
Abstract
The use of graded exercise therapy and cognitive behavioural therapy for myalgic encephalomyelitis/chronic fatigue syndrome has attracted considerable controversy. This controversy relates not only to the disputed evidence for treatment efficacy but also to widespread reports from patients that graded exercise therapy, in particular, has caused them harm. We surveyed the National Health Service–affiliated myalgic encephalomyelitis/chronic fatigue syndrome specialist clinics in England to assess how harms following treatment are detected and to examine how patients are warned about the potential for harms. We sent 57 clinics standardised information requests under the United Kingdom’s Freedom of Information Act. Data were received from 38 clinics. Clinics were highly inconsistent in their approaches to the issue of treatment-related harm. They placed little or no focus on the potential for treatment-related harm in their written information for patients and for staff. Furthermore, no clinic reported any cases of treatment-related harm, despite acknowledging that many patients dropped out of treatment. In light of these findings, we recommend that clinics develop standardised protocols for anticipating, recording, and remedying harms, and that these protocols allow for therapies to be discontinued immediately whenever harm is identified.
Keywords
In 2007, the United Kingdom’s National Institute for Health and Care Excellence (NICE) published treatment guidelines for myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS). The guidelines recommended three therapies aimed at rehabilitating patients by having them gradually increase their activity levels: ‘activity management’, graded exercise therapy (GET), and a form of cognitive behavioural therapy (CBT) intended to persuade patients to increase their activity (NICE, 2007). NICE guidelines are formally directed at National Health Service (NHS) specialist ME/CFS clinics in England and are also used in the rest of the United Kingdom and have influenced practice recommendations in several other countries. However, despite their status as officially recommended treatments, the use of GET and CBT for ME/CFS has attracted considerable controversy. Critics argue (a) that the evidence that these therapies are effective for ME/CFS is flawed and that any apparently positive effects could be due to methodological bias (McPhee, 2017; Vink and Vink-Niese, 2018; Wilshire et al., 2018), and (b) that GET in particular seems harmful to patients (Geraghty et al., 2019). Against this background, the US Centers for Disease Control and Prevention removed GET and CBT from their own ME/CFS treatment guidelines in 2017 (ME Association, 2017). NICE is now reviewing its guidelines for the United Kingdom (NICE, 2017).
When treating patients, all therapies carry some element of risk. A treatment is therefore usually recommended only when a cost–benefit risk analysis shows that the likelihood and extent of benefits clearly outweigh those of the risks. In clinical research, harm is more likely to be investigated for pharmacological treatments than for non-pharmacological ones (Duggan et al., 2014; Meister et al., 2016). However, the cost–benefit principle applies as much to non-pharmaceutical therapies, such as exercise, as to any others (Cooper et al., 2007). For GET and CBT in ME/CFS, the evidence for treatment efficacy is disputed and the likely treatment gains are unclear. This means that there should be a strong focus on the therapies’ costs in any cost–benefit analyses.
A common limitation seen in clinical trials across medicine is that the reporting of harms frequently receives much less attention than that of efficacy outcomes (e.g. Ioannidis and Lau, 2001). Some empirical studies of CBT and GET in ME/CFS have reported no apparent safety concerns, although the reporting of harms in such trials has been widely recognised as being poor, with often no data on adverse events being published at all (Chambers et al., 2006; Kindlon, 2011; Marques et al., 2015; Price et al., 2008; Smith et al., 2015). Advocacy groups for ME/CFS patients regularly report concern about the potential for harms arising from these treatments (e.g. ME Association, 2015). A number of surveys by patients’ associations have suggested that CBT and GET can trigger significant deterioration in ME/CFS patients.
Across 11 such surveys, involving nearly 8000 patients in the United Kingdom, Norway, and the Netherlands, cumulative totals of 57 and 20 per cent of all patients surveyed reported deterioration after GET and CBT, respectively (Geraghty et al., 2019). GET was associated with a higher proportion of patients deteriorating than CBT in every survey that examined both. A subsequent survey of patients’ experiences over the past 10 years was commissioned by Forward ME (ME Association, 2019) at the request of NICE. The survey reached a sample of over 2000 patients, roughly a quarter of the number of patients seen in UK NHS ME/CFS clinics each year (British Association for CFS/ME, 2019). Symptom deterioration was reported by 81 per cent of patients who received GET and 47 per cent who received CBT, further confirming the pattern seen by Geraghty, Hann and Kurtev. The deterioration does not appear to be restricted to potentially substandard therapy being provided outside the NHS. One survey (Kindlon, 2011) compared the proportion of patients reporting deterioration following GET and found no difference whether the therapy was provided by NHS specialists or by non-NHS therapists (31% vs 33%).
A multi-site cohort study by Collin and Crawley (2017) confirmed that significant levels of deterioration are reported by patients attending NHS ME/CFS specialist clinics in England. Among 418 patients who were followed up 1 year after baseline, 20 per cent reported that their ME/CFS had worsened; from a subset of 383 who were followed up after 2 or more years, 30 per cent reported worsening. The authors reported these findings as reflecting the often treatment-resistant nature of ME/CFS. However, the prevalence of deterioration from baseline after years of being treated by specialists according to NICE guidelines raises the question of whether practitioners (or researchers) are paying enough attention to the risk of harm in this population, or are equipped to recognise harm when it happens.
A recent service audit conducted by the British Association for CFS/ME (2019), an organisation that supports clinical professionals, suggested that service approaches vary considerably across the UK health system. Tellingly, this report emphasised that, as the area of CFS/ME ‘does not yet have the advantage of an accepted evidence base for diagnosis or treatment’ (p. 34), service design and delivery depend greatly on choices made by clinicians based on their experiences. As such, it is likely that the way clinics deal with the issue of treatment-related harm will be similarly variable.
In the present research, we surveyed all NHS-affiliated ME/CFS specialist clinics in England to assess how harms following treatment are detected and to identify practices for warning patients about the potential for harms during, after, or arising from treatment. We requested information from individual clinics to gain insight into their readiness to deal with harms.
Method
Sampling frame and contact
Based on an online directory publicly posted by the ME Association (a registered UK charity) as of November 2018 (ME Association, 2018), we identified 57 separate specialist NHS centres in England providing services to adult ME/CFS patients. During the period of November 2018 to January 2019, we sent each clinic (or the NHS Trust that provided it, as listed in the ME Association’s directory) a standardised freedom-of-information request asking about information and data relating to harms (see section ‘Information requested’). The United Kingdom’s Freedom of Information Act (FOIA) requires public authorities to provide recorded information in response to requests, but authorities do not need to respond to questions that cannot be answered with recorded data (Information Commissioner’s Office, 2019). Nonetheless, we also asked each centre to send us any verbal information about harm that it gave to ME/CFS patients and staff if it did not provide them with written information.
We sent a single reminder to any clinic that had not responded within the 20-working-day period set out in the FOIA. We closed data collection when each clinic had had at least 30 working days to reply to our original request.
We established that 11 of the 57 centres no longer functioned at the time they were contacted. Two further clinics told us that they did not provide rehabilitative therapies (such as GET or CBT) to ME/CFS patients. This left a final target sample of 44 centres in this study.
Information requested
Information for patients and staff about risks and harms
The first two questions in our freedom-of-information requests related to information given to patients and staff about safety, risk, and harm in relation to rehabilitative therapies.
The first question was:
Please provide the information that you give ME/CFS patients about the safety and risks of the rehabilitative therapies (e.g. CBT, graded exercise therapy, activity management) provided by your service. If information is only provided verbally, we would be grateful for a brief summary. If you do not give patients such information in any form, please say so.
The second question was:
Please provide us with any written guidance that you use to determine whether an ME/CFS patient has been harmed by the rehabilitative therapies (e.g. CBT, graded exercise therapy, activity management) provided by your service. This may include training material that you use to help your staff recognise harms. If you use unwritten criteria to determine whether a patient has been harmed, we would be grateful for a brief summary. If you have no criteria for judging whether a patient has been harmed, please say so. If you used different guidance for the patients in the time period dealt with in [the subsequent questions], please provide that also.
Quantitative data requests
The remaining five questions were numerical and related to data on the patients who began treatment in 2016 (or, if data for this period were not available, for the nearest earlier 1-year period starting on any calendar date). 2016 was chosen to be long enough ago for post-treatment harms to be detected and follow-up to have taken place.
The questions asked (a) how many patients began therapy; (b) how many dropped out because their condition worsened, because they experienced harm from the therapy, or because of an unknown reason; (c) how many reported an increase in symptoms that had lasted for more than a few days and/or that their symptoms had become severe or distressing (according to the NICE (2007) guidelines, healthcare professionals should advise ME/CFS patients to contact them if this happens); (d) how many patients were recorded as having been harmed by their therapy; and (e) how long any follow-up period was, and how many patients had been lost to follow-up.
Data extraction and analysis
Two members of the research group, who had coding experience, independently extracted 22 items of data from each clinic’s responses. For the responses to the first question, about the information given to patients about risks and harms, the coders used a list of statements such as ‘Symptoms may worsen temporarily’. The coders judged whether the clinics had made each statement – or something that meant the same – to any of their patients (see Table 1 for the full list). For the second question, the coders judged whether the clinic had criteria to determine whether a patient has been harmed, and for the quantitative questions, the coders attempted to extract the quantitative data and some summary information about how any follow-up of patients was conducted.
Information provided by ME/CFS clinics (N = 38) to patients regarding safety and risks of rehabilitative therapies.
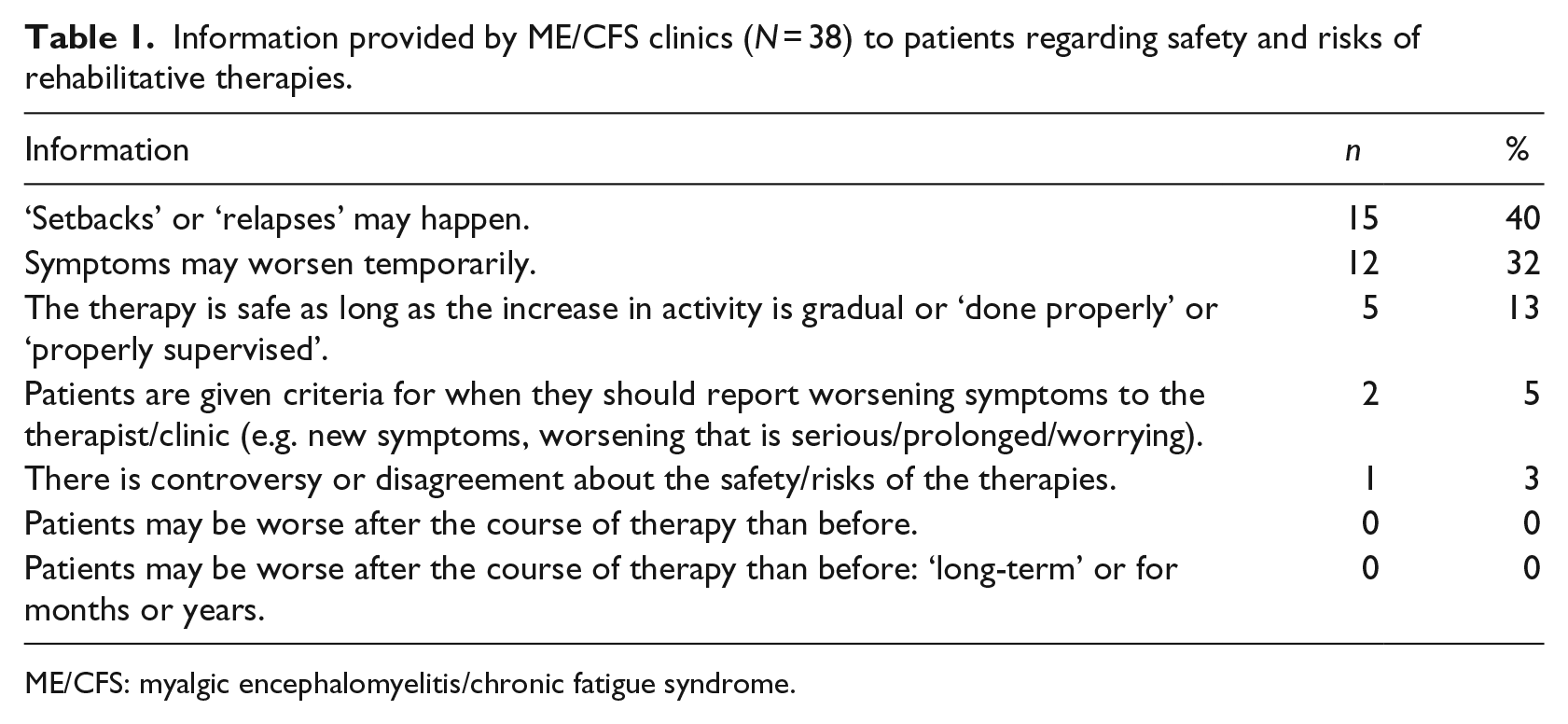
ME/CFS: myalgic encephalomyelitis/chronic fatigue syndrome.
There were two disagreements that could not be resolved between the coders and these were resolved by a third party (also from the research group). For each data item, we calculated the percentage of clinics for which the two coders agreed on the data. Median agreement across items was 95 per cent (interquartile range (IQR) = 89%–97%).
Results
Response rate
Four of the 44 clinics eligible for inclusion did not respond by the cut-off date. Also, two centres that contracted their services out to private providers declined to take part on the basis that private providers are exempt from the FOIA. Thus, responses were received from a total of 38 eligible clinics, giving a response rate of 86 per cent.
Guidance for patients about safety and risks
Table 1 shows information that clinics reported giving ME/CFS patients about the safety and risks of the rehabilitative therapies, as classified by our coders. (Warnings about symptoms not directly related to ME/CFS, such as chest pain during exercise or emotional distress from facing the reality of symptoms, were not included.) The most commonly reported guidance from clinics was that ‘setbacks’ or ‘relapses’ were possible (N = 15; 40%). The second common piece of advice was that ‘symptoms may worsen temporarily’ (N = 12; 32%). Only one of the 38 clinics reported telling patients that the safety of the rehabilitative therapies is disputed.
Guidance for staff about safety and risks
Just 1 of the 38 clinics reported having guidance for determining whether a patient had been harmed during or after ME/CFS treatment. They described their approach as follows:
Harm may be defined by the patient as [it] could take different forms … If patients rate their health as worse or much worse we review the written information to assess if this is related to the treatment or to other causes, such as a deterioration in co-morbidities or a life event.
A number of other clinics reported that they used scales such as the 36-Item Short Form Health Survey (SF-36; Ware and Sherbourne, 1992) to measure improvement and deterioration. However, no clinic said how or whether they used any such measure to determine whether a patient had been, or might have been, harmed.
Overall, 18 clinics (47%) responded that they gave no written guidance to staff about harm detection, nor did they report giving any verbal guidance; 19 clinics (50%) gave responses that did not address the question.
Quantitative data requests
Of the 38 clinics, 23 (61%) provided at least some quantitative data for a specified 1-year period in response to our data request; 15 clinics gave information for patients starting treatment in 2016, with the rest giving information for 1-year period in the range of 2015–2018. Fifteen clinics made it clear how many patients began treatment during the year; the median number of patients in these clinics was 132 (full range = 26–450; IQR = 58–212).
Table 2 summarises the clinics’ responses relating to harms. Given the small number of cases, individual values are presented rather than summary statistics.
Data provided by ME/CFS clinics (N = 38) relating to treatment harm.

ME/CFS: myalgic encephalomyelitis/chronic fatigue syndrome.
Altogether, it was clear for 12 clinics that they followed up all patients once treatment was completed. The number of follow-ups ranged from one to four. For two of these clinics, follow-up was 12 months after initial assessment of the patient; for nine clinics, follow-up was timed from the patient’s final treatment session and was between 3 and 12 months later. The remaining clinic did not specify its follow-up timing.
Discussion
This study was conducted to assess how NHS ME/CFS clinics in England deal with the possibility of treatment-related harm. Overall, our findings suggest that such clinics place little focus on dealing with such harms, with a general pattern of centres not addressing the issue of harm with patients or staff and, ultimately, reporting no harm.
It is certainly notable that no clinic at all reported any harm for any patient. It is equally notable that all 7 of the 38 clinics that provided dropout rates (18%) reported that patients dropped out of treatment, including for reasons that were unclear. As noted above, previous research has shown that significant numbers of patients receiving rehabilitative therapies report deterioration, both within NHS centres in England (e.g. Collin and Crawley, 2017) and internationally (Geraghty et al., 2019). Against the backdrop of these findings, the centres we sampled seem overly optimistic in reporting zero harm.
We consider three explanations for why centres reported zero treatment-related harm for their services. First, it could just be that no harm occurred in the 17 centres that gave us data. But Collin and Crawley’s (2017) and Geraghty et al.’s (2019) works suggest that harms are not rare. We would have expected to see harms in our dataset and it seems implausible that they would all be concentrated in the 21 clinics that did not report harm rates.
The second possibility is that patients attending the clinics in our dataset did indeed experience harm (which might account for the dropout rates reported), but did not report their harm to the clinics, thus preventing the clinics from recording it. In relation to this, it is worth noting the clinics’ descriptions of their advice to patients. No clinic reported telling patients explicitly that they could be worse after therapy than before. Having not been primed about harm, patients who deteriorated might have been reluctant to report it to their clinic, or might have attributed their deterioration to other causes.
For example, one clinic gives the following text to patients in the ‘Frequently Asked Questions’ section of an information leaflet about GET:
There are many sources of information available on the internet; however it is not always easy to see if this information is factual and correct. Many people have concerns with GET making their condition worse. If GET is correctly undertaken it will not harm you. Many controversies occur when people have undertaken what they feel was GET but this is often not the case. For example we know of cases where it has been a general exercise programme that has been carried out and increased too quickly, leading people to do too much too quickly, thereby having a detrimental effect.
Rather than telling patients that treatment-related harm is possible, this message encourages patients to take personal responsibility for any deterioration (because of not having ‘correctly undertaken’ their therapy) and discourages them from reporting it to their clinic as ‘harm’. Even without priming, patients providing feedback on medical treatment are frequently influenced by socially desirable responding bias (Epstein et al., 2005). Patients may be particularly influenced when clinics tell them that the treatments are effective. A related issue concerns the way therapies such as CBT might teach patients to reframe their negative experiences, further discouraging them from reporting harms (Kindlon, 2017). In combination, such factors are likely to lead to a misinformation ‘loop’, where clinics are reinforced in believing no harms have occurred by the very fact that patients do not report them.
The third possible reason for the reported zero-harm rate is that patients did indeed report harm, or try to do so, but that clinics did not formally record it. As noted above, only one clinic reported any kind of criteria for determining harm. It is unclear how the rest of the clinics would have recorded explicit reports of harm by patients. This matter could be clarified by directly surveying the experiences that patients and staff have had in relation to harm-reporting. We note that therapies such as GET and CBT are not covered by existing national harm-reporting systems (such as the ‘Yellow Card Scheme’ operated by the United Kingdom’s Medicines and Healthcare Products Regulatory Agency). This means that if patients cannot report their harms to the clinics, then no agency at a national level will be aware of these data.
Some comments made by clinics seemed to suggest an institutional scepticism about whether approved therapies for ME/CFS could cause harm. For example, one clinic responded to our request for harm data by stating:
This data is not available. This is making an assumption that treatments we provide are harmful. If any treatment is contraindicated we would not provide it.
ME/CFS is a variable condition, and any patient’s judgement of whether they have been harmed by their treatment must therefore be based on context. They must decide whether any deterioration is beyond the usual variation in their symptoms, fits the timing and happens in the absence of other possible triggers. However, the complexity of this judgement leaves room for clinics to attribute harm to other causes, and if clinics presume that treatments are harmless, they will inevitably fail to record harms accurately.
The NICE (2007) guidelines for ME/CFS explicitly recommend that clinics tell patients to contact them, once they have started therapy, if they experience an increase in symptoms that lasts more than a few days, or if symptoms become severe or distressing. However, only two clinics in this study were able to provide us with the number of patients who had reported such concerns. It therefore seems that few NHS ME/CFS clinics in England are equipped to track these experiences in a formal way. This is concerning, given that NICE appears to consider them important indicators of current or impending harm.
Limitations of the present study
This study offers some initial insights into the issue of harm during or after rehabilitative therapy for ME/CFS, but is limited in several respects. Because we surveyed institutions rather than people, the information gathered is at a macro-level rather than micro-level. It represents the clinics’ official approaches to harm, as outlined by the staff responsible for dealing with the freedom-of-information requests. However, the responses are unlikely to fully capture how frontline clinical staff view or deal with harms in daily practice. As such, it is important to interpret our findings as mainly reflecting institution-level matters. Further research would be needed to examine what the firsthand experiences of patients and their therapists have been. Additional insights could be gained from objective patient-level data on harms.
One related limitation is the fact that clinics may vary in how they define a ‘dropout’. Where clinics allow a patient to stop a particular therapeutic approach – such as GET – while continuing to see a therapist, it is possible that this patient will not be classified as having ‘dropped out’ of therapy. As above, future research that focuses on firsthand patient experiences would clarify whether this has happened.
In addition, the data that we gathered reflect the limitations of making freedom-of-information requests. Such requests are, by their nature, more restricted than the questions used in typical surveys or psychometric research. The FOIA obliges public bodies to supply recorded data that they hold, but does not oblige them to answer questions about what information or material they do not hold. Also, public bodies do not have to respond to questions about experiences and attitudes, such as whether a therapist would record a harm when a patient said they had been made worse by the therapy even if the therapist disagreed. Nor do such bodies have to answer direct questions about procedure, and so we did not ask the clinics whether they warned patients about the controversy surrounding the safety of CBT and GET. The best that we could do was to note such information if it was volunteered. Finally, it is also possible that one or more of the clinics chose to withhold information that we requested, but that would have been against the FOIA, and so we think it unlikely.
Conclusion
This study aimed to get initial insights about how prepared English NHS ME/CFS clinics are to deal with adverse outcomes during or after rehabilitative therapies. Harms may be a decisive factor when weighing up costs and benefits of the therapies, given the controversy over the therapies’ efficacy and the disputes about the quality of the evidence that underpins them.
In this regard, it is striking that among the ME/CFS clinics surveyed in this study, there was an almost universal absence of criteria for detecting harm, and that no clinic reported any harm as having occurred in their patients. Four-fifths of the dataset did not give any information about patients dropping out: of those that did, all of them reported that some patients had dropped out during treatment, with one clinic reporting that as many as 44 per cent of patients did so. However, no clinic reported that they attributed any of this patient dropout to treatment-related harm.
A related point is that clinics mainly reported providing little information to patients about the possibility of harm, although several advised patients that setbacks or relapses could happen. It may be useful for patients to be provided with information about the prevalence of deterioration previously found in NHS CFS clinics (Collin and Crawley, 2017) or reported in other surveys (Geraghty et al., 2019), as well as information about the relative pattern of harms reported for different treatments. Such information will be especially important when seeking to obtain informed consent from patients prior to ME/CFS treatment. Furthermore, there would appear to be clear benefits to a national system for collecting information from patients who believe they have been harmed by rehabilitative therapies, similar to the United Kingdom’s Yellow Card Scheme for collecting information about adverse effects arising from medical drugs or devices.
In the absence of any evidence that clinics systematically record or even screen for harms that might arise from treatment for ME/CFS, clinics should ideally avoid making assumptions that the therapies they offer are harmless because of their nature. This seems a particularly pressing concern given the significant controversy over the evidence for the efficacy of the rehabilitative therapies, and the widespread view among patients and advocates that these therapies can cause harm. Instead, clinics should develop standardised protocols for anticipating, preventing, and, where necessary, recording and remedying harms for those patients affected by them. Such protocols should also provide for therapies to be discontinued immediately wherever they are identified as causing patient harm.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.