain attendance data for them, and one participant was excluded for failing to complete all the measures at Time 2. Four additional participants completed the survey at Time 1, but not at Time 2. The study was approved by the University’s Institutional Review Board (IRB).
Group fitness program
The university group fitness program offers several dance, strength and conditioning, cardiovascular, indoor cycling, and mind/body classes on campus on a regular basis throughout the semester (http://recwell.umn.edu/wellness/group-fitness). The fitness program serves all students. Students may take part for a fee, and they are not restricted by skill level. Attendance is voluntary, the program is open to all students at the university, and students may attend any number and type of classes they wish.
Procedure
The participants filled out a set of self-report measures via a secure online survey program used by researchers at the university (Qualtrics), both at the start (Time 1) and end of the semester (Time 2). Data were collected during two semesters, between 2/2/2016 and 5/12/2016 and between 1/26/2017 and 4/23/2017. Participants averaged 70.3 days (SD = 13.4, range = 43–90) between assessments. Table 1 shows which measures were given at which time. Participants received a US$20 gift card following the completion of the second set of measures.
Descriptive statistics for the measures.
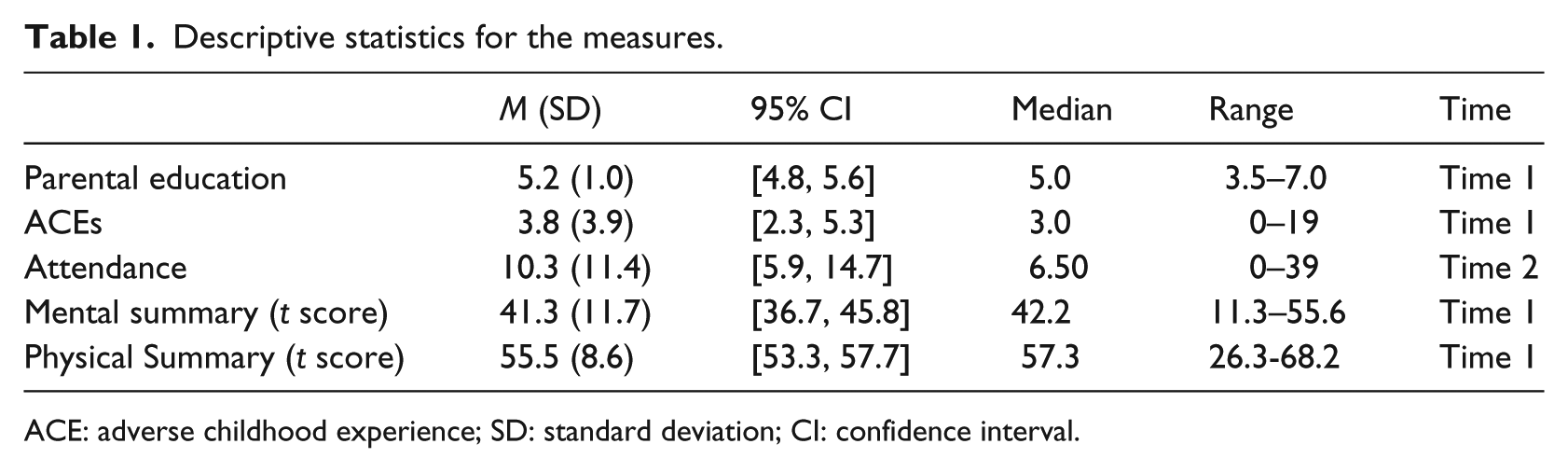
ACE: adverse childhood experience; SD: standard deviation; CI: confidence interval.
Measures
Parental education
We used parental education as a proxy for childhood socioeconomic status (SES). Participants rated the highest educational level of both their male and female primary caregivers (1 = No formal education and 7 = Completed post-college work), with the additional items of Don’t know and No primary male/female caretaker. We calculated parental education by averaging the scores of the male and female caregivers. If the participant did not know the educational level of a parent/caregiver, only the educational level of the other parent/caregiver was used.
ACEs
The questionnaire was used in three previous studies by our same research group (Karatekin, 2019; Karatekin & Ahluwalia, 2016; Karatekin, Ahluwalia, & Desir, 2018). We combined the original ACEs questionnaire (Felitti et al., 1998) with the validated Juvenile Victimization Questionnaire (JVQ) (Finkelhor et al., 2013), which included questions that went beyond maltreatment and household dysfunction. We also slightly edited the wording to be appropriate for adults. This 33-item instrument covered experiences of moderate to severe adversity between ages 0 and 18. The instructions were based on instructions for the adult retrospective version of the JVQ (http://www.unh.edu/ccrc/jvq/index_new.html): These are questions about some things that might have happened during your childhood. Your “childhood” begins when you are born and continues through age 17. It might help to take a minute and think about the different schools you attended, different places you might have lived, or different people who took care of you during your childhood. Try your best to think about your entire childhood as you answer these questions.
Participants responded to each question with a “yes” or “no”; yes responses were summed to yield an ACEs score that could range from 0 to 33. We dropped the two items inquiring about accidents and illnesses of loved ones following a subsequent exploratory factor analysis of data from 1479 undergraduates from four studies, which included the current study (Karatekin & Hill, under review). The remaining 31 items were used for all the analyses in the current study. Internal consistency, assessed by Cronbach’s α, was 0.86.
Mental health
We assessed mental and physical health with the 36-item short-form survey (SF-36; Ware et al., 1993). Mental and Physical Summary t scores were calculated from manuals provided by survey developers (Ware et al., 1993; Ware and Kosinski, 2001). Scores could range from 0 to 100, with higher scores indicating better mental health.
Attendance
Attendance information was obtained at the end of the semester (Time 2) from the Recreation and Wellness Center. Attendance was recorded for each fitness class by having attendees check into the center’s electronic system (using paper sign-in sheets if the system was not functioning). Thus, attendance refers to the number of times the student attended a fitness class.
Data analyses
Data were examined for missing values, and continuous data were checked for outliers and deviations from normality. No outliers were found. Because the distributions of ACEs and attendance were highly skewed, we transformed these variables through taking their natural logarithms. We used the transformed scores for the inferential analyses. However, for ease of comparison, we report the raw scores in the descriptive statistics.
We conducted a hierarchal linear regression to test the research question, with attendance as the dependent variable. We first conducted diagnostic checks to examine violations of normality of residuals, linearity, homoscedasticity, independence of errors, and multicollinearity. Results did not suggest a need for taking additional measures. For the first step in the regression, we entered parental education and Mental Summary scores. For the second step, we added ACEs. Given the sample size, we had 75% power to detect a large effect (f2 = .35) with two predictors and 67% power to detect a large effect with three predictors (http://www.gpower.hhu.de/). We used an analysis of variance (ANOVA) to determine whether the second step was a significantly better fit to the data than the first step. We did not use Physical Summary score as a covariate, as it was not at all related to attendance after taking parental education into account, B = .003 (SE = .04), t = .09, p = .93, β = .02. We used R (version 3.5.0; R Core Team, 2017) to analyze the data. Significance level was set at 0.05 for all analyses.
Results
Descriptive statistics
Table 1 displays descriptive statistics for the measures. Parental education scores ranged from 3.5 to 7, with a median of 5, which corresponds to graduation from college. Participants reported a median of three ACEs, with a range from 0 to 20. Attendance had a wide range, with participants attending as little as no classes or as many as 39. The mean mental summary score of 41.3 was lower than the mean score of 47.2 in the 1998 normative sample of women ages 18–34 (Ware and Kosinski, 2001), but similar to the mean score of 41.2 we obtained earlier in a larger sample from the same university (Karatekin & Ahluwalia, 2016), and the mean score of 44.7 in a sample of undergraduate students at another university (DeBerard and Masters, 2014). On the other hand, the mean Physical Summary score of 55.5 was similar to both the 1998 normative mean of 53.1 (Ware & Kosinski, 2001) and the mean score of 57.4 from a larger but comparable sample (Karatekin & Ahluwalia, 2016).
Prediction of attendance from ACEs
As can be seen in Table 2, parental education and mental health did not significantly predict attendance in Step 1 when controlling for each other. Nevertheless, the association was in the predicted direction, with lower parental education and worse mental summary scores predicting less attendance, and they accounted for 20 percent of the variance in attendance scores. The lack of significant results was likely due to the small sample size. In Step 2, ACEs significantly predicted attendance scores, after controlling for the other two variables. The standardized beta (β) for ACEs (–0.40) was fairly large and in the expected direction, with more ACEs indicating worse attendance. Step 2 explained an additional 13 percent of the variance in attendance scores. An ANOVA comparing the two steps was significant, F(24) = 5.79, p = 0.024, indicating that the addition of ACEs significantly improved the model.
Results of the hierarchical regression on attendance (N = 28).
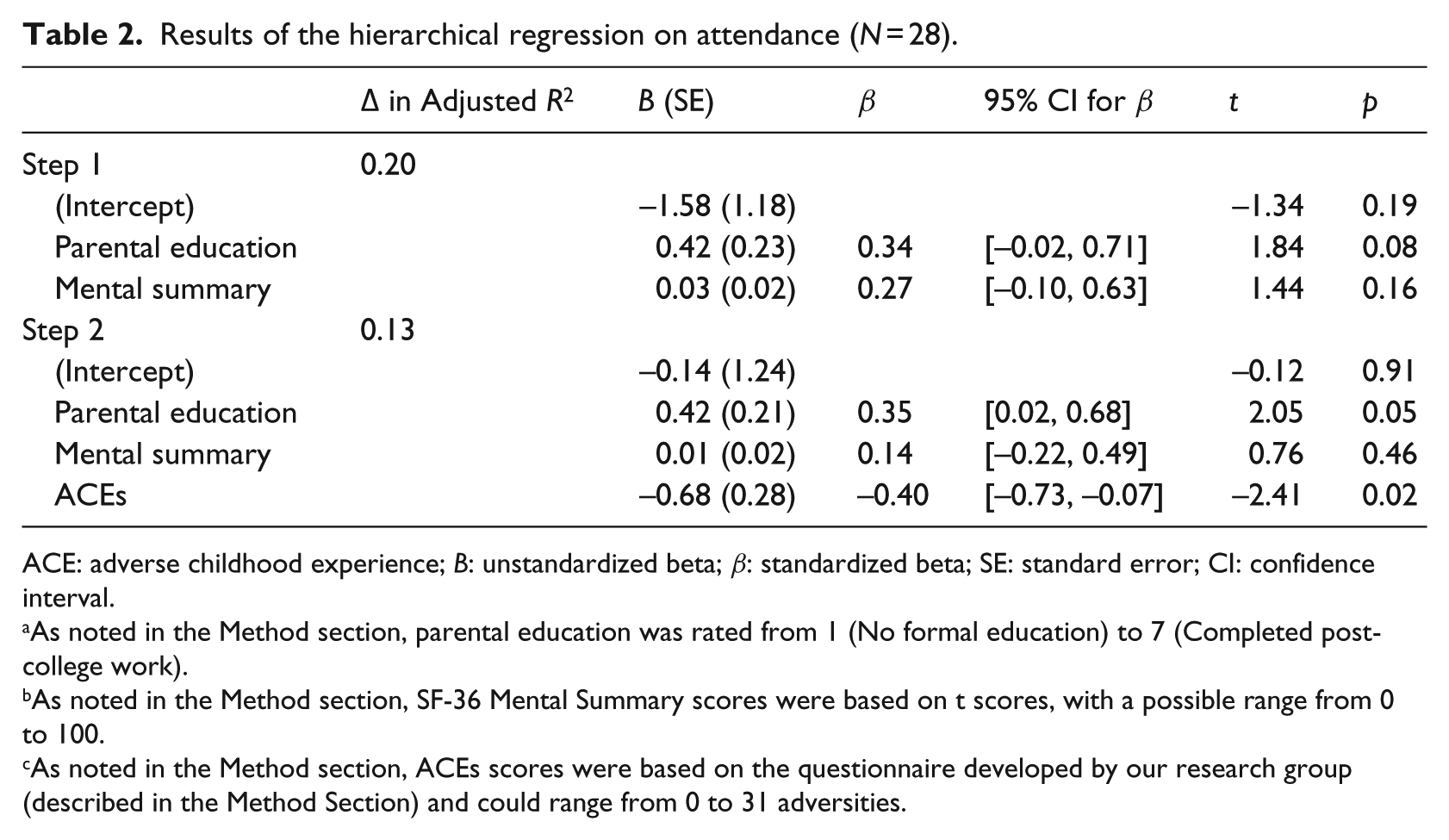
ACE: adverse childhood experience; B: unstandardized beta; β: standardized beta; SE: standard error; CI: confidence interval.
As noted in the Method section, parental education was rated from 1 (No formal education) to 7 (Completed post-college work).
As noted in the Method section, SF-36 Mental Summary scores were based on t scores, with a possible range from 0 to 100.
As noted in the Method section, ACEs scores were based on the questionnaire developed by our research group (described in the Method Section) and could range from 0 to 31 adversities.
Discussion
Summary of the results
We tested whether ACEs would predict attendance in a voluntary university group fitness program. Results of this short-term longitudinal study showed that the more ACEs students reported at the beginning of the semester, the lower their attendance was over the course of the semester, even after controlling for parental education and initial level of mental health. Furthermore, ACEs had a stronger relationship to attendance than mental health did (β = -.40 vs. .14), and this relationship reached significance despite the small sample size.
To our knowledge, this is the first study to empirically demonstrate that ACEs predict attendance at a specific health-promotion program. Our results extend Felitti’s (1993) informal observations that patients who dropped out of a weight-loss program had experienced numerous ACEs in their childhood, previous research showing that trauma history predicts lower attendance in psychotherapy (Cohen et al., 2017; Fletcher et al., 2017; Jensen et al., 2014; Kumar et al., 2016; Miles and Thompson, 2016; Wamser-Nanney and Steinzor, 2017), and studies associating poor mental health with lower attendance at health-promotion programs (Burgess et al., 2017; Shah et al., 2015).
Strengths and limitations
Besides the small sample size, limitations of the study included the lack of gender and racial/ethnic diversity in the sample. More research is needed to determine whether these results will generalize to populations beyond college students willing and able to pay for fitness classes. Although some evidence suggests ACEs may be subject to recall bias, especially for those who are currently depressed (Scott et al., 2010), other studies indicate that current symptoms do not affect the reliability of reports of child maltreatment in young adults (Pinto et al., 2014). Evidence further suggests that the relation between the number of ACEs and negative outcomes holds for both prospective (Clark et al., 2010; Scott et al., 2010) and retrospective studies (Afifi et al., 2011; Anda et al., 2008). Furthermore, test–retest reliability for the sum of the items is acceptable over intervals ranging from 6 to 20 months (Dube et al., 2004; Mersky et al., 2017; Pinto et al., 2014; Zanotti et al., 2017), and we found a test–retest reliability of 0.77 over an average of 7 weeks for the ACEs measure used in the current study (Karatekin & Hill, under review). Finally, the Recreation and Wellness Center could not include students in their attendance database if they failed to check into the system, which could have inadvertently created a lower attendance score for the student. On the other hand, a strength of the study was that we obtained attendance data from the center rather than self-report, as some studies do (Rhodes et al., 2017).
Directions for future research and implications for practice
Results contribute to research in both ACEs and in adherence to health-promotion programs by suggesting that (1) failure to follow through with health-promotion programs should be included as another potential mediator of the relationship between ACEs and poor health, and (2) ACEs should be included as another potential predictor of attendance in studies on the effectiveness of health-promotion programs.
Findings point to three additional research directions. First, more research is needed on whether findings generalize to other medical and psychological interventions. There have been a few studies showing an association between response to mental health interventions and maltreatment in particular (Garner et al., 2014; Nanni et al., 2012) or ACEs in general (Nemeroff et al., 2003; Tunnard et al., 2014). However, these studies have not examined drop-out rates as a function of ACEs. As noted in the Introduction, we found in a previous study of college students (Karatekin, 2019) that being exposed to a high number of ACEs was strongly associated with the likelihood of prematurely quitting a variety of health-related interventions. However, there are no other published studies to our knowledge that have pursued this question of the relationship between ACEs and drop-out from health-related interventions. More research is needed especially to examine the contribution of ACEs to predicting drop-out from health promotion interventions for individuals who are at risk for chronic diseases.
Second, more research is needed on the mechanisms of the association between ACEs and drop-out. It has been proposed that ACEs can lead to health-risk behaviors through psychosocial mechanisms, such as difficulties with forming and maintaining social connections (Kendall-Tackett, 2002). These difficulties with social relationships can, in turn, increase health-risk behaviors (Umberson and Montez, 2010; Yang et al., 2016). For instance, college students have been found to have a higher likelihood of health-risk behaviors, such as lack of exercise and poor diet, when they had less social support (Allgöwer et al., 2001). In a previous study of college students, we demonstrated that students with more ACEs had less perceived social support (Karatekin & Ahluwalia, 2016). Thus, individuals with more ACEs might be more likely to drop-out of interventions in the absence of a strong support network. Furthermore, in our previous study of undergraduates at the same university (Karatekin, 2019), we found that the more ACEs students reported, the less helpful they found interventions to be (including formal and informal interventions, such as outpatient psychotherapy, group activities for improving physical health, life coaching, and self-help programs). More studies are needed to further probe why this is the case and whether this perception mediates the relationship between ACEs and drop-out.
More research is also needed on moderators of the relationship between ACEs and drop-out. For example, a systematic review of predictors of adherence to lifestyle interventions for obese adults (Burgess et al., 2017) found that, in addition to better baseline mental health, early success in losing weight, lower baseline body-mass index, older age, and being male all predicted better adherence and/or attendance. Examining interactions between such baseline factors and ACEs could help identify individuals at especially high risk of attrition or non-adherence to interventions.
If further research shows that ACEs predict adherence and attendance across settings, health care providers and other professionals can use this knowledge to design screening tools and interventions to proactively minimize attrition and to optimize the effectiveness of their programs. As research by Felitti et al. (1998) makes clear, further exploring the roots of the problem of drop-out from health-promotion programs can prove useful in improving the long-term health and well-being of individuals exposed to high levels of adversity in their childhoods.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.