
Abstract
This article explored the role of a lifetime history of gender-based violence, ambivalent sexism, and gynecological health worries in the development of reproductive and sexual symptoms among women in Kyrgyzstan. Non-pregnant women who were patients of gynecological clinics (N = 143) participated in the study. A positive relationship between the experience of any type of violence (physical, sexual, and emotional) and number of gynecological symptoms was found. Hostile sexism was found to be a predictor of the number of reported symptoms. The number of gynecological health worries was found to fully mediate the relationship between history of gender-based violence and number of gynecological symptoms.
Gender-based violence (GBV), in the forms of physical, sexual, emotional, and economic violence from male partners and other men is experienced by approximately a third of the female population of the world (World Health Organization (WHO), 2013). Experiencing GBV has been associated with an array of somatic symptoms in women, such as chronic pain, arthritis, gastrointestinal problems, and physical health complaints, as well as psychological concerns, including post-traumatic stress disorder (PTSD), anxiety, and depression (e.g. Campbell et al., 2002; McCauley et al., 2015; McNutt et al., 2002; Taft et al., 2007; Wong and Mellor, 2014). Women who have been victims of physical and sexual abuse during childhood or adulthood report higher health care utilization and health care costs (Hathaway et al., 2000; John et al., 2004; Montero et al., 2011). All forms of GBV, especially physical and sexual abuse by male partners and others, has also been found to relate to gynecological symptoms (e.g. Cambron et al., 2002, 2014; Coker et al., 2000, 2009; Golding et al., 2000; Leithner et al., 2009).
With regard to gynecological symptoms, women with a history of GBV report abdominal pain, pain during menstruation, irregular menstrual cycle, chronic pelvic pain, pain during intercourse, infertility, and unspecified symptoms associated with their genital organs, to a greater degree than women with no histories of violence (John et al., 2004; Leithner et al., 2009; Letourneau et al., 1999; Mark et al., 2008). In addition to a history of physical and sexual violence, a history of psychological or emotional violence has been found to be strongly associated with the development of gynecological symptoms (Coker et al., 2000; Johnson et al., 2007). Women who have experienced multiple types of violence (i.e. physical, sexual, and/or psychological) report a higher number of gynecological symptoms (e.g. John et al., 2004), suggesting a possible additive effect of different types of gendered violence. Finally, independent of the type of violence experienced (physical, sexual, or emotional), the number of gynecological symptoms increases with the frequency of exposure to violence within a given time period (Golding et al., 1998). The duration of the period of abuse (Coker et al., 2000; Golding, 1996) and the recency of the exposure to violence (Eberhard-Gran et al., 2007) also seem to influence the increase in gynecological symptoms reported.
Although this link between the experience of violence and the number of gynecological symptoms in women has been fairly consistent, little is known about what factors might relate to increased symptoms in women survivors. Anxiety about one’s health has been given some attention as a potential outcome of the experience of violence, in particular, GBV (Campbell et al., 2002; John et al., 2004). Health anxiety is defined as persistent worries about one’s general health, excessive attention to somatic symptoms, and worry about having an undiagnosed medical condition (Barsky, 2001; Stein et al., 2004; Walker et al., 2007). Although research that directly studies health anxiety in relation to a history of violence is scarce, some studies associate past experience of violence with more health worries. Specifically, a history of sexual assault was found to predict health anxiety and somatization in women in the military, and the number of health worries was moderately correlated with the number of bodily symptoms women reported (Stein et al., 2004). With respect to gynecological symptoms in particular, John et al. (2004) found that women who reported a history of domestic violence also reported a greater predisposition of worries about gynecological cancer in comparison with women who reported no history of violence.
In addition to health worries, the present study explored the women’s ambivalent sexism (AS) (Glick and Fiske, 1996) as a possible factor that may increase the gynecological symptom development. AS is defined as holding both hostile and benevolent sexist attitudes toward women and AS has been found to correlate with women’s greater acceptance of violence against women in the forms of domestic violence and rape myths (Chapleau et al., 2007; Glick et al., 2002; Lila et al., 2013; Koepke et al., 2014; Marques-Fagundes et al., 2015; Yamawaki, 2007), including in international samples (Expósito et al., 2010; Glick et al., 2002; Marques-Fagundes et al., 2015; Yamawaki, Ostenson and Brown, 2009). It is thought that women who have been victims of GBV may place more blame on women for their experiences of GBV in an effort to explain the violence and offer themselves a sense of control and self-protection, and therefore, have more negative and hostile attitudes toward women in general. Based on the above studies, we suggested that hostile sexism may play a role in symptom development in women with a history of GBV due to women survivors’ accepting attitudes toward violence against women. We suggest that the discrepancy between experiencing GBV and endorsing hostile sexism might result in greater distress and somatic manifestations of distress.
The present study explores the association between the experience of GBV and the development of reproductive and sexual symptoms in women in Kyrgyzstan. Previous research has found an incidence rate of 83 percent for domestic violence reported among women in Kyrgyzstan, with a high prevalence of the practice of bride kidnapping, a particular form of violence against women in parts of Central Asia, as well as strong endorsement of attitudes toward violence against women reported by both women and men (Association of Crisis Centers for Women, 2009). Nevertheless, the majority of research to date on the development of somatic symptoms in response to GBV comes from Western countries. In relationship to women’s rights, Kyrgyzstan is a country with diverse and changing attitudes toward women’s rights (Association of Crisis Centers for Women, 2009). The diversity of attitudes toward women and GBV is partially explained by the fact that Kyrgyzstan is a Central Asian post-communist country with a rich and complicated social, political, cultural, and religious history that is still undergoing a sociopolitical transition from Soviet-style communism to an independent country with a democratic government. Due to these influences, there is a diversity of attitudes toward women’s roles in society, including tolerant attitudes toward violence against women. Research suggests that due to these attitudes toward violence against women, there is a high potential that women in Kyrgyzstan may become victims of any form of violence (Molchanova et al., 2013). This study thus aims to explore the relationships among GBV, health worries, and AS in a sample of women seeking medical care.
Based on the suggested aim, the following hypotheses guided this study:
Women who report a history of GBV during adulthood will report a significantly greater number of gynecological symptoms in comparison with women who do not report any recent history of violence;
Each type of violence (sexual, physical, and emotional) measured independently will be associated with an increase in gynecological symptoms in women;
Women who endorse greater ambivalent sexist attitudes (both benevolent and hostile) will report a greater number of gynecological symptoms in the presence of a history of GBV during adulthood;
Gynecological health worries will mediate the relationship between history of violence and the number of symptoms. We hypothesized that experience of GBV would result in greater health worries, which would in turn influence the increase in somatic symptoms.
Method
Participants
Participants in this study were 143 women (ages 18–55, M = 32; SD = 8.9) who were not pregnant and were in treatment for gynecological symptoms in five obstetric-gynecological clinics in Kyrgyzstan. The authors aimed to recruit at least 80 participants to ensure that further analyses are powered enough given the number of independent variables (4) and possibility of drop out. In terms of ethnicity, 78 respondents self-identified as Kyrgyz (54.5%), 46 as Russian (32.2%), and the rest as other. All participants of this study were citizens and residents of Kyrgyzstan. A total pf 82 questionnaires (57.3%) were filled out in Russian and 61 (42.7%) in Kyrgyz. The majority of participants were married (n = 75; 52.4%), employed (n = 86; 60.1%), and reported a high school degree or higher (98%). More than half of the participants reported having at least one child (67.8%). A total of 15 participants (10.5%) described themselves as not religious, 66 as somewhat religious (46.2%), 56 (39.2%) as religious, and 6 (4.2%) as very religious.
Measures
Reproductive and sexual symptoms questionnaire
A questionnaire to measure the presence of gynecological and/or sexual symptoms was developed specifically for this study. The existing similar checklists were deemed inapplicable to the aims of this study because they are measuring a larger list of symptoms and do not focus on gynecological ones. The questionnaire consisted of two sections. Section 1 consisted of 11 “yes” or “no” questions that asked the participant to mark the symptoms and sensations that she had experienced during the previous year, as well as diagnoses that she had received during this period. Sample items included “pain in your abdomen,” “missing two or more periods,” “unusually heavy menstrual bleeding,” “unusually severe pain during menses,” “vaginal infection,” “abnormal pap smear,” “gynecological cancer,” “infertility,” “ovarian cyst,” “endometriosis,” “premenstrual syndrome (PMS),” and other. Section 2 asked participants to rate on a Likert-type scale (0—“never,” 1—“seldom,” 2—“sometimes,” 3—“often,” 4—“all the time”) how often they experienced the following three sexual symptoms during the past year: “pain during sexual intercourse,” “lack of libido,” and “inability to reach orgasm (vaginal or clitoral).” Each sexual symptom in section 2 was coded as present if the participants replied that they experienced it “sometimes” or more during the past year. The sections 1 and 2 were scored together by combining the number of gynecological symptoms and sexual symptoms, which yielded a score from 0 to 14 (see Table 1).
Means, Standard Deviations, and Pearson correlations among the key variables of interest (N = 143).
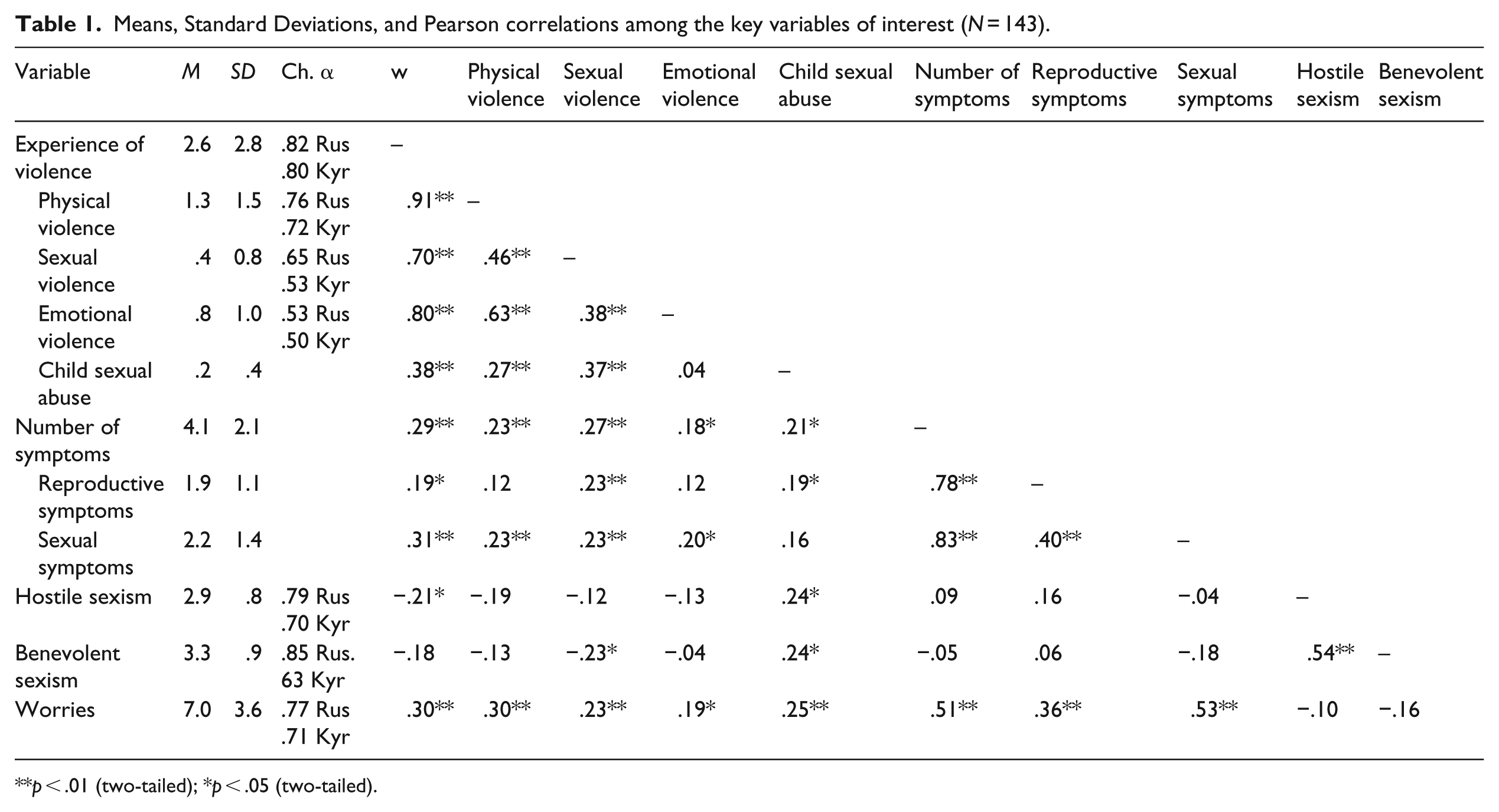
p < .01 (two-tailed); *p < .05 (two-tailed).
Gynecological worries questionnaire
A self-report questionnaire measuring women’s subjective worries around sexual and reproductive health was developed for this study. The existing similar checklists were deemed inapplicable to the aims of this study because they are measuring a larger list of symptoms and do not focus on gynecological ones. The questionnaire consisted of 15 items and asked participants to rate their concerns about their reproductive and sexual health during the past year (e.g. “How often during the last year have you been worried about the following thoughts: Whether you would be able to get pregnant; whether you might have an sexually transmitted disease (STD); whether your vaginal discharge is abnormal,” etc.). Each statement was scored on a Likert-type scale with the following ratings: “0 = never,” “1 = rarely,” “2 = sometimes,” “3 = often” and “4 = all the time.” The scores for this questionnaire were scored by adding up the scores for all items, which yielded a score from 0 to 60 (Table 1).
WHO’s Violence Against Women Instrument
The Violence Against Women Inventory (VAWI) was used to measure the extent to which women experienced GBV of any type during their lifetime (Nybergh et al., 2013; WHO, 2005). The VAWI consists of 13 items originally measuring various aspects of intimate partner violence that are grouped in three sections: psychological, physical, and sexual violence against women. The original instrument was found to have high internal validity (the internal consistency ranged from Cronbach’s alpha of .72 to .80 for different types of violence). In the present study, the VAWI was used with slight modifications with permission of WHO (2016), specifically, the respondents were asked to answer the inventory questions in application to partner as well as non-partner violence. The range of violence experience (including witnessing violence) was measured by adding up all “yes” answers to any of the items, which yielded a score from 0 to 14 (Table 1). Also, the extent of the experience of each type of violence was scored separately: the experience of physical violence was a score from 0 to 6, the experience of sexual violence as a score from 0 to 3, and experience of psychological violence on a range from 0 to 4. The measure was amended with a single dichotomous question on whether participants reported child sexual abuse and a single dichotomous question on the experience of witnessing violence in the family as a child.
AS inventory
The Ambivalent Sexism Inventory (ASI) was used to measure the attitudes and expressions of internalized sexist beliefs. The ASI (Glick and Fiske, 1996, 2001) is a 22-item self-report questionnaire, consisting of 11 items measuring hostile sexism, and 11 items measuring benevolent sexism. Every item is answered using a Likert-type scale from 0 (disagree strongly) to 5 (agree strongly). The authors reported .85 for the Adjusted Goodness of Fit Index (AGFI) and Alpha Reliability Coefficients from .83 to .92 across six different studies. The correlations between the original hostile and benevolent sexism scales are reported to be at least .71. The ASI has been used cross-culturally in at least 19 countries, and the cross-cultural reliability has been found to be high (Glick and Fiske, 2001). The measures of internal consistency are described in Table 1.
Translation
All the materials described above were translated into Kyrgyz and Russian languages using the procedure of double translation (Sousa and Rojjanasrirat, 2011). The translation team consisted of the primary investigator and five independent bilingual translators who were graduate students in psychology. Two translators translated the inventory into Russian and Kyrgyz, then a judge proficient in Russian and Kyrgyz checked the two translated versions for discrepancies and made decisions about the final translation. The same procedure was conducted to translate the Russian and Kyrgyz versions back into English by different translators and a judge. The primary investigator compared the translations and the original and communicated with the judges in the two cases of discrepancies until those were eliminated.
Procedure
Participants were recruited in the waiting areas of gynecological clinics by three local research assistants trained in research methods in psychology and research ethics. The assistants were proficient in both Kyrgyz and Russian languages. The permission of the Department of Health of Bishkek, Kyrgyzstan, was obtained prior to the beginning of the study and the study went through Human Subject Review at the first author’s university at the time of the study. Doctors were provided with envelopes that contained informed consent forms and all the questionnaires. The patients filled out the questionnaires in the doctor’s office. Doctors were instructed to pass the envelopes with a description of the study to interested patients but to not assist. Research assistants were present in the clinic throughout the procedure. An honorarium of $7 was offered for participation in the study. This sum of money was considered appropriate for Kyrgyzstan for a half-an-hour survey.
Design and analysis
A correlation analysis was conducted to explore the relationships among the variables of lifetime experience of violence and total number of symptoms. A number of t-tests were conducted to explore if different types of violence (sexual, physical, and emotional) predicted gynecological symptoms in women. A series of multiple regressions were run to test the impact of AS on the total number of symptoms. This study hypothesized that the relationship between experience of violence and reported symptoms would be stronger for women who scored higher on hostile and benevolent sexism. Finally, a multiple regression was used to test the mediation model exploring number of worries as a mediator of the relationship between violence and symptoms. The mediation analysis was conducted using the method described in the study by Frazier et al. (2004).
Results
Preliminary analyses
The prevalence of lifetime violence (during childhood or adulthood, including witnessing violence in one’s family of origin) in the overall sample was found to be 94 percent. The prevalence of violence in the Kyrgyz language sample was found to be 89 percent, and in the Russian language sample, 99 percent. A total of 50 participants (35%) reported never experiencing any type of violence during adulthood. There were no significant differences found in the number of worries and symptoms reported between the two language groups (t(140) = −.167; p = .868).
The relationship between experience of violence and symptoms
The results revealed a small positive correlation (r = .28, p < .01) between the experiences of violence during a woman’s lifetime and the total number of gynecological symptoms within the past year, as well as a significant relationship between all types of violence and gynecological symptoms. Finally, there was a relationship between lifetime experience of violence, including child sexual abuse, with reproductive symptoms (Table 1). The effect sizes for the correlations between the key variables of interest varied from small (r = −.21) for correlation between hostile sexism and history of violence to large (r = .53) for correlation between worries and number of sexual symptoms, and were mostly medium.
The results of a t-test analysis revealed that women who reported lifetime violence also reported more total symptoms (M = 4.52, SD = 2.1) in comparison with women who reported no experience of violence (M = 3.15, SD = 1.8, t(143) = −3.82, p < .01) (see Table 2). Also, the number of both reproductive and sexual symptoms differed between the two groups of participants.
Differences in means and standard deviations between women who experienced violence and those who did not.

p < .01 (two-tailed).
Testing AS as a predictor of the number of symptoms
For studies of AS in relationship to violence, the two constructs of hostile and benevolent sexism are explored separately (Glick and Fiske, 1996). All further analyses in this study were conducted using the measure of violence during adulthood, and did not include abuse during childhood or witnessing violence. A three-stage hierarchical multiple regression was conducted with number of gynecological symptoms as the dependent variable. Prior to conducing a hierarchical multiple regression, the relevant assumptions for this statistical analysis were tested and necessary data transformations were made. Number of worries was entered at stage 1 of the regression as a control variable, as it has been found by prior research to be one of the outcomes of GBV and to be strongly associated with the number of reported symptoms (Barsky, 2001; Campbell et al., 2006; John et al., 2004; Walker et al., 2007; Plichta and Fdalik, 2001; Stein et al., 2004). The responses of only 95 respondents were analyzed at this stage, due to including only women who experienced violence and a reduction in the return of questionnaires with completed measures of AS.
Adulthood GBV and hostile sexism variables were entered at stage 2 as predictor variables. Finally, the product term of violence and hostile sexism was entered into the regression at stage 3. The results of this regression are summarized in Table 3. In the first step, the number of worries reported for the previous year accounted for a significant amount of variance in the total number of gynecological symptoms (R2 = .33, F(92, 1) = 45.949; t = 6.799; p < .001). In the second step, the past experience of violence and hostile sexism were found to explain a significant additional amount of variance in the total number of symptoms (R2 = .41, ∆R2 = .07, F(90, 3) = 20.525; t = 2.809(violence); t = 2.245(hostile sexism); p < .001). However, the interaction term was not found to account for any additional amount of variance in the total number of symptoms, suggesting that hostile sexism did not moderate the relationship between GBV and number of symptoms. Post hoc power analysis was conducted using SPSS program and the observed power to detect reported effect size (Table 3) for the model 1 with worries as predictor was determined to be 1.000, the observed power to detect reported effect sizes for the model 2 were .837 for the general model, .463 for violence, and .737 for hostile sexism.
Summary of hierarchical regression analysis exploring experience of violence during adulthood and hostile sexism predicting the number of gynecological symptoms.
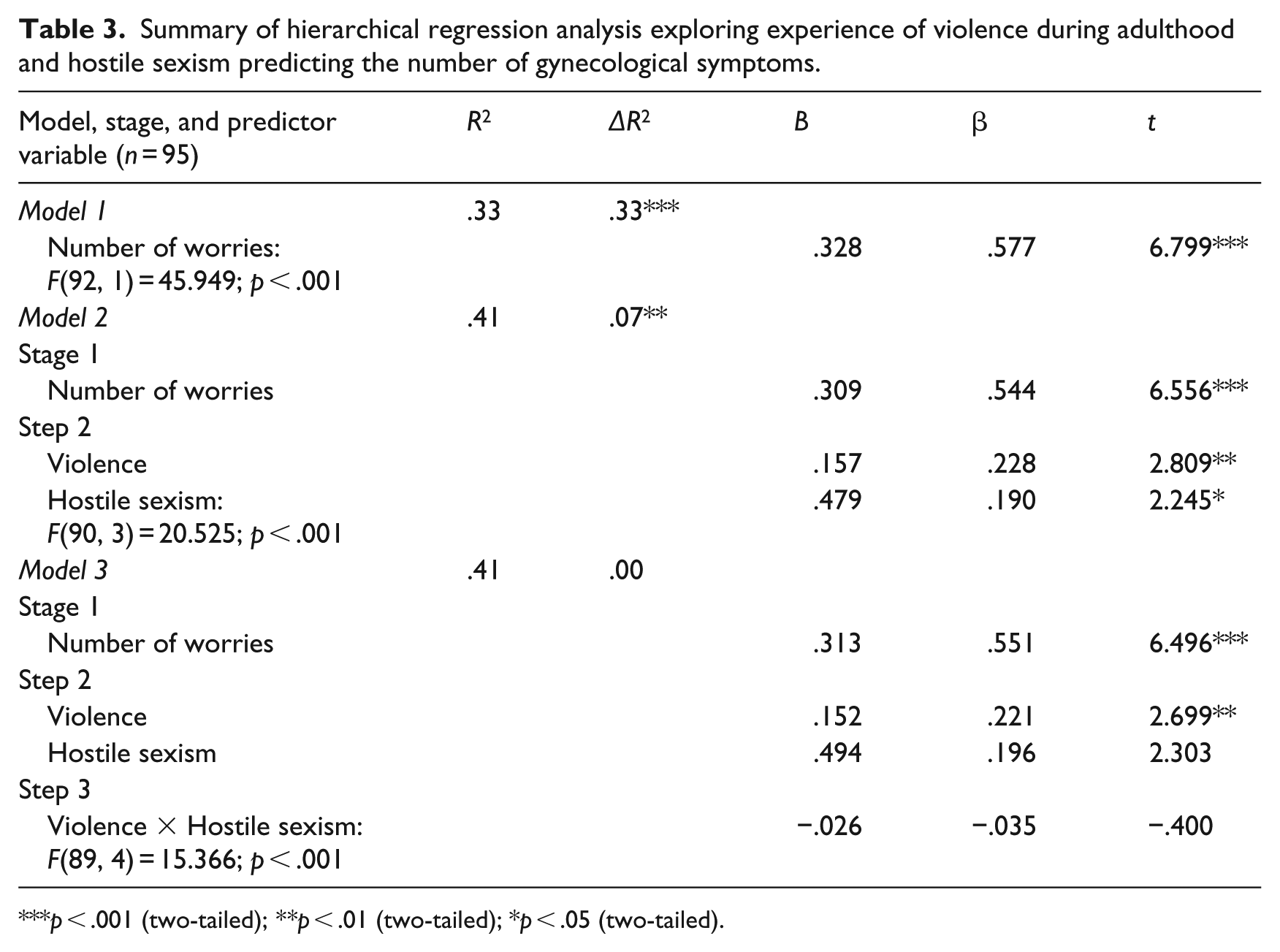
p < .001 (two-tailed); **p < .01 (two-tailed); *p < .05 (two-tailed).
Benevolent sexism was not found to be a significant unique predictor of the number of gynecological symptoms, and thus was not included in subsequent analyses.
Testing the number of health worries as a mediator of the relationship between violence and symptoms
A mediation analysis was conducted to explore the role of reproductive and sexual health worries in the development of symptoms in women who reported an adulthood history of GBV (see Table 4). At the first step, the relationship between violence and symptoms was found (R2 = .08, F(141, 1) = 12.585; t = 3.547; p < .001). At the second step, the relationship between violence and number of worries was established (R2 = .09, F(140,1) = 13.466; t = 3.670; p < .001). Finally, at the third step, it was found that in the presence of the number of worries the relationship between violence and symptoms becomes insignificant (R2 = .28, F(139, 2) = 27.452; t(worries) = 6.259; p < .001; t(violence) = 1.934; p = .055). Post hoc power analysis was conducted using SPSS program and the following power values were observed: .994 for the general model, .742 for violence, and .997 for worries.
Summary of multiple regression analysis exploring the number of gynecological health worries mediating the relationship between experience of violence and number of symptoms.
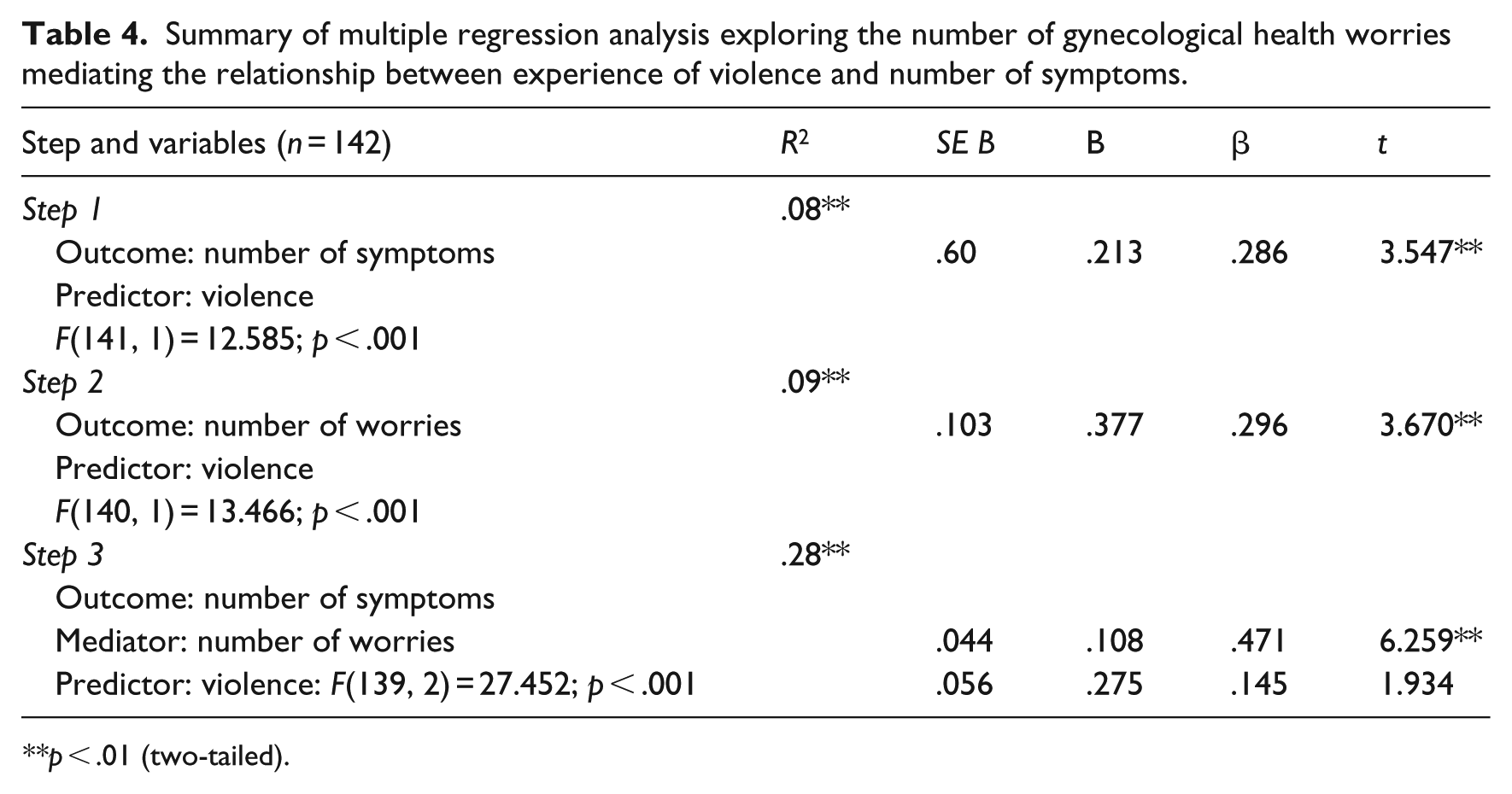
p < .01 (two-tailed).
The significance of the mediation model was tested using the method by Kenny et al., 1998; the mediated effect of number of worries was considered significant. The number of health worries was found to fully mediate the relationship between violence and symptoms. Figure 1 demonstrates the mediation model that was tested. The alternative mediation model with number of symptoms mediating the relationship between violence and worries was also tested but symptoms were not found to mediate the relationship (R2 = .29, F(139, 2) = 28.157; t(symptoms) = 6.259; p < .001; t(violence) = 2,186; p = .031).
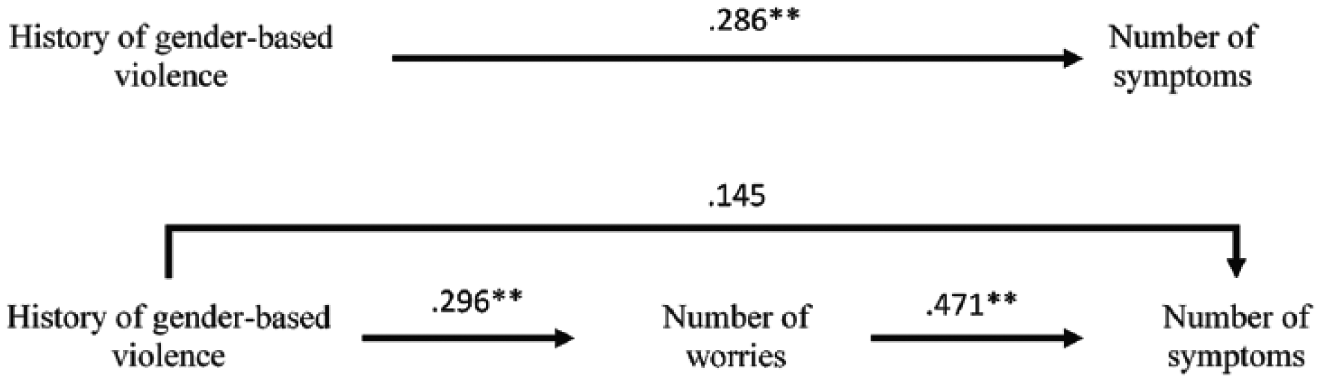
The mediation model explaining the role of reproductive and sexual health worries in the relationship between violence and symptoms.
Discussion
This study supported the results of global research suggesting a strong link between any experience of GBV and both reproductive and sexual symptoms in women. The present study adds to the international research on violence against women, as the majority of the literature on this subject comes from the United States and Europe. There are few studies on this topic to our knowledge that were conducted in Asia with the exception of Agrawal et al. (1996) and Salam et al., 2006, both of which found a difference in symptoms reported by women who had experienced violence versus women who had not.
The rates of violence found in our sample (57% for the experience of physical violence, 25% for sexual, and 47% for emotional) are generally similar to the rates of violence reported in other studies, which range from 21% to 66% for physical violence (Cambron et al., 2014; John et al., 2004; Wijma et al., 2000), from 13% to 33% for sexual violence (Cambron et al., 2014; Leithner et al., 2009; Mark et al., 2008; Wijma et al., 2000), and around 23%–54% for emotional or psychological violence (Cambron et al., 2014; Johnson et al., 2007; Leithner et al., 2009).
The present study supported findings of previous global research suggesting a link between gendered violence and health worries. The number of worries was found to correlate with a history of violence (r = .30; p < .01). Our research expands upon previous findings (Barsky, 2001; Campbell et al., 2006; John et al., 2004; Plichta and Falik, 2001; Stein et al., 2004; Walker et al., 2007); our data suggest that gynecological health worries mediate the relationship between violence and gynecological symptoms. This means that the previous well-researched link between violence and symptoms may be explained to some extent by the elevated health worries in women-survivors of abuse.
Contrary to what was hypothesized, hostile and benevolent sexism were not found to mediate the relationship between violence and symptoms in this study. However, hostile sexism was found to explain some variance in the number of symptoms (up to 7%), after controlling for the contribution of health worries. In the context of the present study, this finding suggests a negative relationship between internalized negative stereotypes of femininity and a history of violence. Specifically, women who reported greater experience of GBV during adulthood also reported less negative attitudes toward women, which is in contrast to other research findings.
Limitations
This study focused on the study of gynecological symptoms in women, and avoided measuring other types of somatic symptoms. However, the established relationship between violence and symptoms might be not fully explored due to lack of information on the total number of all somatic symptoms in respondents. Also, although the respondents were recruited in gynecological clinics, the list of symptoms in our study was based on self-report and was not confirmed by official diagnosis. Finally, there is a possibility of selection bias due to recruiting participants seeking medical services at the moment and thus probably experiencing higher number of health worries than women from the general population.
Conclusion and implications
There is a strong relationship between a history of GBV and the development of reproductive and sexual symptoms in women in Kyrgyzstan. Women who reported a history of violence also experienced more gynecological health worries. Reproductive and sexual health worries explained the relationship between violence and symptoms, suggesting that gendered violence may result in a higher number of worries in women, which then may contribute to the development of actual gynecological symptoms. Also, women who experienced a greater number of different types of violence tended to have less hostile sexist attitudes toward women, according to our research. Furthermore, research is needed to explore this relationship, given it contrasts with the majority of research on hostile sexism and violence.
Knowledge of the mechanisms of gynecological symptoms development might provide important insights into planning of health care and providing psychological services to women. Our research revealed that GBV plays an important role in the development of health anxiety and somatic symptoms in women. A specific implication of our study is highlighting the importance of addressing women’s health worries, especially around reproductive and sexual health, and the importance of screening for violence histories in women-patients of gynecological clinics, both those presenting with diagnosable symptoms as well as general worries about their reproductive and sexual health. Such practices could enhance interventions of timely and multifaceted medical and psychological interventions for women-survivors of GBV. The results of this study also provide some data to inform the process of elimination of violence against women in the country by highlighting the medical consequences of abuse and the role of internalized sexism in symptoms development for women-survivors and for the general public.
The present study did not explore the preventive factors and resilience in women-survivors of violence. Furthermore, research might focus more on the factors preventing women from the development of symptoms and worries even in the presence of violence. In conclusion, this study, the first of its kind in Central Asia, identified the strong association between GBV and health-related worries and reported symptoms of gynecological concerns among women seeking services. These findings could be used to inform prevention and intervention practices in medical contexts, and to increase awareness of the ongoing serious effects of GBV.
Supplemental Material
Supplemental_Material – Supplemental material for The role of gender-based violence, health worries, and ambivalent sexism in the development of women’s gynecological symptoms
Supplemental material, Supplemental_Material for The role of gender-based violence, health worries, and ambivalent sexism in the development of women’s gynecological symptoms by Elena Kosterina, Sharon G Horne and Sharon Lamb in Journal of Health Psychology
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.