
Abstract
Polycystic ovary syndrome is the most common endocrine disorder among women aged from 18 to 40 years. Its debilitating menstrual/obesity-related symptoms challenge conceptions of femininity. To date, age-related differences in women’s body esteem and physicians’ symptom management recommendations have not been investigated. Age moderated the relationships between symptom concerns and both sexual attractiveness and physical condition, but only for midlife, not for emerging adult women. Midlife women received holistic management information from physicians, while emerging adult women received weight management information. This study highlights the need for physician training to manage women’s health and age-targeted body acceptance interventions for women diagnosed with polycystic ovary syndrome.
Keywords
Polycystic ovary syndrome (PCOS) is the most common hormonal disorder in reproductive-aged women, affecting one in every five women, with prevalence rates ranging from 10 to 25 percent of women worldwide (Azziz et al., 2004; March et al., 2010; Sirmans and Pate, 2013). PCOS is characterized by a hormonal imbalance in estrogen and testosterone, which not only disrupts the menstrual cycle and fertility, but also leads to an increase in insulin resistance (Sirmans and Pate, 2013). Because the metabolic system is not using insulin appropriately, the body begins to produce more testosterone to block insulin production. This creates a negative feedback loop, leading to rapid weight gain, resistance to weight loss via caloric restriction and/or aerobic exercise, menstrual irregularities, increases in masculine secondary sexual characteristics, such as male-pattern baldness and excess hair growth (i.e. hirsutism), and acne (Benson et al., 2008; Talbott et al., 2007). Women diagnosed with PCOS are also at an increased risk for obesity-related disorders (e.g. type II diabetes, cancer, cardiovascular disease; Benson et al. (2008)) and reproductive problems (e.g. endometrial cancer, infertility; Azziz et al. (2004)). Along with the pervasive physical health complications, many women with PCOS also suffer from the added negative impacts to their mental health and well-being. Specifically, they may struggle with higher depression, anxiety, body dissatisfaction, disordered eating patterns (e.g. bulimia, binge-eating behaviors), and lower subjective quality of life than women without PCOS (Ching et al., 2007; Deeks et al., 2010).
Given the debilitating nature of the host of symptoms associated with this disorder, it is not surprising that, for women diagnosed with PCOS, their conceptions of their body esteem may be affected. Not only do many women diagnosed with PCOS suffer with perceptions of abnormality and difference from other women (Kitzinger and Willmott, 2002), but also experience higher dissatisfaction with their bodies (Himelein and Thatcher, 2006) and reduced sexual desire and arousal (Bazarganipour et al., 2013). This is particularly the case with more clearly visible symptoms, particularly weight gain and difficulty in losing weight (Himelein and Thatcher, 2006). The symptoms associated with PCOS affect women’s experiences with their bodies, in terms of structure (i.e. appearance), function (i.e. sexual functioning, physical ability), and challenge (the symptoms associated with PCOS challenge conceptions of femininity; Bazarganipour et al. (2013)).
Women become socialized to be hyperfocused on their appearance as a defining feature of their identity and the extent to which they are valued by society (Cash et al., 2004). The psychological and behavioral impacts of these body weight ideals are particularly salient during late adolescence and emerging adulthood when key psychosocial tasks involve developing a sense of identity, what it means to be “feminine, along with a preoccupation with relationships and peer evaluations (Erikson, 1959). Indeed, this time in women’s lives is vital for the formation of schemas that identify how they should look and present themselves (Côté and Levine, 2002). Although there has been a reactive movement in recent years promoting body acceptance and recognizing heterogeneity of body types, sizes, and shapes, the prevailing discourse is that these “other” forms of beauty still reify the implicit notion that the canonical feminine form is unrealistically thin (Attie and Brooks-Gunn, 1989). For women with PCOS, this already tumultuous period is further exacerbated by the symptoms of a disorder that severely challenges these feminine conceptions, and this may be reflected in the resources that women are provided for symptom management.
The array of symptoms associated with PCOS and their various functions are vast. Therefore, symptom management is usually a combination of medication and lifestyle changes (Setji and Brown, 2007). Most commonly, women are prescribed oral contraceptives and are often placed on dietary plans and/or exercise regimens (Dokras et al., 2017; Setji and Brown, 2007). Women in the study of Williams et al. (2016) described protocols for symptom management, including daily skincare (for acne management), hair care routines (for hirsutism), and diet and exercise regimens to control their weight. Although it has been established that physicians and specialists recommend diet and exercise as the first line of defense (Dokras et al., 2017), it is unclear whether age-related differences exist in physicians’ likelihood of promoting diet and exercise in place of other, more holistic symptom management options.
There are two gaps in this area of the literature. It is unclear whether age plays a role in (a) women’s experiences with the structure and functions of their body and (b) medical professionals’ recommendations for PCOS symptom management and treatment. Preliminary research suggests that societal expectations of women are reinforced and thus perpetuated by medical professionals (e.g. Dokras et al., 2017), and this may especially be the case for emerging adult women with PCOS. First, emerging adult and midlife women diagnosed with PCOS experience the challenges of societal values and expectations in terms of both the appearance (thinness and masculine characteristics) and the link between fertility (irregular menstruation and disrupted ovulation) and femininity (Kitzinger and Willmott, 2002). This may especially be the case for emerging adult women who, upon receiving diagnosis, may fear for the future. For instance, younger women in Nasiri-Amiri et al.’s (2014) study were especially concerned about their ability to bear children and felt a “loss of womanhood” as a result of having PCOS.
Second, because of the biological mechanisms through which PCOS operates, traditional approaches to weight and symptom management, like attempting to change one’s diet and increase exercise, are substantially less effective, leading to feelings of failure, self-blame, disordered eating patterns, and depression, particularly for younger women (Himelein and Thatcher, 2006). This is problematic in that medical professionals may not be tailoring symptom management approaches to the individual women and not considering salient factors like age. For instance, Legro (2017) identified that, although it is difficult to treat all the symptoms of PCOS at once, one of the most common treatment foci tends to be weight management. Despite this, women in previous studies have reported that the information they received was dissatisfactory (Gibson-Helm et al., 2014). Although it is unclear why physicians are focusing primarily on weight, it may be a way to provide an easy, band-aid solution that aligns with the current sociocultural pressures to be thin (Thompson and Stice, 2001). These preliminary findings highlight the necessity of research on age-related differences in women’s experiences with PCOS that accounts for individual differences.
Although there is no research to date examining the relationship between the concerns associated with the symptoms of PCOS and body esteem, it is possible that age may be a risk factor for the negative effects of the symptoms of this disorder for emerging adult women and a buffer against the negative effects for midlife women. For example, a large number of literature suggests that midlife and older women are more satisfied and accepting of their appearance and body compositions, despite age-related normative changes in their appearance (e.g. a slowing metabolic rate and menopause; Chrisler and Ghiz (1993); Lee (2013); Ogle and Damhorst (2005)), while late adolescence and emerging adult women are most preoccupied with their appearance as they conflate a thin body ideal with a burgeoning identity (Thompson and Stice, 2001; Wharton et al., 2008). As well, physicians, in their role of the diagnosing body, may be contributing to this disconnect between emerging adult and midlife women’s experience and management of their symptoms by ascribing to ubiquitous age- and appearance-related stereotypes (Tylka et al., 2014).
Purpose of the present study
Given that women with PCOS experience more misalignment with a feminine ideal and difficulty navigating societal expectations with the reality of the disorder, the present study has two aims: (a) to explore the role that age played in the concerns related to the debilitating effects of PCOS-related symptoms on women’s body esteem and (b) to investigate whether the symptom management recommendations provided to women differed by age. We hypothesized that younger, emerging adult women would express concern with their symptoms to a greater extent than midlife women, who would likely accept this diagnosis as part of who they are as women. We, thus, examined the hypothesis that age would moderate the relationship between the concerns associated with obesity- and menstrual-related symptoms (i.e. the more directly observable and chronic concerns associated with PCOS, which challenge the concept of femininity) and facets of body esteem (i.e. sexual attractiveness (SA), weight control (WC), and physical condition (PC)) in a diverse sample of Canadian women diagnosed with PCOS by a medical professional. We also hypothesized that medical personnel would recommend body alteration through diet and exercise, and thus, reinforce appearance standards, to a larger proportion of younger than midlife women.
Method
Participants
We recruited women with a confirmed diagnosis of PCOS (N = 62) from a mid-sized Canadian university (n = 12) and from the local community (n = 50). 1 The ethnicity breakdown was 83.9 percent in Caucasian/White, 6.5 percent in Middle Eastern, 1.6 percent in South Asian, 1.6 percent in Jamaican, and 6.5 percent in mixed descent. Their ages ranged from 18 to 47 (M = 28.10, standard deviation (SD) = 7.49). The mean length of time since receiving their diagnosis was 3.78 (SD = 1.74) years for emerging adult women and 4.23 (SD = 2.03) years for midlife women. The average number of physicians seen for PCOS was 3.54 (SD = 2.09) for emerging adult women and 4.77 (SD = 2.41) for midlife women. Body mass index (BMI) ranged from 19.78 to 48.35 (M = 31.92; SD = 6.72) with 17.5 percent being classified as normal weight, 20.6 percent as overweight, and 60.3 percent as obese. 2
Measures
Body esteem scale
The body esteem scale (BES; Franzoi and Shields, 1984) is a 35-item measure of body-related self-esteem, comprising the following subscales: SA, WC, and PC. Each subscale comprises items of the body associated with that function (e.g. lips for SA, waist for WC, and physical stamina for PC). A sample item from the BES_SA subscale is “sex organs.” Items are answered from 1 (have strong negative feelings) to 5 (have strong positive feelings), with higher scores indicating more body-positive feelings. Cronbach’s α for the SA, WC, and PC subscales were .87, .91, and .88, respectively.
Polycystic ovary syndrome questionnaire-50
The polycystic ovary syndrome questionnaire-50 (PCOSQ-50; Nasiri-Amiri et al., 2016) is a 50-item measure of concerns associated with PCOS symptoms. We used the obesity and menstrual disorder subscale (PCOS-OM) in the present study. A sample item from that subscale is “Felt concerned about being overweight.” Items are answered from 1 (always) to 5 (never), with higher scores indicating less severe concern with symptom impact. Cronbach’s α from the PCOS-OM subscale was .87.
Demographic questionnaire
Participants reported their age, ethnicity, and BMI. They were also asked about the types of symptom management information they received from their healthcare team.
Procedure
The data used in the present study were originally collected for another study investigating women’s diagnostic experiences pre-, during, and post-diagnosis within the context of the Canadian healthcare system. The study was approved by the University’s Research Ethics Board (REB# 34212). The participants provided their written consent before completing the demographic questionnaire, followed by the BES and PCOSQ-50 in randomized order.
Results
Descriptive statistics are presented in Table 1. We satisfied the assumptions of moderation, and there were no outliers using a standard score cutoff of +/−3.29 or influential observations using standardized DFBETA (cutoff of|2|). We assessed moderation using Hayes’ (2013) PROCESS Macro v3.0, which is an observed variable ordinary least squares regression path analysis tool estimating direct and indirect effects. For each moderation analysis, both independent variables (i.e. PCOS-OM subscale and age) were entered as predictors of each dependent variable in step 1, and the interaction term (mean-centered) was entered in step 2 to explicitly test for moderation. BMI was considered as a covariate, but ultimately was not used. There was very little variability in BMI (i.e. most women had a BMI of 30 +) and this is not surprising given that one of the most common symptoms of PCOS is obesity. Therefore, only length of time (until diagnosis was received) was specified as a covariate in each analysis. We dichotomized age into emerging adult (18–29; n = 36) and midlife-aged women (30–47; n = 26) for two reasons. First, the split reflects divisions in previous research studies on women’s body image, where younger, emerging adult women were under 30 years of age and adult or midlife women were 30 + (e.g. Allaz et al., 1998; Becker et al., 2013). Second, given the smaller nature of the sample, the dichotomization provides a clearer interpretation of the results (De Coster et al., 2011).
Descriptive statistics and correlations (N = 62).
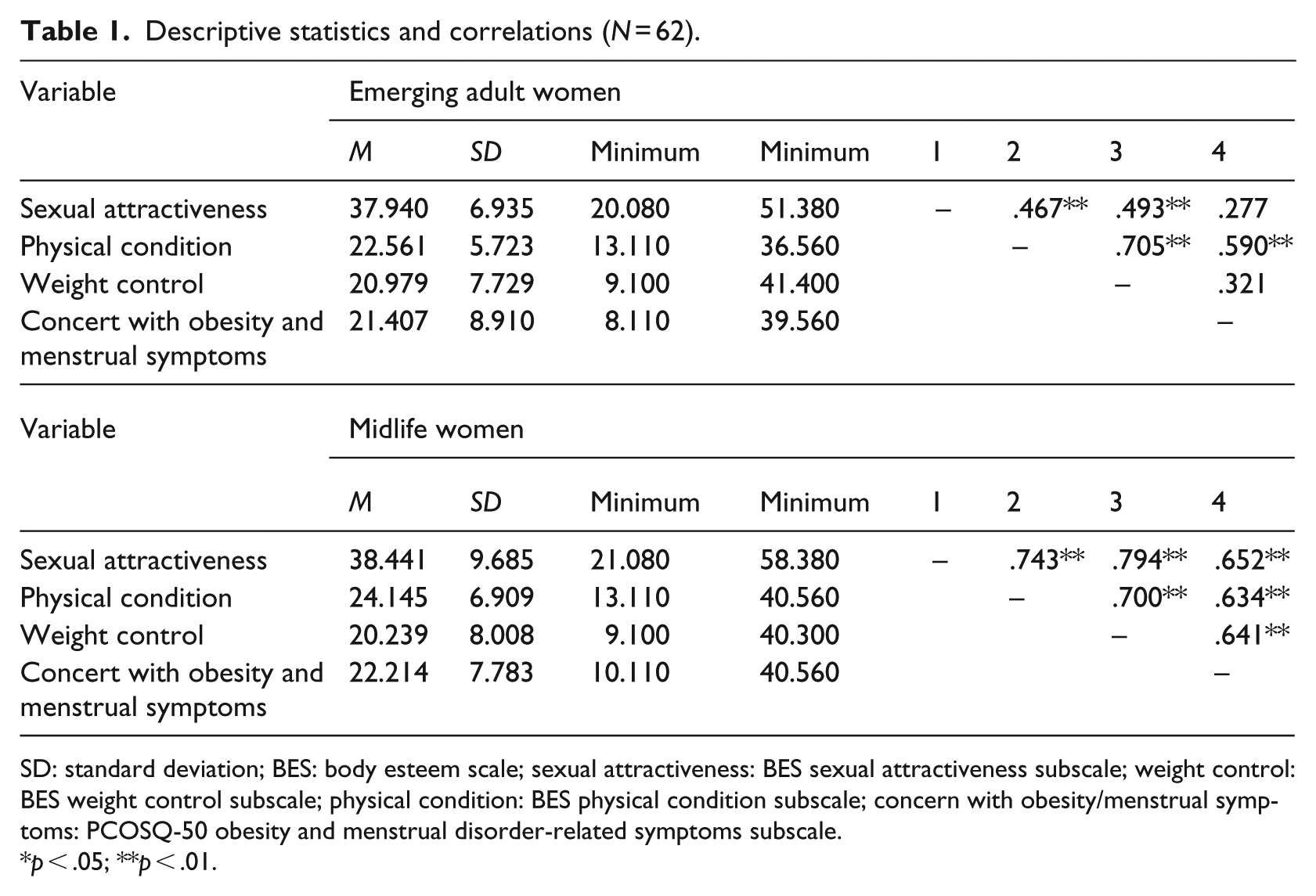
SD: standard deviation; BES: body esteem scale; sexual attractiveness: BES sexual attractiveness subscale; weight control: BES weight control subscale; physical condition: BES physical condition subscale; concern with obesity/menstrual symptoms: PCOSQ-50 obesity and menstrual disorder-related symptoms subscale.
p < .05; **p < .01.
The role of age
Body esteem
Sexual attractiveness
The relationship between PCOS-OM and SA was hypothesized to be moderated by age. Time of diagnosis was not a significant covariate (p = .412). In step 1, PCOS-OM and age were entered as predictors. PCOS-OM did not predict SA, b = −.475, standard error (SE) = .328 (−1.132, .182). Age was a significant predictor of SA, b = −13.258, SE = 5.365 (−24.001, –2.515). As expected, age was found to be a significant moderator, b = .623, SE = .229 (.165, 1.081). Overall, the moderation model predicted 28 percent of the SA variance, F (1, 57) = 7.420, p = .009, ∆R2 = .094. Simple slopes analyses indicated that the relationship between PCOS-OM and SA was significant for midlife women, b = .771, SE = .190 (.390, 1.151). This was not significant for emerging adult women (see Figure 1), b = .148, SE = .140 (−.133, .428).
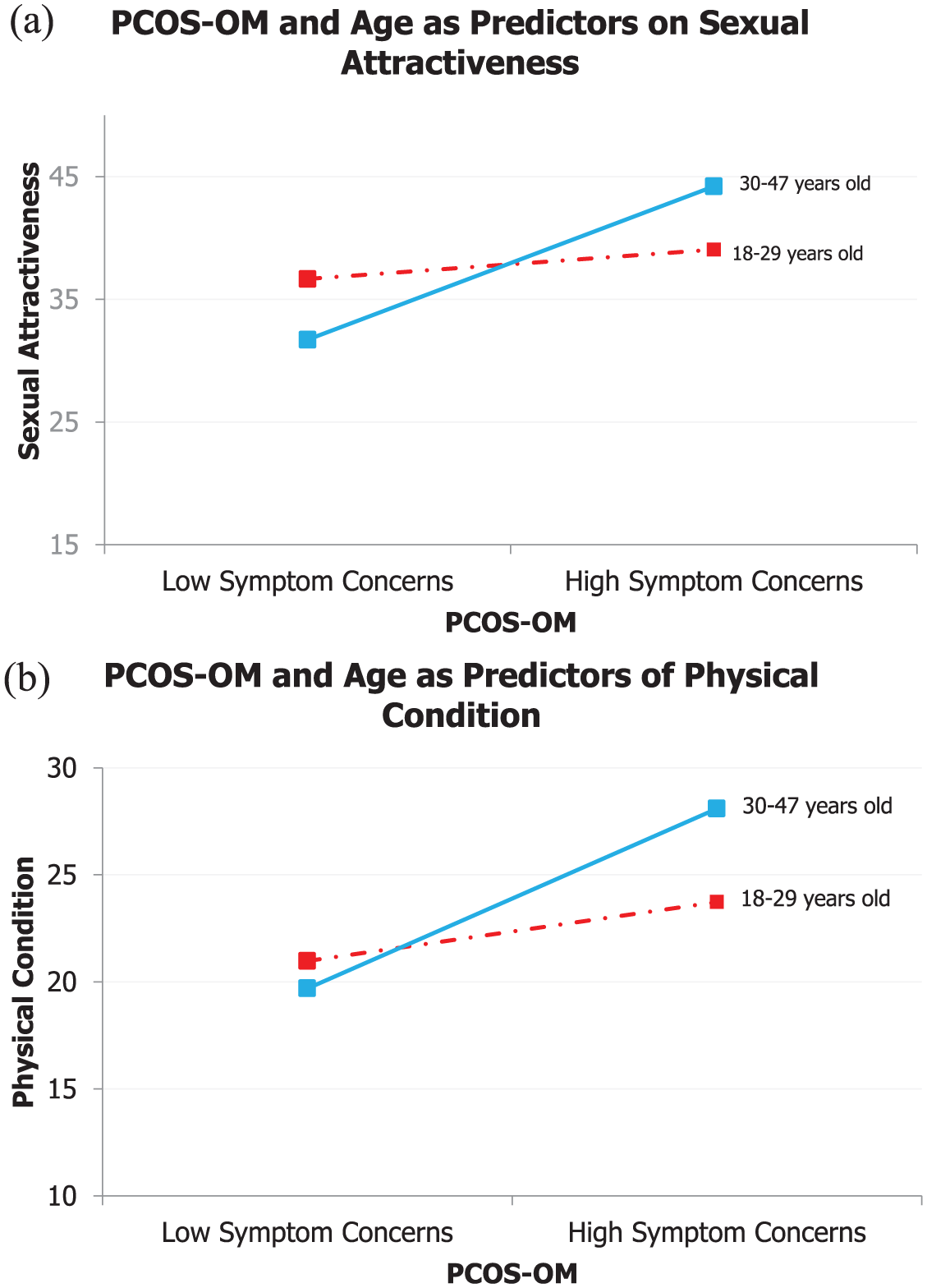
(a) The relationship between PCOS-OM and SA moderated by age. (b) The relationship between PCOS-OM and PC moderated by age.
Physical condition
The relationship between PCOS-OM and PC was hypothesized to be moderated by age. Time of diagnosis was not a significant covariate (p = .179). In step 1, PCOS-OM and age were entered as predictors. Again, PCOS-OM did not predict PC, b = −.179, SE = .249 (−.677, .320). Age also did not predict PC, b = −5.938, SE = 4.072 (−14.092, 2.213). Age was found to be a significant moderator, b = .349, SE = .174 (.001, .696). Overall, the moderation model predicted 30 percent of the PC variance, F (1, 57) = 4.033, p = .049, ∆R2 = .050. Simple slopes analyses indicated that the relationship between PCOS-OM and PC was significant for midlife women, b = .518, SE = .144 (.229, .807). This was not significant for emerging adult women (see Figure 1), b = .170, SE = .106 (−.043, .383).
Weight control
The relationship between PCOS-OM and WC was hypothesized to be moderated by age. Time of diagnosis was not a significant covariate (p = .320). In step 1, PCOS-OM and age were entered as predictors. PCOS-OM did not predict WC, b = .352, SE = .291 (−.230, .934). Age also did not predict WC, b = −3.586, SE = 4.751 (−13.100, 5.928). The relationship between PCOS-OM and WC was not moderated by age, b = .128, SE = .203 (−.277, .534).
Physicians’ recommendations for symptom management
Women’s experiences while dealing with a life-altering disorder like PCOS can be complicated, and physicians tend to be the first individuals from whom women seek information on symptom management and treatment. Therefore, in an attempt to understand age-related differences in the experiences of women diagnosed with PCOS, we investigated the information that women at different ages were given about PCOS management by their primary healthcare team (i.e. family practitioners, specialists), typically at the onset of receiving a PCOS diagnosis (see Tables 2 and 3 for a summary). 3 We explored medication options (e.g. birth control and Metformin), weight management (e.g. low-carb diet and seeing a nutritionist), lifestyle management (e.g. mental health resources), and alternative options (e.g. acupuncture and online support groups). Most women in this study received medication information (86% and 77%, respectively) and weight management information (58% and 62%, respectively). Medications prescribed almost always included birth control to regulate their menstrual cycles as well as Metformin that regulates glucose levels and increases insulin sensitivity (Lashen, 2010). Over half of the women in our study (60%) reported receiving information on weight loss. It is unclear, however, whether these recommendations came with consideration of the complex nature of PCOS or provision of weight loss plan that was tailored to weight loss challenges of PCOS.
Description of women’s diagnostic processes grouped by age.
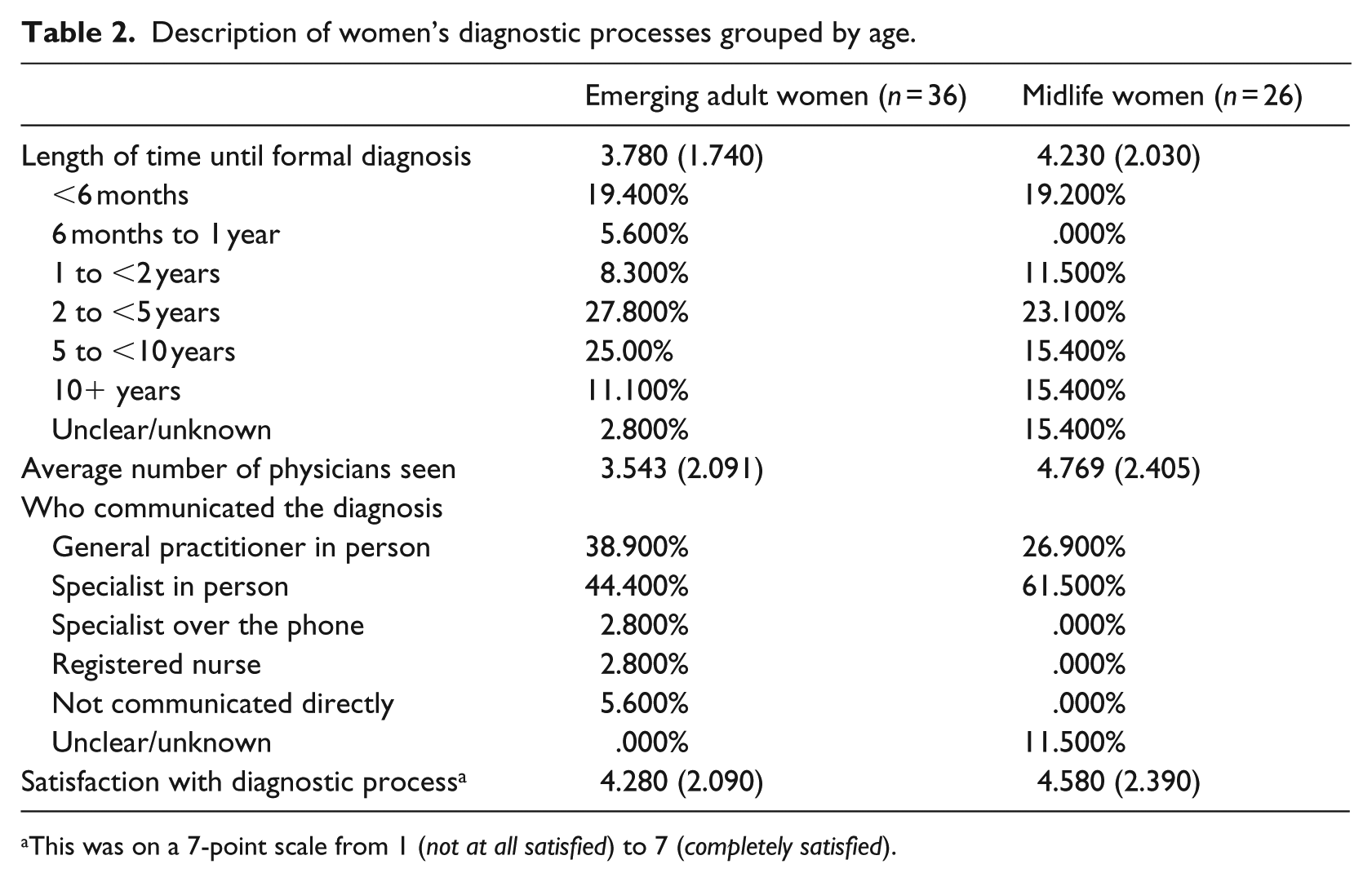
This was on a 7-point scale from 1 (not at all satisfied) to 7 (completely satisfied).
Description of information provided by type and age.

There are no statistically significant differences between emerging adult and midlife women on any of the types of information provided.
Emerging adult and midlife women reported receiving similar amounts of information about “lifestyle management” (25% and 35%, respectively). However, upon closer inspection, this seemed to be mostly related to changing eating behaviors. In fact, 55 percent of the emerging adult and 33 percent of the midlife women, who received “lifestyle information” said that this information was about diet and exercise. Finally, far less young than midlife women received alternative option information (11% and 46%, respectively). These included naturopathic care, nutritionists, acupuncture, online support groups, and medical marijuana, all of which target various difficulties associated with PCOS.
Discussion
The aims of the study were to examine age-related differences in (a) how women with PCOS feel about their symptoms and both the structure and functions of their body (i.e. their perceived SA, WC, and PC) and (b) the symptom management recommendations that frontline medical personnel were providing women diagnosed with PCOS. We found that midlife women (30 + years old) concerned with debilitating menstrual- and obesity-related PCOS symptoms reported feeling more sexually desirable and physically fit than emerging adult women (< 30-years old), who felt less sexually desirable and physically fit. However, we found no age-related differences in women’s feelings of control over their weight.
Given that physicians are the first line of defense for women to seek information from, we investigated age-related differences in the types of symptom management information that these women were receiving by their primary health team. We found that primary care professionals, the frontline practitioners, who are diagnosing these women and providing them with the information necessary for the successful management of PCOS, were recommending treatment regimens that uphold sociocultural standards of thinness that are expectant of emerging adult women (i.e. diet and exercise). Midlife women, however, received more alternative medication options (e.g. acupuncture, online support groups).
One of the key findings in this study is that age acted as a buffer for the concerns associated with debilitating PCOS symptoms like weight gain and menstrual-related issues for older women. Although these findings are preliminary, midlife women seem to be more accepting of their bodies and less concerned with these symptoms despite being considered obese via BMI, suggesting that age buffers negative body image in these women. Although no study has investigated this within the PCOS context, Hurd (2000) found that, despite experiencing extra pressure to fit into youth-centered beauty standards, women felt that health was more important than physical attractiveness. Our findings align with limited previous research (Chrisler and Ghiz, 1993) that suggests that midlife women are still concerned about their bodies but that they may take a more holistic perspective to include their health, which may make the practice of body positivity much easier compared to younger women.
Another noteworthy finding is that PCOS is a disorder that threatens the aspects of the self that are at the very core of what it means to be a woman in the current sociocultural climate. Because Western society places emphasis on body parts reflecting beauty ideals (Cash and Henry, 1995), an inability to achieve that, especially when it is outside one’s control—like suffering from a debilitating health condition—threatens the very nature of the feminine. Struggling with excess and uncontrollable weight gain and the uncomfortable symptoms associated with PCOS means deviating from the pervasive cultural norms of women as being thin, and therefore, beautiful (Becker et al., 2013). A stark example of this comes from Kitzinger and Willmott’s (2002) interviews, where the women discussed a fear of “the freak.” They compared their outwardly-presenting symptoms observed at the circus (i.e. “bearded ladies” and “hairy monsters”). Similarly, Iranian women in Nasiri-Amiri et al.’s (2014) study felt unwomanly and unattractive—both physically and sexually—as a result of PCOS.
Women, especially younger women, in our study highlighted that their healthcare team may have inadvertently contributed to this by placing emphasis on weight loss. It is possible that physicians are addressing weight concerns first because emerging adult women themselves are concerned or because obesity is a debilitating symptom of PCOS (Dokras et al., 2017). However, similar to previous research, emphasis on weight loss as the focal point of treatment may imply a bias toward upholding sociocultural beauty standards, whether intentional or not. For instance, Dokras et al. (2017) found that doctors focused on birth control and lifestyle management to manage PCOS symptoms. The healthcare professionals did not place as much emphasis on midlife women, who tended to receive a more nuanced management plan that included alternatives like online support groups. This emphasis on weight loss can be difficult for many women diagnosed with PCOS (Nasiri-Amiri et al., 2014). More research is necessary to investigate whether physicians’ treatment plans for women with PCOS are influenced, at least in part, by the larger sociocultural context in which they practice.
Notwithstanding, our sample size of 62 women is not representative of all women with PCOS in Canada. Most women were from Ontario, Canada, which limits finding generalizability. However, there is little research on this pervasive women’s health issue and the majority of the scant research derives from countries outside of Canada, such as Australia (e.g. Gibson-Helm et al., 2014, 2018) and Iran (e.g. Mehrabian et al., 2011; Nasiri-Amiri et al., 2016), which have starkly different healthcare systems. Canada differs from other countries in that its healthcare system is publicly funded. The provision of services depends on need rather than one’s ability to pay (Government of Canada, 2018). Also, it is important to recognize that a sample of this size of women with PCOS is still a salient first step in determining gaps in symptom management.
Second, we did not ask for information on time since diagnosis of the women in our study. This information would have been useful in controlling for recall bias. However, we did ask women how long it took them to receive a diagnosis and although non-significant, we included this as a proxy adjustment for recall bias. One possible solution for future researchers is to employ interview techniques and to isolate the period of the event to facilitate easier recall (Biemer et al., 1991). Next, a majority of our sample identified as Caucasian, so future research is required to disentangle and expand upon these findings within other cultural and ethnic contexts. We also recognize that the Canadian healthcare system is drastically different from healthcare systems found in other countries, so there is a need for consideration of other policies and funding for specialists in future studies.
Implications for practice and/or policy
Despite the limitations, this study has implications for practice and research on women’s health issues. First, future research may benefit from implementing qualitative designs unpacking the diagnostic experiences of women with PCOS to better capture these age-related differences in greater detail. This will allow for the construction of meaning from lived experiences through the voices and perspectives of women diagnosed with PCOS. Although our study only focused on one visible symptom concern, it is possible that other equally visible and debilitating symptoms of PCOS (e.g. acne, unwanted hair growth) cause concerns within other contexts. Further exploration is necessary in order to investigate whether the role of age found in this study holds in these other relationships. This study also points to the importance of encouraging targeted body acceptance, education, and advocacy interventions for younger, emerging adult women with PCOS.
Second, these findings illustrate the constant need for women to deconstruct the culturally-sanctioned ideals of beauty and femininity inherent in social structures and dynamics. One potential avenue for this is through conversations with medical health professionals, like general practitioners and specialists. Although this could be empowering, it also illuminates the disconnect between the medical profession and the treatment of PCOS. Indeed, Dokras et al. (2017) noted that many physicians were not aware of the criteria used to diagnose a woman with PCOS. Therefore, this may prompt women to do their own research about their symptoms and management of them, furthering the disconnection from the medical profession. Previous research suggests that some physicians may experience discomfort discussing women’s health issues (Hsieh et al., 2013). Despite this, more training for physicians and frontline about PCOS and similar women’s health issues, and with a focus on the complexities (e.g. the difficulty in losing weight because of the insulin resistance) may help to deviate from these ubiquitous cultural beauty ideals that are integrally damaging.
Conclusion
Among a group of women diagnosed with PCOS, we found a buffering age effect, wherein midlife women felt more sexually attractive and physically fit despite concerns related to obesity and menstrual issues. Physicians may be reinforcing beauty standards by recommending weight loss as a quick-fix solution and not considering PCOS holistically. Our findings suggest that physicians need more training to be able to adequately manage and/or treat women’s health issues. As well, we suggest targeted body acceptance education and workshops for younger, emerging adult women suffering from PCOS.
Footnotes
Acknowledgements
The authors of this paper would like to express their gratitude to the following Life Memories Lab research assistants and volunteers: Amanda Bailey, Sanaya Dhabhar, Christine Elgie, Rachel Katzman, Rachel Plowman, and Chantal Vien.
Ethical approval and consent to participate
This research received clearance by the Research Ethics Board at the University of Windsor, Ontario, Canada (REB# 34212). Hence, the rights of the participants were protected, and all applicable human research subject guidelines were followed. All participants provided their written consent to participate.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the University of Windsor with an Internal Grant for Women (eRSO #33937, 2015).