
Abstract
This study aims to analyze the correlations and relevance of self-efficacy items in 411 patients with diabetes using network analysis. We found that the self-efficacy items structure is consistent between genders and types of diabetes. However, the strength of item correlations was significantly higher in type 2 diabetes. The items central to the network were following a regular diet in type 2 diabetes and adjusting diet when ill in type 1 diabetes. No significant gender differences were found. Knowledge of the most central aspects of self-efficacy and their interconnections can help clinicians to target psychoeducational interventions aimed at empowering patients.
Introduction
Diabetes mellitus is a chronic condition with a high prevalence. In 2017, the International Diabetes Federation (IDF, 2017) estimated that about 425 million of people (8.8% of adults 20–79 years) have diabetes (87%–91% type 2 and 7%–12% type 1) and that 4 million people die from diabetes or its complications. The global economic cost of diabetes healthcare has been estimated as approximately US$727 billion (IDF, 2017). In 2016, in Italy, over 3.2 million people have been diagnosed with diabetes (about 90% have type 2 and 9%–10% type 1 diabetes), representing 5.3 percent of the Italian population (16.5% among people 65 years old and over) (Istat, 2017).
Once the diagnosis is established, patients with diabetes are expected to follow a complex set of self-care activities to manage their disease on a daily basis. The American Association of Diabetes Educators (AADE) specifies seven self-care behaviors to promote healthy outcomes, including healthy eating, physical activity, monitoring indicators of diabetes control (such as blood glucose and glycosylated hemoglobin), taking medication, problem-solving, and healthy coping (Coyle et al., 2013). In order to support the person with diabetes in managing these self-care activities, the American Diabetes Association (ADA) and the AADE suggested to incorporate the diabetes self-management education and support in the healthcare models (Riddle et al., 2018). These interventions should facilitate the knowledge and ability necessary for diabetes self-care and support people with diabetes in implementing and sustaining the behaviors needed to manage their chronic condition (Beck et al., 2017).
In 1960, Bandura introduced the concept of self-efficacy to define people’s confidence in their capabilities to organize and execute courses of action required to attain designated performances (Bandura, 1977). It is concerned not only with the skills one has but also with judgments of what one can do with whatever skills one possesses (Bandura and National Institute of Mental Health, 1986). According to the self-efficacy theory (Bandura, 1994; Bandura and National Institute of Mental Health, 1986), the expectations of personal mastery (efficacy expectations or self-efficacy) and success (outcome expectations) determine whether an individual will engage in one particular behavior. Self-efficacy is not of a general nature but is strictly related to specific situations and tasks (Maibach and Murphy, 1995). The ADA (Beck et al., 2017) recommends that self-efficacy should be measured to assess confidence in performing diabetes self-care activities. In fact, from a perspective of patient-centered psychosocial care in diabetes (Young-hyman et al., 2016), targeting interventions according to patient’s self-efficacy has a key role to improve diabetes self-management (Beckerle and Lavin, 2013; Iannotti et al., 2006; King et al., 2010; Nouwen et al., 2009; Sarkar et al., 2006).
Recently, the Diabetes Management Self-Efficacy Scale (DMSES), a widely used instrument first developed in the Netherlands (Van der Bijl et al., 1999) and then in a shorter 15-item version in the United Kingdom (Sturt et al., 2010), was validated in Italian in patients with type 2 diabetes (Messina et al., 2018). Exploratory factor analysis showed that this scale consists of two factors, lifestyle management and disease management. However, it is unknown whether the self-efficacy constructs measured by this scale and the correlations between items differ between type 1 and type 2 diabetes or between genders. Understanding whether specific aspects of self-efficacy are more prominent or more strongly interlinked in different patient subgroups is relevant for the design of targeted psychoeducational interventions to promote effective self-care.
In order to examine the empirical relationships among self-efficacy items in deeper detail, we used network analysis. Network modeling is a novel way of representing psychological constructs as complex dynamical systems of interacting variables. The inspection of networks allows understanding the extent to which items belonging to the same construct are connected to each other and the strength of their mutual relationships. Although in the majority of applications the analysis was typically limited to determining a network structure in a single population, recently, the focus has shifted from single population studies to studies comparing network structures from different subpopulations (Van Borkulo et al., 2015), and specific tests have been developed (Van Borkulo et al., 2016) to examine whether the network structure is identical across subpopulations, whether specific correlations differ in strength between subpopulations, and whether the overall connectivity is equal across subgroups.
It is well known that type 1 and type 2 diabetes have a different pathogenesis, age of onset, and require different therapeutic strategies for the glycemic control. Regarding gender, differences have been reported on disease management compliance with treatment and complications (Ballotari et al., 2017; McCollum et al., 2005; Maiorino et al., 2018).
Given clinical knowledge and previous evidence, we hypothesized that patients with type 1 and type 2 diabetes, as well as males and females, would feel differently capable of managing some aspects of their disease and applied network analysis to investigate the structure of the self-efficacy network in type 1 and type 2 diabetes, and in males and females stratified by type of diabetes.
Methods
Patients
Two cross-sectional surveys were conducted, in which the Italian version of the Diabetes Management Self-Efficacy Scale (IT-DMSES) was administered by trained researchers, including three of the authors (R.M., A.R., and A.U.). The first study included outpatients attending scheduled follow-up visits at the Endocrinology Unit of Sant’Orsola-Malpighi Hospital Bologna between 1 May 2017 and 31 October 2017. Inclusion criteria were age between 18 and 80 years, clinical diagnosis of type 1 or 2 diabetes for at least 6 months, and willingness to sign informed consent. Exclusion criteria were clinical diagnosis of mild cognitive impairment/dementia and clinical diagnosis of gestational or iatrogenic diabetes.
The second sample included people with type 2 diabetes recruited from the Endocrine-Metabolic Disease Module of the Internal Medicine Department of San Marino State Hospital between 1 October 2016 and 28 February 2017. Inclusion criteria were age between 18 and 80 years, being diagnosed with type 2 diabetes for at least 6 months, and willingness to sign informed consent. Exclusion criteria were dementia and gestational diabetes.
The study protocols were approved by the Ethics Committee of Sant’Orsola Hospital (currently Independent Ethics Committee of Center Emilia Area) (registration number: 31/2017/U/Oss) and the Ethics Committee of the Institute for Social Security (ISS) of San Marino (registration number: 28/2016/CERS).
All participants provided a written informed consent to participate after receiving a thorough explanation of the study procedures and having an opportunity to ask questions.
Measures
The DMSES (Sturt et al., 2010; Van der Bijl et al., 1999) measures the individual’s efficacy expectations for engaging in diabetes self-management activities, such as checking the blood sugar, maintaining healthy eating plans when away from home. Items are scored on a 0- to 10-point numerical scale, with higher scores indicating higher self-efficacy levels. The Italian validation paper carried out on the San Marino sample identified two factors, disease management (items 1, 2, 3, 6, 14, 15) and lifestyle management (items 4, 5, 7, 8, 9, 10, 11, 12, 13) (Messina et al., 2018). Detailed item description is provided in Table 1.
IT-DMSES structure, consisting of two factors (disease management and lifestyle management).

Statistical analysis
The 15 IT-DMSES items were used for the network analyses. A network is a graphical representation of the correlations between items. In this representation, items are depicted as nodes and correlations as edges. Thicker and more saturated edges denote stronger correlations. Positive correlations are represented as green edges and negative correlations as red edges. The network display is based on an algorithm (Fruchterman and Reingold, 1991) that places strongly associated nodes at the center of the network and weakly associated nodes at the periphery.
A network model including all possible correlations among items would require the estimation of a large number of parameters, including n threshold parameters for the nodes and n * (n − 1)/2 parameters for the pairwise correlations between nodes. With 15 items, this would amount to estimating 120 parameters. To deal with the problem of a relatively small data set compared to the number of parameters, we used the “least absolute shrinkage and selection operator (LASSO)” technique (Tibshirani, 1996) that leads many edge estimates to shrink to exactly zero and to drop out of the model. The LASSO returns a sparse, that is, conservative, network model in which only a relatively small number of edges are used to explain the relationships among items. Because of this sparsity, the estimated models become more interpretable. The LASSO utilizes a tuning parameter to control the degree to which the removal of small correlations is applied. We selected this tuning parameter by minimizing the Extended Bayesian Information Criterion (Chen and Chen, 2014). To take into account the skewed distribution of items, a non-paranormal transformation was applied to the data (Liu et al., 2009).
Then, to quantify the importance of each node in the network, we used the betweenness, centrality, and degree indices. The betweenness denotes the number of times a specific node acts as a bridge along the shortest path between two nodes, the closeness measures the number of direct and indirect links between one node and the others, and the degree is the strength of links with the other nodes. These indices are normalized (mean = 0 and standard deviation (SD) = 1), so that an index with a value > 1 indicates that it is >1 SD from the mean.
The network analysis was conducted using the statistical software JASP version 0.8.6 (JASP Team University of Amsterdam, 2018). The R-package NetworkComparisonTest was used to test (1) the invariant network structure, (2) the invariant edge strength, and (3) the invariant global strength between subgroups.
Results
Patient characteristics
Overall 411 patients were recruited, 246 in Bologna and 165 in San Marino.
The Bologna sample included 105 patients with type 1 diabetes and 141 patients with type 2 diabetes, while the San Marino sample included 165 patients with type 2 diabetes. Patient characteristics by type of diabetes and by gender are reported in Tables 2 and 3, respectively.
Socio-demographic and clinical characteristics of study participants (N = 411).

SD: standard deviation; BMI: body mass index.
Chi-square.
t-test.
Gender differences in type 1 and type 2 diabetes (n = 411 patients).

SD: standard deviation; BMI: body mass index.
t-test.
Chi-square test.
Patients with type 1 diabetes were younger, more frequently female, living with parents, and employed than those with type 2 diabetes. They also had lower body mass index (BMI), higher education, and a longer history of disease. Hypertension, dyslipidemia, ischemic heart disease, kidney disease, and eye damage were significantly more common in type 2 diabetes. The treatment regimen in type 2 diabetes was oral hypoglycemic mono- or pluri-therapy in 42.2 percent of patients, combination of oral hypoglycemics and insulin in 43.8 percent, and insulin alone in 10.5 percent. In type 1 diabetes, the large majority of patients were treated with insulin alone (93.3%) and 6.7 percent with insulin and oral hypoglycemics.
In type 2 diabetes, comparisons between genders revealed that males were more likely to have ischemic heart disease, dyslipidemia and kidney, neurological and peripheral circulatory complications. However, females had more frequently thyroid diseases as comorbidity. In type 1 diabetes, the only gender differences included are a poorer glycemic control and a higher frequency of thyroid disease in females.
Network analysis
Comparison between type 1 and type 2 diabetes
This analysis was carried out in the overall sample, including 306 patients with type 2 diabetes and 105 with type 1 diabetes. The network structure in type 2 and type 1 diabetes indicated that the IT-DMSES domains disease management and lifestyle management, colored, respectively, in red and blue, comprised two distinct clusters. However, the network structure, that is, the pattern of correlations among items proved to be significantly different between type 1 and 2 diabetes (M = 0.66, p < 0.001) (Figure 1).
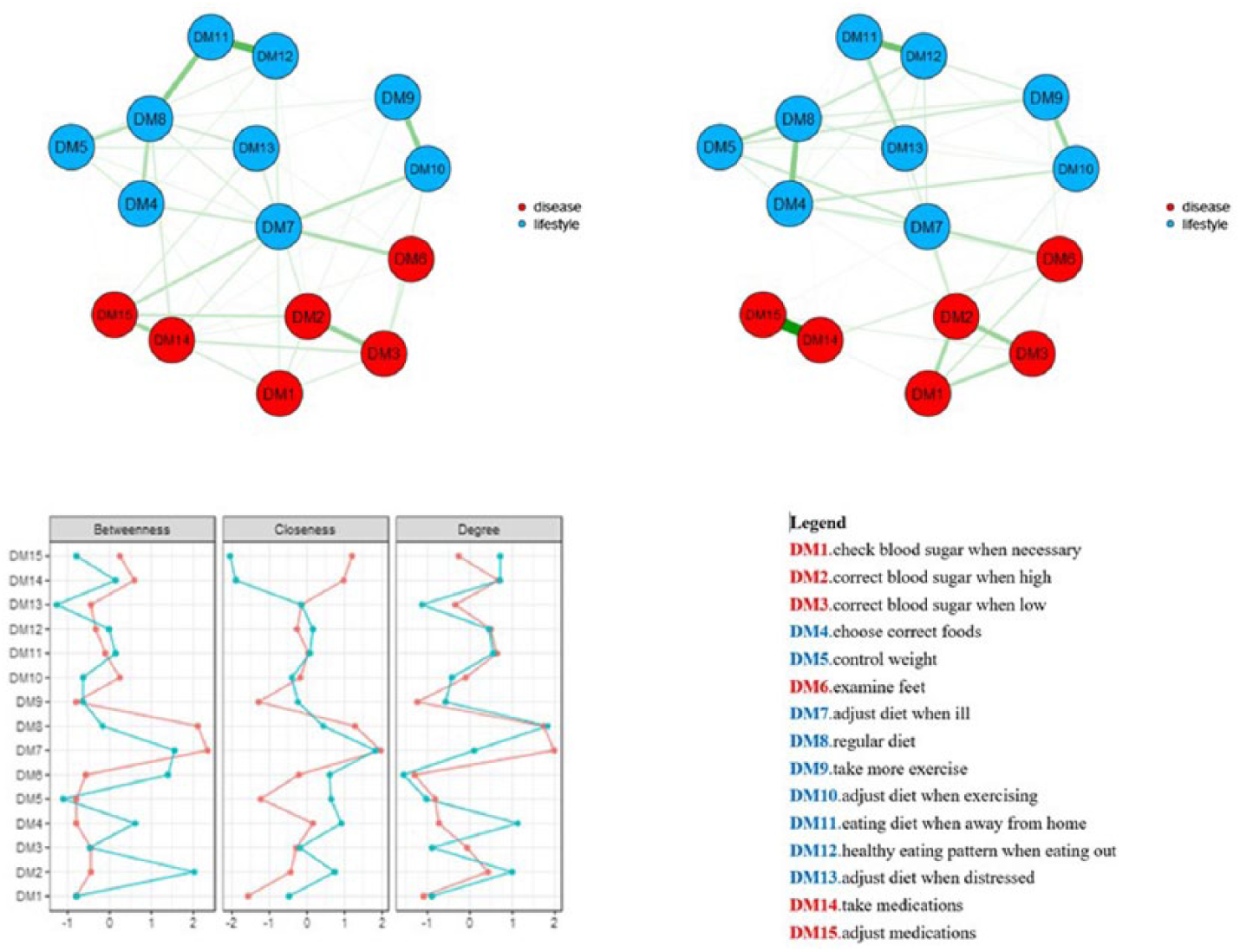
Network of self-efficacy IT-DMSES items for type 1 (on the left) and type 2 diabetes (on the right) and centrality indices (panel C: red line = type 1 diabetes; blue line = type 2 diabetes).
The global strength test revealed a significantly stronger interconnection in type 2 compared with type 1 diabetes (S = 0.77, p = 0.019). Notably, this result is accounted by the strong association in type 2 diabetes between items DM14 (take medications) and DM15 (adjust medications) that are peripheral and almost disconnected from the rest of the network. Vice versa, in type 1 diabetes, self-efficacy in lifestyle management and disease management items is more densely but weakly interconnected with each other. As expected, tests of specific edge strengths confirmed a significant difference (p < 0.001) between type 2 and type 1 diabetes for the item pair DM14 (take medications)–DM15 (adjust medications) (weight = 0.790 in type 2, weight = 0.280 in type 1) and identified additional differences for the pairs DM7 (adjust the eating plan when ill)–D10 (adjust diet when exercising) (weight = 0.224 in type 1 and 0.023 in type 2), DM8 (regular diet)–DM11 (eating diet when away from home) (weight 0.360 in type 1, weight = 0.027 in type 2), DM13 (adjust diet when distressed)–DM14 (take meds) (weight = 0.149 in type 1, weight = 0 in type 2).
Concerning the centrality of self-efficacy items, in type 2 diabetes, three items played a key role: DM2 (correct blood sugar when high) has the highest betweenness (connected directly more items with each other), DM7 (adjust diet when ill) had the highest closeness (direct and indirect connections with other items), and item DM8 (regular diet) has the highest degree (stronger links with other items). In type 1 diabetes, item DM7 (adjust diet when ill) has all the highest centrality indices.
Gender differences in type 2 diabetes
This analysis was carried out in the 192 males and 114 females with type 2 diabetes. The network structure was similar between genders (M = 0.23, p = 0.663), and the global strength was almost overlapping in males and females (S = 0.02, p = 0.953) (Figure 2).
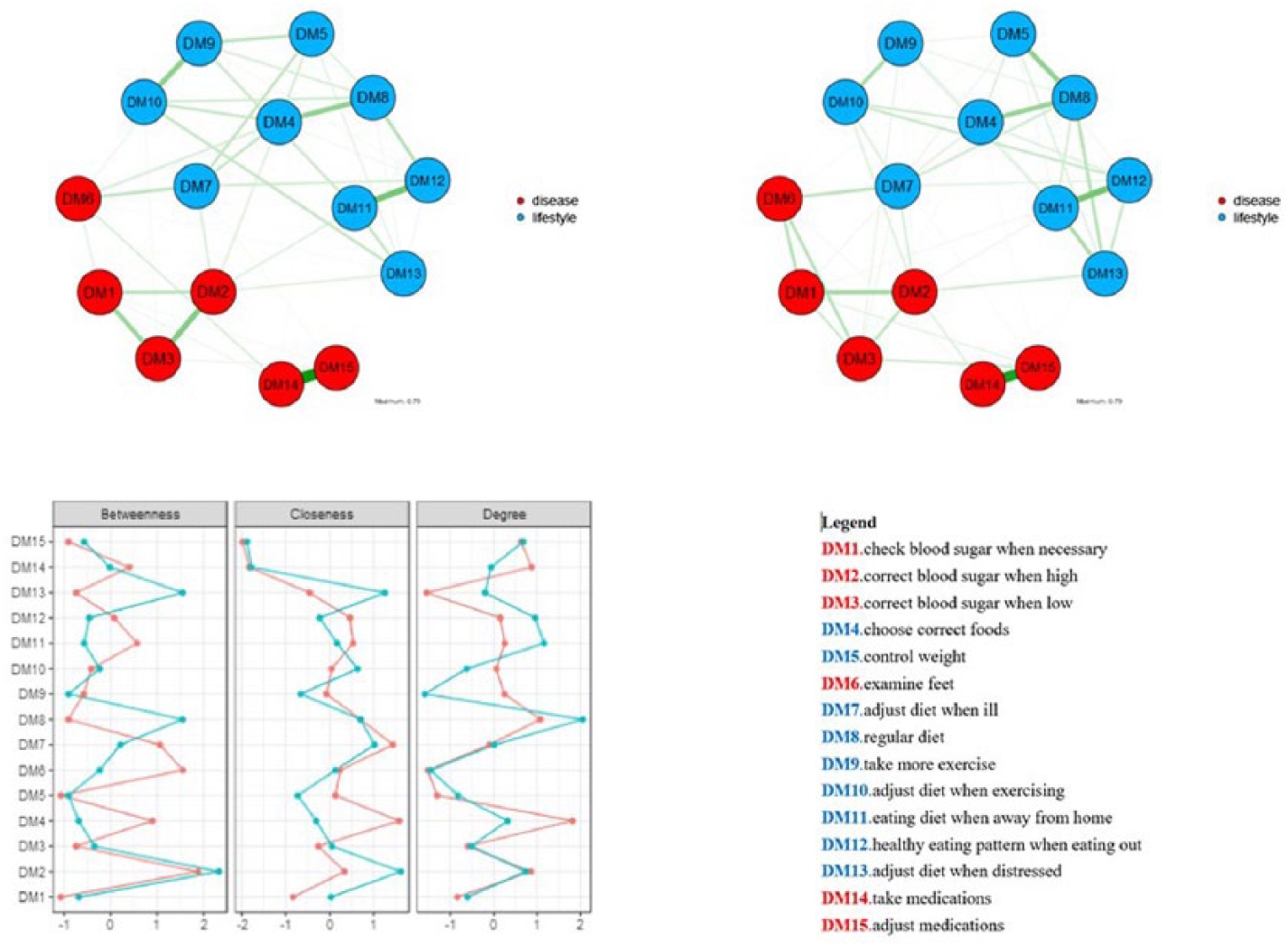
Network of self-efficacy IT-DMSES items for males (on the left) and females (on the right) in type 2 diabetes and centrality indices (blue line = females; red line = males).
Still, a visual inspection of the network showed some unique edges in males and females. While DM10 (adjust diet when exercising) was connected with DM13 (adjust diet when distressed) only in males, DM6 (examine feet) was connected with DM3 (correct blood sugar when low), DM12 (healthy eating pattern when eating out) with DM13 (adjust diet when distressed), and DM8 (regular diet) with DM13 (adjust diet when distressed) only in females.
Gender differences in type 1 diabetes
This analysis included 52 females and 53 males with type 1 diabetes. The network structure and the global strength of the correlations proved to be invariant between genders (M = 0.41, p = 0.577 and S = 0.05, p = 0.937). However, the network showed some unique edges. In males, DM7 (adjust diet when ill) was connected with DM8 (regular diet), and DM1 (check blood sugar when necessary) with DM4 (choose correct foods); in females DM8 (regular diet) was connected with DM9 (take more exercise) (Supplementary Figure 1).
Conclusion
This study is, to our knowledge, the first attempt to apply network analysis to investigate the relationships between diabetes self-efficacy items and to investigate the network structure and the strength of item relationships between type 1 and type 2 diabetes and between genders.
Our findings indicate that disease management (medication adherence, checking blood sugar levels, and examining feet) and lifestyle management (diet and physical activity) are two spatially distinct but related clusters of items, consistent across types of diabetes and genders.
The original result of this study is the difference in the self-efficacy network structure between type 1 and type 2 diabetes. The high interconnections between items in type 1 diabetes indicated that, in general, patients’ perceived ability to address specific tasks to manage their illness is associated with their ability to control their lifestyle. Thus, educational interventions aimed at empowering patients in coping with their disease are likely to affect both these aspects.
On the contrary, our findings indicate that in people with type 2 diabetes self-efficacy in taking and adjusting medications are two items strongly linked with each other but isolated and disconnected from the confidence in managing daily lifestyles. These findings suggest that an educational intervention targeted to support patients with type 2 diabetes in managing their disease may have a limited effect on the adoption of healthy lifestyles and vice versa. Thus, this study points to the need to set up psychoeducational interventions for type 2 diabetes in which the adoption of healthy lifestyles should be given at least the same attention as the glycemic control and the treatment management. Because educational programs vary in the method of delivery, content, illness, and behavior change theory, their quality and outcomes should be monitored rigorously.
The IT-DMSES provides a standardized validated tool that can be used to measure the psychosocial effects of educational programs in two ways. The first traditional way consists in analyzing changes in self-efficacy scores. Sturt et al. used the DMSES as an outcome measure in a cluster randomized trial comparing the efficacy of the Diabetes Manual versus a 6-month delayed intervention. At 26 weeks, the total DMSES score was 11.2 point higher in the intervention group compared with the control group, denoting significantly higher confidence in self-care (Sturt et al., 2008).
The second innovative way, based on a network approach, consists in analyzing the item correlations before and after the program. Stronger links among items at the end of the educational program indicate that self-efficacy is improved and that confidence in managing specific tasks is connected to confidence in managing other tasks. On the contrary, looser and weak links would suggest that self-efficacy worsened. We argue that this alternative approach would offer a deeper insight into the self-efficacy aspects that change after the intervention and is consistent with self-efficacy theory which posits that confidence in self-care is not of a general nature but related to specific situations (Bandura and National Institute of Mental Health, 1986; Van der Bijl and Shortridge-Baggett, 2001).
A recent review underscored the efficacy and cost-effectiveness of self-management education programs in promoting and facilitating self-management, which leads to improved biomedical, behavioral, and psychosocial outcomes (Chatterjee et al., 2017).
Our study has some limitations. This was a cross-sectional study measuring self-efficacy during a single study visit; therefore, we were unable to ascertain the persistence of self-efficacy in diabetes management over time.
The generalizability of these study findings beyond this patient population should be done with caution because our sample is not representative of patients with type 2 and type 1 diabetes in other settings, such as primary care. Moreover, self-efficacy was assessed using a self-report measure. Patients’ perceived ability in diabetes management may be overestimated due to a social desirability bias since patients completed questionnaires in the presence of the researcher. It is possible that the study is underpowered to detect gender differences in the subgroup of patients with type 1 diabetes that had a relatively small size. Still, this limitation is partially mitigated by the evidence of a simulation study, which reported that when a substantive proportion of edges is independent (not connected to all the other edges), the power converges to one for the tests concerning the network structure invariance and global strength (Van Borkulo et al., 2016).
To conclude, network comparisons provided an insight on the self-efficacy aspects more interlinked with each other in type 1 and 2 diabetes. Self-efficacy varies between type 1 and type 2 diabetes. In particular, self-efficacy in adjusting diet when ill plays a central role in type 1 diabetes and underscores that the ability to face non-regular self-management activities is strongly and directly interconnected with the other aspects of lifestyle and disease management. In type 2 diabetes, following a regular diet has the strongest connections with all other items. Knowledge of these aspects can give useful directions to clinicians to target psychoeducational interventions to support patient in the self-management of their condition. No significant gender differences emerged in the network structure. Future perspectives include the use of the network approach to analyze the efficacy of self-management educational programs in clinical trials and intervention studies.
Supplemental Material
Supplementary_figure_1._Network__for_males-females_in_T1DM – Supplemental material for Does self-efficacy in diabetes management differ by type of diabetes and gender? Results from network analysis
Supplemental material, Supplementary_figure_1._Network__for_males-females_in_T1DM for Does self-efficacy in diabetes management differ by type of diabetes and gender? Results from network analysis by Paola Rucci, Rossella Messina, Andrea Ubiali, Andrea Rochira, Jaap van der Bijl, Tatiana Mancini, Maria Pia Fantini and Uberto Pagotto in Journal of Health Psychology
Footnotes
Acknowledgements
R.M., A.U., and A.R. collected data and carried out the literature review; P.R. and R.M. wrote the first draft of the paper. P.R. conducted the statistical analyses. M.P.F., J.v.d.B., T.M., and U.P. contributed to the paper writing, the data interpretation, and provided intellectual content. All the authors approved the final version of the paper.
Data availability statements
The data sets generated during and/or analyzed during this study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.