
Abstract
We tested whether personality traits help explain the association between discrimination and racial health disparities in a sample of 1033 Black and White older adults. Participants completed measures of discrimination, personality, and self-reported physical and mental health. Elevated discrimination among Black participants was indirectly linked to worse physical and mental health outcomes through elevated neuroticism and lower agreeableness, controlling income, education, and gender. The specific facets of depression, impulsiveness, and trust were the most robust intervening personality factors. Interventions that target cognitive, emotional, and behavioral sequelae of discrimination may lessen its impact on health disparities.
Health disparities between Black and White Americans are pervasive across various health outcomes and throughout the lifespan. Black individuals have lower life expectancy, worse physical functioning, higher rates of physical and mental illnesses, greater psychological distress, and steeper declines in health over time (Asnaani and Hall-Clark, 2017; Brown et al., 2012; McClendon et al., 2019; Thorpe et al., 2016; Williams et al., 1997, 2016). A major focus of the health disparities literature has been to identify psychosocial mechanisms of Black–White health inequalities that may be targeted in interventions and public health initiatives.
Discrimination is a form of psychosocial stress commonly experienced by Black Americans that is associated with poor mental and physical health outcomes (Barnes et al., 2004; Clark et al., 1999; Kessler et al., 1999; Lewis et al., 2015; Mays et al., 2007; Williams and Mohammed, 2009). Discrimination is defined as the unfair treatment of groups of individuals based on socially marginalized aspects of their identity, such as race, ethnicity, culture, gender, or ability. It involves the exclusion, degradation, or harassment of individuals deemed to be inferior based on beliefs perpetuated by dominant institutions and members of society, particularly those from privileged social groups (Schmitt and Branscombe, 2002). Greater self-reported discrimination is associated with lower psychological well-being, higher risks of mental illness (e.g. anxiety, depression, posttraumatic stress disorder, schizophrenia), decreased self-esteem and life satisfaction, less use of needed mental health services, poorer self-reported health, chronic health conditions, physical disability, and biological dysregulation (e.g. high blood pressure) (Brondolo et al., 2011; Burgess et al., 2008; Kessler et al., 1999; Lewis et al., 2015; Mays et al., 2007; Pieterse et al., 2012; Schmitt et al., 2014; Vines et al., 2017; Williams et al., 2008). Marginalized racial groups, such as Black Americans, experience a higher burden of discrimination (Kessler et al., 1999), and evidence suggests that discrimination may contribute to racial health disparities (Williams et al., 2012).
Despite the well-established links between discrimination and health, there is limited knowledge about what factors may contribute to this association (Vines et al., 2017). Identifying putative mechanisms can elucidate the most potent intervention targets for reducing the deleterious effects of discrimination on health. Discrimination may impact health through shaping the development of negative schemas about other people as intentionally harmful and untrustworthy, and the world as uncontrollable and hostile (Brondolo et al., 2011). It may be through the establishment of such cognitive frameworks that discrimination increases negative affect and hypervigilance and erodes trust (Carter, 2007).
Evidence supports associations between discrimination and these affective and behavioral sequelae. A recent meta-analysis found significant small to medium effect sizes for associations between greater self-reported discrimination and poorer psychological well-being (e.g. negative affect, life satisfaction) in both cross-sectional (r = −.23) and longitudinal studies (r = −.15) (Schmitt et al., 2014). Self-reported discrimination is associated with lower trust in medical providers, and trust has been found to mediate associations between discrimination and medication adherence (Cuffee et al., 2013; Hausmann et al., 2013; Haywood et al., 2014). Furthermore, research suggests that self-reported discrimination is associated with hypervigilance, anger, and social avoidance (Carter et al., 2016; Sibrava et al., 2019), even after controlling for other forms of stress (Pieterse et al., 2010).
The broad array of affective and behavioral consequences stemming from self-reported discrimination is closely related to personality traits. For example, negative affect is closely related to the personality trait of neuroticism, and trust is a component of the trait of agreeableness. Personality traits are global constructs related to emotion, cognition, and behavior that represent how people relate to themselves, others, and the world. They are potent predictors of mental and physical health outcomes and are associated with health disparities (Hampson, 2012; McClendon et al., 2019). In personality and health research, personality traits are frequently defined in terms of the five-factor model (FFM). The FFM includes five major domains of personality (i.e. neuroticism, extraversion, openness, agreeableness, and conscientiousness; Costa and McCrae, 1992; Ferguson, 2013). Neuroticism is the tendency to experience negative emotions; extraversion is the tendency to seek stimulation and engage socially; openness is the tendency to prefer a variety of experiences and ideas; agreeableness is the tendency to be trusting and cooperative; and conscientiousness is the tendency to be thoughtful and goal-directed.
Evidence suggests that discrimination is concurrently and prospectively associated with neuroticism, agreeableness, and conscientiousness (Sutin et al., 2016; Xiang et al., 2018). Sutin and colleagues (2016) found that perceived discrimination at initial assessment was associated with decreases in conscientiousness and agreeableness and increases in neuroticism over time in two large independent samples of older adults. These findings provide temporal plausibility that discrimination may change personality. Lower openness, extraversion, and related constructs (e.g. positive affect) have also been linked to greater reported discrimination, albeit cross-sectionally and with weaker effect sizes (Schmitt et al., 2014; Sutin et al., 2016). Discrimination is also linked to personality-related constructs such as elevated depression and anxiety symptoms, hostility and anger, and lower self-control (Brondolo et al., 2011; Williams et al., 2012). Alongside evidence that personality traits are consistently and robustly associated with health outcomes (Ferguson, 2013; Hampson, 2012; Iacovino et al., 2016; Weston et al., 2015), these data suggest that discrimination-related racial health disparities may be partially attributable to discrimination-related differences in personality.
In the current study, we tested whether discrimination and personality traits indirectly link race to physical and mental health outcomes. We hypothesized that Black participants would report higher levels of discrimination, which would be associated with higher neuroticism, lower agreeableness, and lower conscientiousness, which in turn, would be associated with poorer mental and physical health. We focus on these specific personality traits due to evidence of their prospective relationships with discrimination, though we also explore associations of discrimination with openness and extraversion. Furthermore, given evidence that Black Americans report lower levels of trust than Whites in a variety of domains (e.g. health care, interpersonal relationships; Armstrong et al., 2013; Iacovino et al., 2014a; Smith, 2010) and that trust is associated with health outcomes (Lee and Lin, 2011; Verhaeghe and Bracke, 2011), we expected the trust facet of agreeableness to be the most robust predictor.
Methods
Participants
Participants were drawn from the St. Louis Personality and Aging Network (SPAN) study, an ongoing longitudinal protocol assessing a wide range of personality, health, social, and biological characteristics in a representative community sample of 1630 older adults recruited from the St. Louis metropolitan area (wave 1: ages 55–64; 55% female; 65% White, 32% Black; Oltmanns et al., 2014). Participants were recruited using listed phone numbers that were crossed with current census data to identify households with at least one member in the eligible age range. An over-sampling procedure was employed during recruitment to increase representation of Black men, who were underrepresented during the early phases of recruitment (see Spence and Oltmanns, 2011 for more detail). Exclusion criteria included lacking a permanent residence, a lower than sixth grade reading level and active psychotic symptoms. Each participant completed a 3 hour in-person assessment at wave 1 and was invited to complete two subsequent in-person follow-up sessions approximately every 3–3.5 years. Participants were also asked to complete a short sequence of mailed or online follow-up questionnaires every 6 months after entering the study.
There were 1033 Black and White participants (mean age = 66.4 years, standard deviation (SD) = 2.9 years, range = 60.7–73.3 years; 28% Black, 72% White) who completed the assessment time-point at which the measure of discrimination was administered (i.e. wave 11; approximately 6–7 years after baseline). This represents 65.5 percent of the initial sample of Black and White participants (N = 1577). Of those who did not complete wave 11 (n = 544), 38 percent (n = 205) were lost to attrition, 18 percent (n = 97) died, and 44 percent (n = 242) returned to the study for a later follow-up session. Compared to those who did not, those who completed wave 11 had significantly higher annual household income (r = .13, p < .001) and education (r = .16, p < .001). They did not differ on any other variables examined in current analyses. Attrition did not differ by race (χ2(1) = .09, p > .10).
Written informed consent was obtained from participants prior to participation in the study. Each participant received $60 compensation to complete each in-person assessment and $20 to complete each mailed/online assessment. All procedures were approved by the Washington University institutional review board (IRB; approval no. 201102523).
Informants
Analyses include both self and informant reports of personality traits. Participants (93%) chose at least one person who knew them best to provide data about the participant’s personality. Participants had known their informants for an average of 32.5 years. Overall, 96 percent of Black participants and 95 percent of White participants matched their informant in race. The majority of White participants’ informants were significant others (52.6%), whereas Black participants’ informants were similarly distributed between significant others (34.6%) and family members (32.6%). Informants completed questionnaires about their associated participant through the mail or online. They received $30 remuneration for questionnaires completed during a follow-up in which the participant had an in-person session and $10 for all other follow-up questionnaires.
Discrimination
The Major Experiences of Discrimination Scale (MED; Kessler et al., 1999) was collected at wave 11. The MED is an eight-item measure of lifetime major experiences of discrimination across a range of life domains including housing, access to healthcare, and employment. The perceived reasons for discrimination, such as race, gender, ability status, and political affiliation, are also assessed. Discrimination events were collapsed across reasons for discrimination and were summed to form a composite variable that represented the number of life domains in which participants report being discriminated against at any point in their lifetime. Two items pertaining to the impact of discrimination (“how much has discrimination interfered with you having a full and productive life?” and “how much harder has your life been because of discrimination?”) were rated on a 4-point scale, ranging from “not at all” to “a lot.” These two items were summed to represent the impact of discrimination. Both discrimination variables (i.e. number of domains and impact) were z-scored and summed to form an overall discrimination composite variable, which represents both the pervasiveness and perceived psychological impact of discrimination.
Personality
Personality was measured using the NEO Personality Inventory–Revised (NEO-PI-R; Costa and McCrae, 1992) at wave 11. The NEO-PI-R is a widely used 240-item assessment of five personality domains: neuroticism, extraversion, openness, agreeableness, and conscientiousness. Each domain is made up of six facets. Neuroticism facets include anxiety, angry hostility, depression, self-consciousness, impulsiveness, and vulnerability. Extraversion facets include warmth, gregariousness, assertiveness, activity, excitement-seeking, and positive emotions. Openness facets include fantasy, aesthetics, feelings, actions, ideas, and values. Agreeableness facets include trust, straightforwardness, altruism, compliance, modesty, and tender-mindedness. Conscientiousness factors include competence, order, dutifulness, achievement striving, self-discipline, and deliberation.
NEO-PI-R items are rated on a 5-point scale, with responses ranging from 1 (strongly disagree) to 5 (strongly agree). Adequate reliability and validity have been shown for both clinical and community samples, including for older Black American adults (Savla et al., 2007). Cronbach’s reliabilities of NEO domains for Black participants ranged from .84 (agreeableness) to .90 (neuroticism) for self-report and from .86 (openness) to .95 (conscientiousness) for informant-report. For White participants, reliabilities ranged from .88 (agreeableness) to .94 (neuroticism) for self-report and from .91 (extraversion and openness) and .95 (conscientiousness and neuroticism) for informant-report. Self-other agreement for NEO domain scores was .46 for neuroticism, .51 for extraversion, .51 for openness, .35 for agreeableness, and .42 for conscientiousness (Lawton et al., 2011). Many studies have demonstrated that informant reports of personality traits provide significant incremental validity in the prediction of meaningful outcomes in later life (Cruitt and Oltmanns, 2017; Jackson et al., 2015). Therefore, personality variables were calculated as an average of the participant and informant scales.
Health
The RAND Short-Form 36 Health Status Inventory (HSI; Hays and Morales, 2001) is a self-report questionnaire that was used to measure health-related quality of life within physical and emotional health spheres at wave 11.
The physical health scales assess four aspects of health over the previous 4 weeks. Physical functioning items ask participants to rate how much their health has limited their functioning in daily activities. Role limitations due to physical health problems items measure whether physical problems have limited work or other regular daily activities. General health perceptions items include questions about self-rated health (ranging from “poor” to “excellent”) and general health. Pain items ask participants to rate the amount of bodily pain experienced, as well as how much this pain interfered with work and activities.
The mental health scales also span 4 weeks. Role limitations due to emotional problems assess the extent to which emotional problems have limited work or other activities. Social functioning assesses the extent to which emotional problems interfered with social activities. Emotional well-being assesses emotional state. Energy/fatigue assesses the extent to which participants felt energetic and tired. Self-reported physical health and self-reported mental health were each calculated as an average of the items used to create their subscales. Cronbach’s reliabilities were .83 for the physical health score and .78 for the mental health score.
Statistical analyses
Structural equation modeling was utilized to conduct path analyses with lavaan in R (Rosseel, 2012). Race was included as an endogenous variable. Discrimination, personality traits, and health were included as exogenous variables, with health serving as the outcome. The model we tested is a serial mediation model in which race predicts discrimination, which predicts personality, which in turn predicts the health outcome. Individual personality traits were examined in separate models. Models were estimated using full information maximum likelihood, enabling the use of all available information to compute the models despite missing data. We report standardized estimates and 95% confidence intervals (CIs), which were estimated using bootstrapping.
For those personality domains for which there was a significant indirect effect, we also examined the mediating roles of each of their facets (e.g. trust from agreeableness). Given that the mediators (i.e. discrimination and personality) were assessed at the same time-point, for models with a significant indirect effect we reversed the mediators to gain more information about the directionality of effects. Education, income, and gender (measured at wave 1) were included as covariates in all models.
Results
Demographic characteristics and bivariate correlations
Demographic characteristics of Black and White participants, as well as descriptive statistics for continuous variables can be seen in Table 1. Briefly, Black participants scored significantly higher on the discrimination composite and were more likely to report having experienced discrimination in at least one life domain. Black and White participants did not differ significantly on neuroticism, conscientiousness, or extraversion. There were significant racial differences in agreeableness, openness, physical health, and mental health, with Black participants scoring lower than White participants. Black participants reported significantly more racial (t = −15.71, d = −0.84, p < .001) and nonracial (t = −12.29, d = −0.66, p < .001) discrimination compared with White participants (not displayed in table).
Demographic characteristics and descriptive statistics by race.
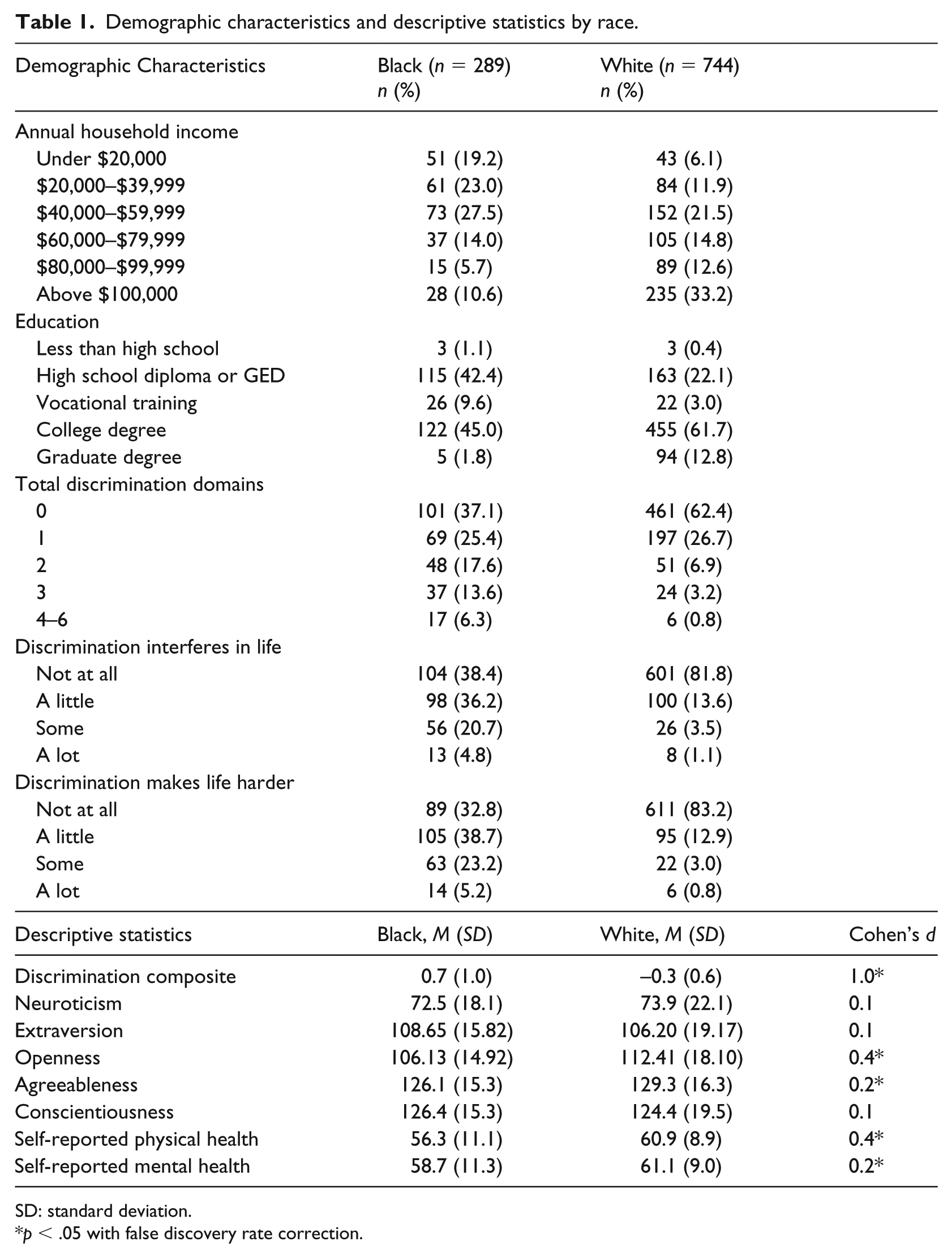
SD: standard deviation.
p < .05 with false discovery rate correction.
Bivariate correlations by race are shown in Table 2. For Black participants, discrimination was associated with higher openness and poorer mental health; for White participants, discrimination was associated with higher neuroticism and openness, and lower conscientiousness and agreeableness. Higher neuroticism and lower extraversion were associated with poorer mental and physical health for both racial groups. We did not conduct indirect effects analyses with extraversion or openness given their non-significant associations with discrimination and/or health.
Bivariate correlations among variables by race.
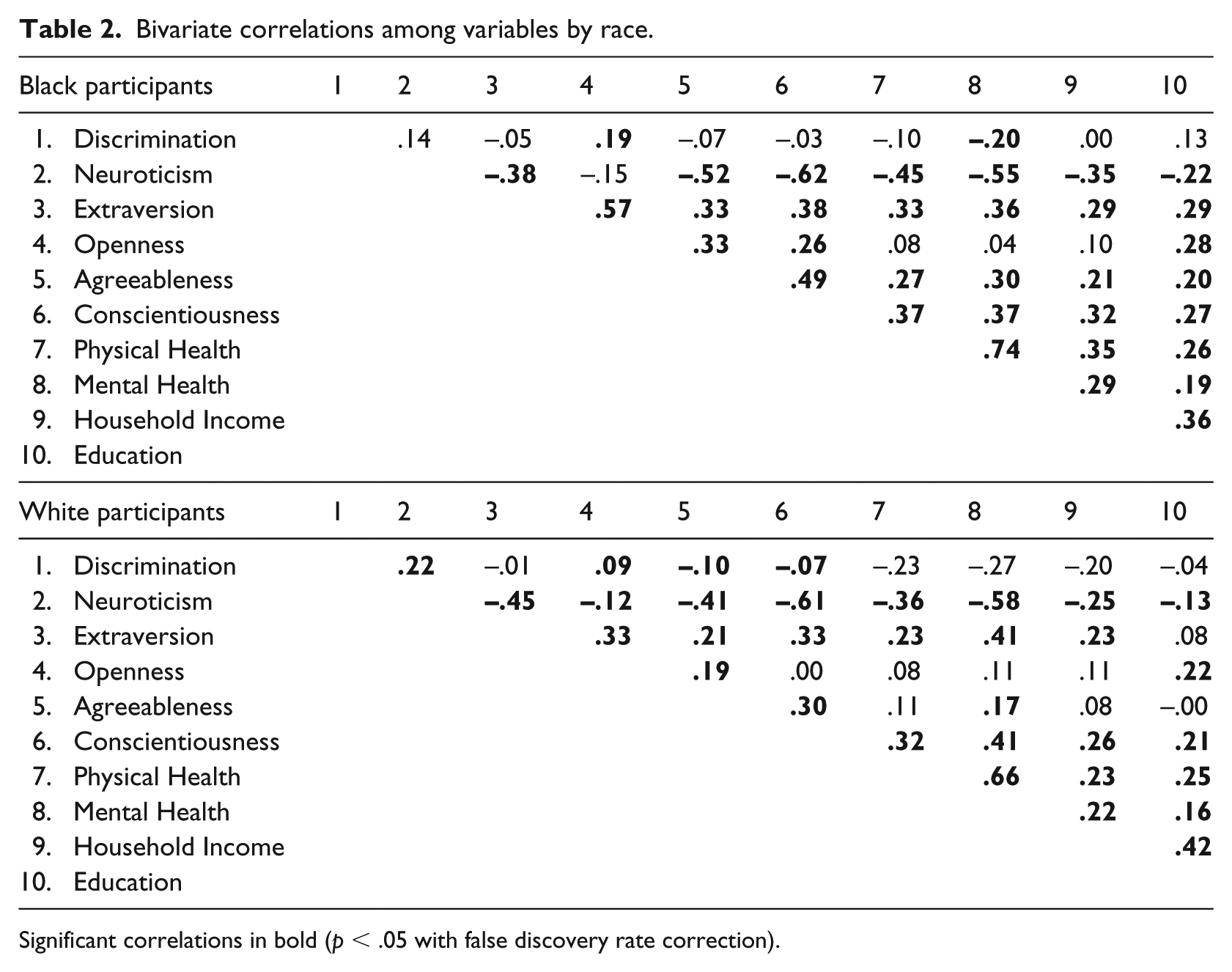
Significant correlations in bold (p < .05 with false discovery rate correction).
Do discrimination and personality traits explain racial health disparities?
Neuroticism
Indirect effects and 95% CIs and p-values for the indirect effects of personality domains and facets are displayed in Table 3. We found support for our main hypothesis, such that there were significant indirect effects of race on mental health and physical health through discrimination and neuroticism (i.e. a × b1 × b2) controlling for education, income, and gender (Figure 1). Black participants reported more discrimination, which was associated with higher neuroticism, which in turn was linked with poorer self-reported physical health and mental health. The total and direct effects of race on mental health were non-significant. The total and direct effects were significantly negative for physical health, such that Black race was associated with poorer physical health overall (total effect) which remained after accounting for discrimination, neuroticism, and covariates (direct effect). When personality and discrimination were reversed in the model, the indirect effects were not significant for mental or physical health (effects = .00, 95% CI = [−.00, .00], p > .10).
Indirect effects of race on health through discrimination and personality domains and facets.
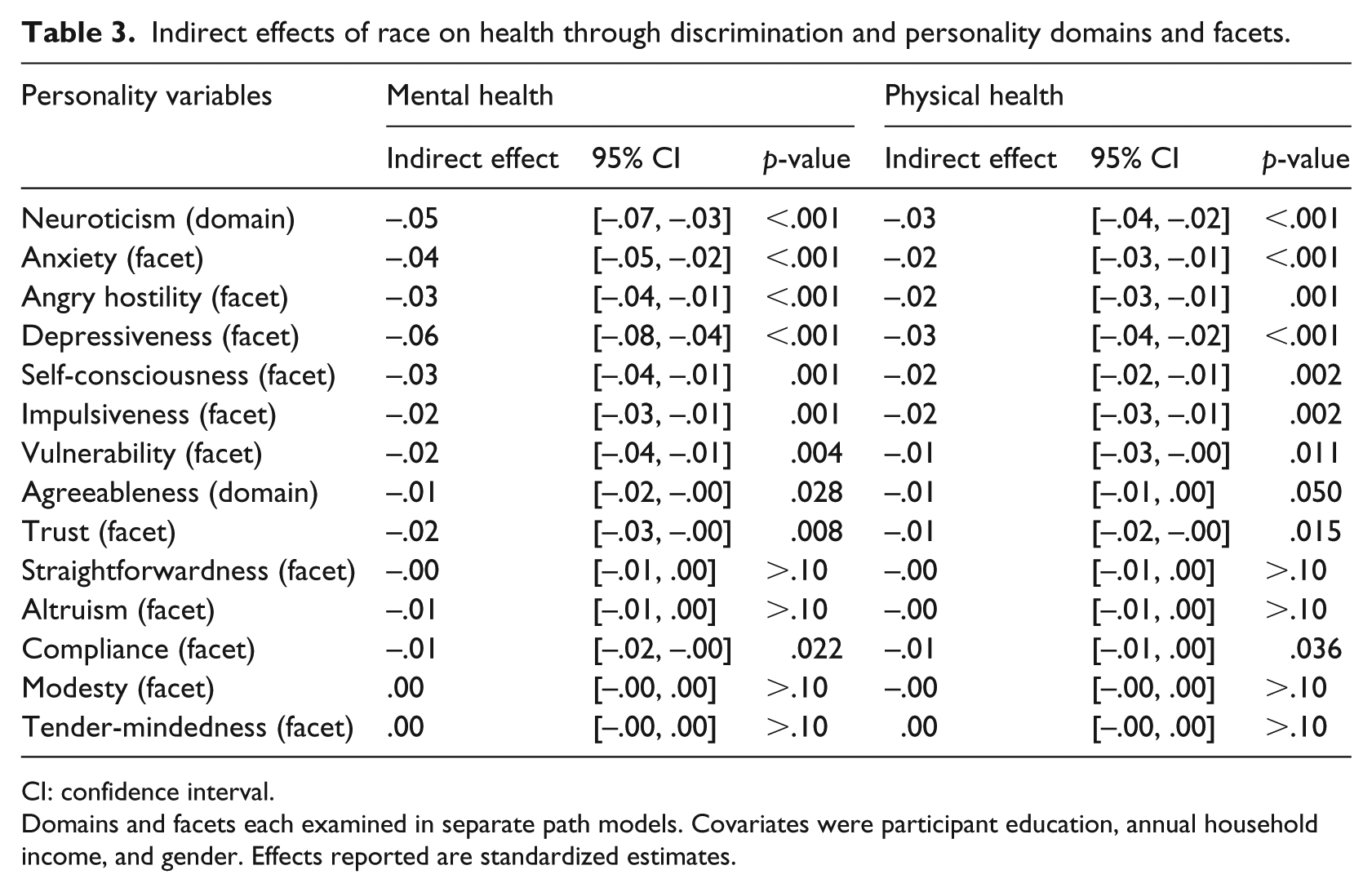
CI: confidence interval.
Domains and facets each examined in separate path models. Covariates were participant education, annual household income, and gender. Effects reported are standardized estimates.
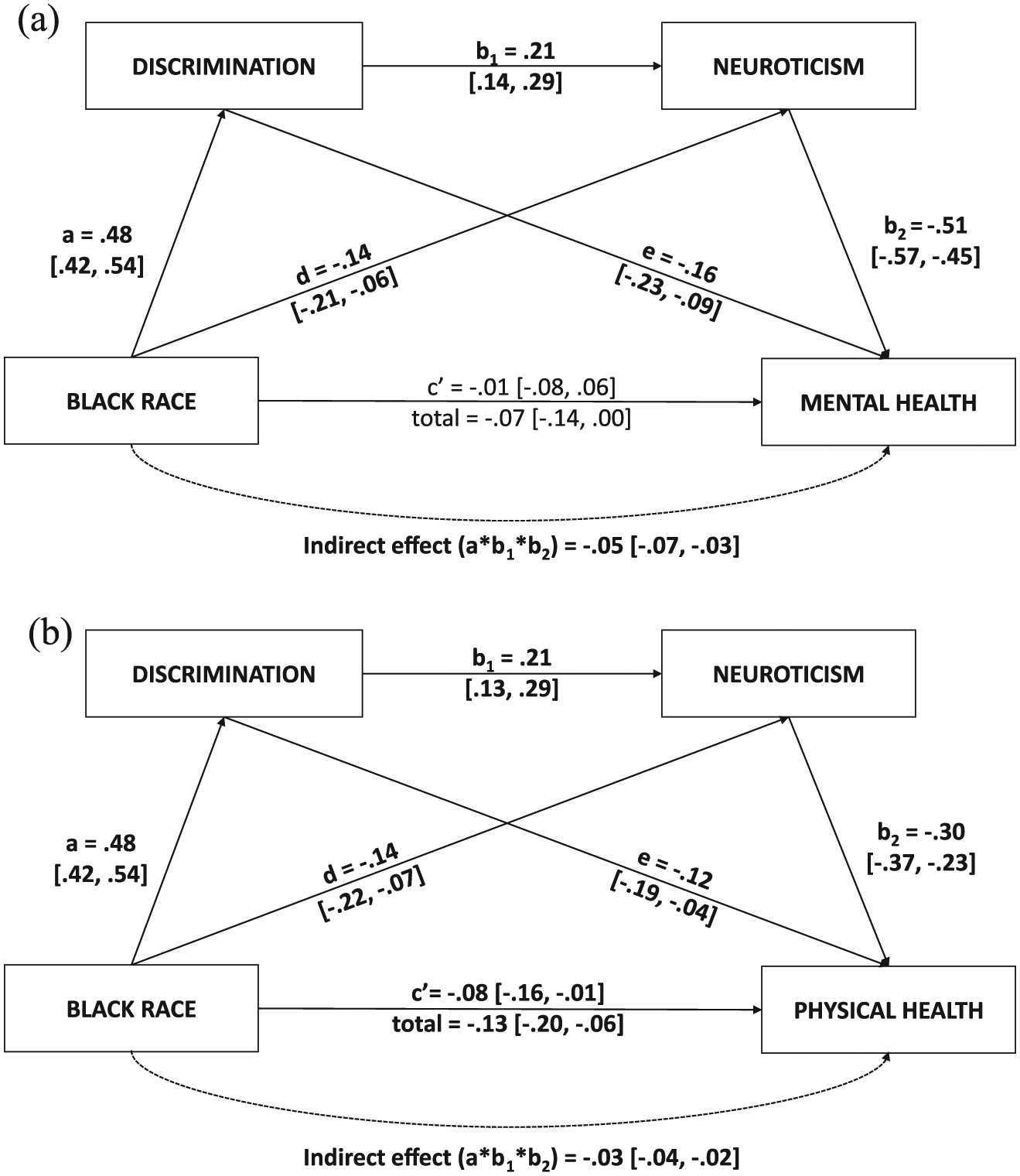
Structural equation models of the indirect effects of race on (a) mental health and (b) physical health through discrimination and neuroticism.
The indirect effect was significant across each neuroticism facet for both physical and mental health (Table 3). However, when all neuroticism facets were included simultaneously as parallel mediators, the indirect effect was only significant through discrimination and depressiveness for mental health (−.05, 95% CI = [−.07, −.03], p < .001), and through discrimination and impulsiveness for physical health (−.01, 95% CI = [−.02, −.00], p = .02).
Agreeableness
Partially supporting hypotheses, there was a significant indirect effect of race on mental health and a marginally significant indirect effect of race on physical health through discrimination and agreeableness (i.e. a × b1 × b2) controlling for education, income, and gender (Figure 2). Black participants reported more discrimination, which was associated with lower agreeableness, which in turn was associated with poorer mental and physical health. The total effect of race on mental health was significantly negative, such that Black race was associated with poorer mental health; however, the direct effect was significantly positive, such that Black race was associated with better mental health after accounting for discrimination, agree-ableness, and covariates. For physical health, only the total effect was significantly negative, whereas the direct effect was non-significant. As with the neuroticism models, when the order of agreeableness and discrimination were reversed, the indirect effect was not significant for mental health or physical health (effects = −.00, 95% CI = [−.01, .00], p > .10).

Structural equation models of the indirect effects of race on (a) mental health and (b) physical health through discrimination and agreeableness.
Facet-level analyses suggested that there were significant indirect effects through trust and compliance (Table 3). Higher discrimination was associated with lower trust and compliance, both of which were associated with lower physical and mental health. When trust and compliance were included in the mediation model simultaneously, the indirect effect was only significant through discrimination and trust for mental health (−.02, 95% CI = [−.03, −.01], p = .009). There was no uniquely significant indirect effect through trust or compliance for physical health, though the total indirect effect was significant (−.01, 95% CI = [−.02, −.00], p = .017).
Conscientiousness
The indirect effects of race on physical health (−.01, 95% CI = [−.02, −.00], p > .10) and mental health (−.01, 95% CI = [−.02, .00], p > .10) through discrimination and conscientiousness were not significant (Figure 3). Higher conscientiousness was associated with Black race and better physical and mental health but was not significantly associated with discrimination. The total effect of race on mental health was not significant, whereas the total effect was significantly negative for physical health (i.e. Black participants reported poorer physical health). The direct effects of race were non-significant for both health outcomes. Results were similar when the mediators were reversed.
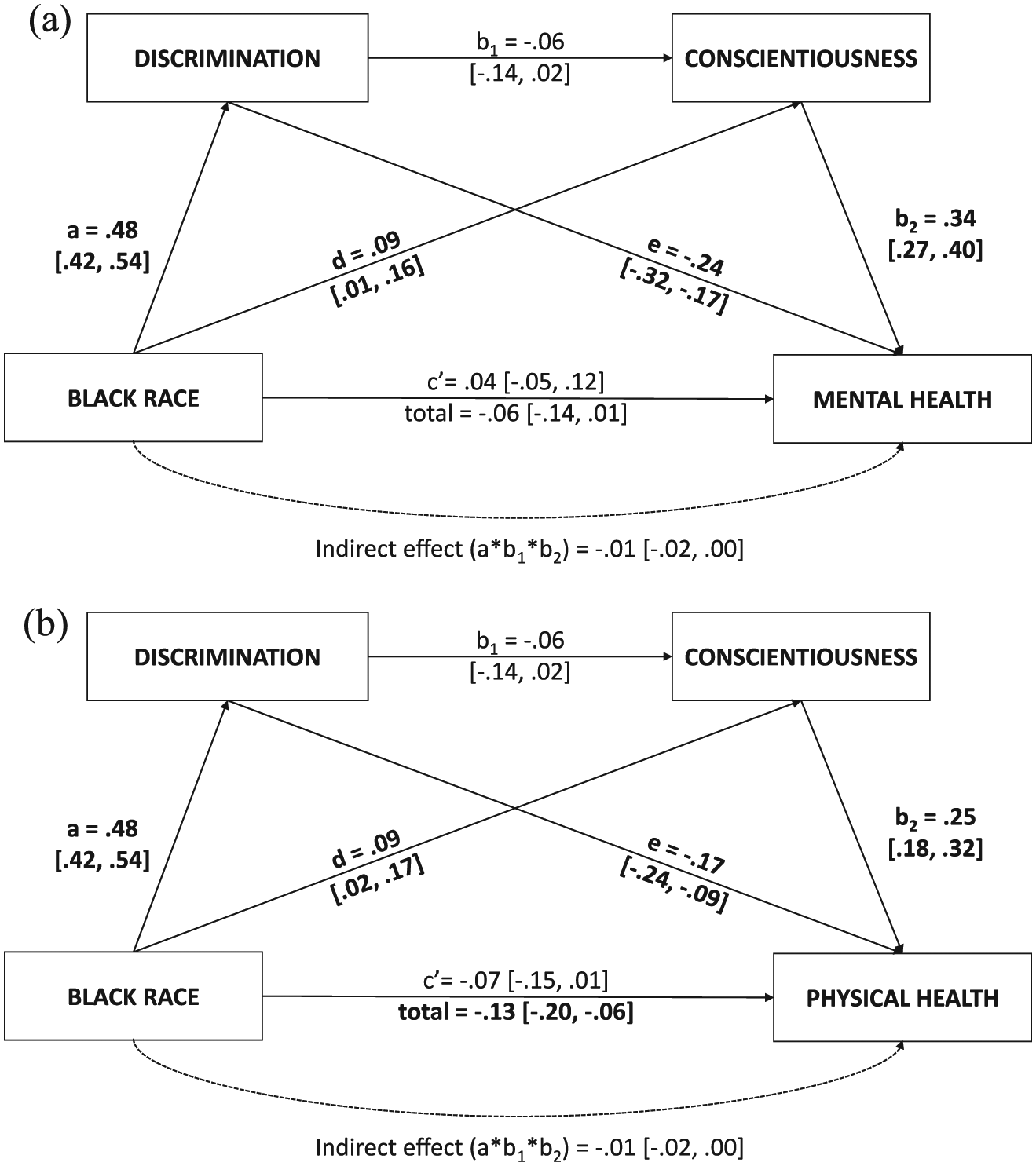
Structural equation models of the indirect effects of race on (a) mental health and (b) physical health through discrimination and conscientiousness.
Other indirect effects
We also examined the other two indirect effects (controlling for income, education, and gender) of race on health (1) through discrimination (a × e) and (2) through personality (d × b2). The indirect effect of race on health through discrimination controlling for neuroticism (a × e; see the figures) was significant for mental (−.08, 95% CI = [−.11, −.04], p < .001) and physical health (−.06, 95% CI = [−.10, −.02], p = .002). The indirect effect of race on health through discrimination controlling for agreeableness was significant for mental health (−.12; 95% CI = [−.16, −.08], p < .001) and physical health (−.09, 95% CI = [−.13, −.05], p < .001). In both cases, Black participants reported more discrimination, which was associated with poorer mental and physical health.
The indirect effects of race on health through neuroticism and conscientiousness, controlling for discrimination (d × b2; see the figures), were significant for mental health (neuroticism = .08, 95% CI = [.03, .11], p < .001; conscientiousness = .032, 95% CI = [.00, .06], p = .03), and physical health (neuroticism = .04, 95% CI = [.02, .07], p = .001; conscientiousness = .02, 95% CI = [.00, .04], p = .025). Black participants reported lower neuroticism and higher conscientiousness, which were each associated with better mental and physical health. In other words, lower neuroticism and higher conscientiousness among Black participants was associated with better health when discrimination was equivalent between racial groups. The indirect effects through agreeableness controlling for discrimination were not significant for mental health (−.01, 95% CI = [−.02, .01], p > .10) or physical health (−.01, 95% CI = [−.02, .01], p > .10), suggesting that the effects of agreeableness on racial disparities in health are specifically connected to discrimination.
Main analyses examined discrimination collapsed across forms (e.g. race, gender, age). Analyses considering indirect effects through racial discrimination and personality revealed similar findings. When all neuroticism and agreeableness personality facets were considered simultaneously, there were significant indirect effects through discrimination and depressiveness (−.06, 95% CI = [−.08, −.03], p < .001) and trust (−.02, 95% CI = [−.03, −.01]) for mental health, and impulsiveness (−.01, 95% CI = [−.02, −.00], p = .01) and trust (−.01, 95% CI = [−.02, −.00]) for physical health. Racial discrimination was not significantly correlated with extraversion, conscientiousness, or openness.
Discussion
In this sample of 1033 late mid-life adults, Black participants reported more discrimination across life domains, greater negative psychological impact of discrimination, and lower physical and mental health than White participants. Black participants also reported lower openness and agreeableness. We found support for our main hypothesis that race exerts an indirect effect on self-reported physical and mental health via discrimination and personality traits. Specifically, Black participants reported greater lifetime discrimination, which was associated with higher neuroticism and lower agreeableness, both of which were associated with poorer physical and mental health, controlling for education, income, and gender. These findings are in line with previous research suggesting that discrimination is associated with changes in neuroticism and agreeableness over time (Sutin et al., 2016) and that discrimination and personality traits are associated with health and health disparities (Hampson, 2012; McClendon et al., 2019; Williams et al., 2012).
Facet-level results suggest that racial health disparities are partly explained by associations between discrimination and negative affect broadly, given that results replicated across all facets of neuroticism. However, when all facets were included in one model, only depressiveness emerged as a significant mediator for mental health, and impulsiveness was the only significant mediator for physical health. Research on health effects of discrimination supports a link between discrimination and depression symptoms as well as major depressive disorder (Lewis et al., 2015). The personality facet of depressiveness reflects a general and pervasive tendency to experience a depressed mood. It is associated with and increases risk for major depression, but it represents an interpersonal, affective, and cognitive style rather than an episodic mental illness. Current results suggest that in contributing to racial disparities in mental health, discrimination has its strongest impact on feelings of sadness, hopelessness, and low self-worth. Discrimination is uncontrollable, often unpredictable, and sends the message to its victims that they are unworthy due to their social group membership, which is often experienced as an essential part of their identity (Schmitt and Branscombe, 2002). Thus, one or more major experiences of discrimination may have a significant negative impact on an individual’s sense of self-worth and optimism, leading to poorer mental health outcomes.
Individuals scoring high on impulsiveness tend to have trouble resisting cravings and react impulsively to unpleasant emotions. The facet of impulsiveness has been linked to poor health behaviors such as unhealthy eating and alcohol problems, as well as mental disorders characterized by impulsive risky behavior such as borderline personality disorder (Iacovino et al., 2014b; Villafuerte et al., 2013). Current findings suggest that experiences of discrimination may increase the use of unhealthy or risky coping behaviors to manage associated physiological and psychological stress responses, which in turn have damaging effects on physical health (Jackson et al., 2010).
Current findings provide compelling evidence about the directionality of discrimination-personality associations. A recent study demonstrated an association between microaggressions, a form of discrimination involving subtle slights and insults, and a neuroticism-related construct (i.e. negative affectivity) but was not able to elucidate the direction of this association (Williams et al., 2018). Some researchers have suggested that discrimination and microaggressions may be related to negative mental health outcomes due to neuroticism influencing perceptions of discrimination, and call into question efforts to reduce the occurrence of microaggressions in settings such as college campuses (Haidt, 2017; Lilienfeld, 2017). Our findings argue against this assertion and rather suggest that discrimination experiences predict higher levels of neuroticism, rather than neuroticism influencing higher reports of discrimination. Thus, reducing discrimination may have positive benefits for improving both neuroticism and health outcomes.
As predicted, trust appeared to be the most important agreeableness facet in connecting discrimination to racial health disparities. In the FFM of personality, trust represents an individual’s tendency to see others as honest, trustworthy, and having good intentions and represents a general interpersonal style that pervades across life domains. Black Americans are consistently found to endorse lower levels of various types of trust (e.g. interpersonal, health care-related, in the dominant culture) compared with Whites (Armstrong et al., 2013; Lee and Lin, 2011; Whaley, 2001). Current findings suggest that trust is eroded among Black Americans in part in reaction to experiences with discrimination. Because of discrimination, individuals may be less likely to trust the health care system and its providers, leading to reduced health care use as well as decreased quality and effectiveness of health care. This may be particularly impactful on mental health care, given the more robust role of trust in mediating mental health disparities. Indeed, research shows that major experiences of discrimination are associated with underutilization of needed health care among Black Americans (Burgess et al., 2008). Furthermore, low trust may lead to attenuated benefits from health-buffering factors such as social support (Hill et al., 2014; Lincoln et al., 2003; Mortenson, 2009; Park et al., 2013).
Notably, after accounting for covariates, discrimination, and agreeableness, Black race was associated with better mental health. This is in line with past research finding that controlling for perceived discrimination increases the Black advantage in mental health relative to Whites (Keyes, 2009). This suggests that in the absence of discrimination, Black Americans would not have a disparity in mental health compared with White Americans. This provides further evidence that discrimination robustly damages the mental health of Black Americans, partly through its impact on agreeableness, contributing to racial health disparities. Similarly, Black race was associated indirectly with better mental and physical health through higher conscientiousness and lower neuroticism, controlling for discrimination and covariates. Thus, Black Americans may possess levels of specific personality traits that, in the absence of disproportionate discrimination, would protect their health and minimize disparities.
The current study has some limitations. Analyses were cross-sectional, and thus our indirect effects models assess only the plausibility of a mechanistic path as we are not able to measure the impact of discrimination on changes in personality. Past longitudinal research by Sutin and colleagues (2016) suggests that discrimination does predict increases in neuroticism and declines in agreeableness. In addition, when we reversed the mediators so that personality predicted discrimination in our models, we found that the indirect effect was not significant. Taken together, this provides preliminary evidence that discrimination contributes to racial disparities in physical and mental health by influencing neuroticism and agreeableness. Longitudinal research is needed to bolster evidence for this hypothesis (Maxwell and Cole, 2007).
Another limitation is that our sample comprised older adults and so current findings may not generalize to other age cohorts. The geographic location of participants in this study may also alter the magnitude or direction of connections among our variables of interest, given the striking, overt, and widely publicized pervasiveness of racial discrimination in the St. Louis metropolitan area (Hudson et al., 2016). Given past research showing associations among the individual pathways explored in our study, however, it is likely that current findings would be replicated in other regions and age cohorts, but research is needed to support this. Furthermore, reporting bias, which may particularly affect racial minority participants’ disclosures of discrimination, personality, and health may also contribute to underestimation of effects.
An additional limitation are our measures of personality and discrimination. We measure personality traits, which are generally stable across life domains but which can vary in intensity as a function of context, such as the racial identity of the person with whom an individual is interacting. It will be an important priority of future research to understand the relative contributions of various forms of, for example, trust and mistrust (e.g. cultural mistrust, trust in healthcare providers) to health disparities. In addition, we utilized a measure capturing acute discrimination events which reflect institutional-level prejudice (e.g. education, housing, police), rather than measuring everyday discrimination or microaggressions, which reflect relational or interpersonal discrimination. Though measuring the frequency of acute events may tap into the chronicity of discrimination, our models may still have underestimated the magnitude of the impact of the full range of discrimination experiences on personality and health disparities. Nonetheless, major discrimination events are likely to shape access to material resources and opportunities as well as health care use, which have robust effects on health (Burgess et al., 2008).
Conclusion
Discrimination is a common experience among Black Americans, and such events are often repeated, chronic, and uncontrollable. These experiences can instill in individuals a sense of powerlessness, fear, or worthlessness, leading to increases in negative emotions such as depression and mistrust (Carter, 2007). Findings suggest that the greater pervasiveness and perceived negative impact of discrimination among Black Americans drives inequalities in cognitive, emotional, and behavioral responses, which in turn contributes to their disproportionately poorer health outcomes.
In addition to working to end discrimination, psychologists can play a crucial role in developing interventions that diminish the impact of discrimination on the health of Black Americans and individuals from other marginalized groups. Current findings suggest that depressiveness, impulsiveness, and mistrust may be the most potent intervention targets for reducing the impact of discrimination on. Research is needed to ascertain the various contexts in which these traits are most pronounced and the most effective strategies for reducing their impact on health; for example, mistrust may be adaptive in certain circumstances and not others, and interventions would benefit from helping individuals make these distinctions.
Research suggests that social support, healthy racial identity, and effective coping with discrimination-related stress can reduce its impact on negative outcomes (Carlson et al., 2018; Wang et al., 2015), likely by influencing intermediate factors such as personality traits (Jackson et al., 2019). Providing evidence-based group interventions that focus on ameliorating negative consequences of discrimination through social support, reducing internalized racism, and increasing effective emotion-coping may be particularly beneficial for promoting health equity (Carlson et al., 2018; Hudson et al., 2016). In addition, healthcare providers will be able to more effectively treat individuals who experience discrimination by addressing mistrust through improved cultural competence training and provider–patient communication.
Footnotes
Authors’ note
Juliette McClendon, PhD, is now affiliated with the National Center for PTSD/VA Boston Healthcare System, Women’s Health Sciences Division and the Boston University School of Medicine Department of Psychiatry. Juliette McClendon was formerly Juliette M. Iacovino.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by National Institutes of Health grants NIA 1F31AG048729, NIA 3R01AG045231, NIA 3R01AG045231-01A1S1, and NIMH R01MH077840.