
Abstract
Little research has examined the relationship between self-concept and depressive and anxiety symptoms and whether this is moderated by illness acceptance in individuals with multiple sclerosis. Results of an online self-report survey completed by 515 individuals with multiple sclerosis revealed that self-concept was negatively associated with depressive and anxiety symptoms with illness acceptance moderating the association such that individuals with highest self-concept and illness acceptance had the lowest levels of depressive and anxiety symptoms. Findings lend support to psychological interventions that focus on increasing illness acceptance and fostering positive self-concept in individuals with multiple sclerosis.
Introduction
Multiple sclerosis (MS) is an incurable degenerative neurological disease involving an unsteady clinical course with unpredictable wide ranging and potentially disabling symptoms. In addition to the physical consequences, receiving an MS diagnosis and experiencing MS symptoms and progression of the disease have been associated with depression and anxiety (Giordano et al., 2011). The lifetime prevalence of depression has been reported being up to 54 per cent and clinical levels of anxiety found to affect up to 45 per cent of MS patients (Beiske et al., 2008; Wood et al., 2013). Levels of depression and anxiety among individuals with MS have been found to be higher compared to individuals with other chronic health conditions (Kessler et al., 2003), suggesting the need to examine factors contributing to increased levels of depressive and anxiety symptoms in those with MS.
While rates of depression and anxiety have been established within an MS population, limited research has been conducted to explore the factors that may explain the variation in levels of depression and anxiety between individuals with MS. The extent to which individuals with MS experience symptoms of depression and anxiety may be due to their level of illness acceptance which has been defined as a process of internalising the functional implications of the condition into one’s self-concept and making behavioural adaptations that encompass the impairment of the condition into the individual’s life. Adaptively adjusting and incorporating the illness into their lives involves coming to terms with the long-term effects of a chronic illness, which is likely to worsen over time. Individuals are able to maximise their physical and mental health within the context of impairment and limitations as a result of their illness (Stuifbergen et al., 2008).
From the research available, negative associations have been found between illness acceptance and measures of depression and anxiety in those with MS (Pakenham and Fleming, 2011; Wright and Kiropoulos, 2017), suggesting that it can be a factor that can be targeted in interventions for depression and anxiety for this group. Relatedly, a recent study found significant reductions in levels of depressive and anxiety symptoms and higher levels of illness acceptance in individuals who were newly diagnosed with MS who undertook a tailored 8-week cognitive behavioural therapy programme for depression and anxiety (Kiropoulos et al., 2016).
Self-concept is defined as an individual’s perception of their identity, adjustment, social skills and status, self-fulfilment, physicality, morality and associated level of self-esteem (Fitts and Warren, 1996). Self-concept has been associated with subjective well-being of individuals and changes in a person’s mood and behaviour (Halberstadt et al., 1996). Positive self-concept is viewed as an essential component of mental health (Taylor and Brown, 1988). Research has found that self-esteem, a component of self-concept, is linked to happiness (Cheng and Furnham, 2004), high positive affect and low negative affect (Orth et al., 2012), and to lower levels of depression (Orth et al., 2009). Relatedly, research into ‘disability identity’ which involves affirming one’s status as a person with a disability and incorporating that into one’s identity has also been found to predict lower depressive and anxiety symptoms in individuals with MS (Bogart, 2015).
In contrast, negative self-concept has been linked strongly to increased risk for major depressive and anxiety disorders, substance abuse and lower quality of life (Pelkonen et al., 2008; Trzesniewski et al., 2006; Vickery et al., 2005), with a recent meta-analysis finding a robust relationship between low self-esteem and depression and anxiety (Sowislo and Orth, 2013).
Negative self-concept has been found to be related to depressive and anxiety symptoms in individuals with MS (Wright and Kiropoulos, 2017) and to an increase in MS-related symptoms and the progression of the disease (Jopson and Moss-Morris, 2003). Qualitative studies investigating self-concept in individuals with MS have found that those diagnosed and living with MS reported changes in the way they perceive themselves and their perceptions of how they are viewed by others, changes in their ability to undertake roles and to participate in relationships (Irvine et al., 2009; Mozo-Dutton et al., 2012), feeling uncertainty about the future and their aspirational self (Irvine et al., 2009), experiencing negative body image (Irvine et al., 2009; Kolzet et al., 2014), feeling less attractive and self-confident and reporting higher levels of concern about sexuality and physical deficits (Pfaffenberger et al., 2011), and being concerned about disease progression and disability (Dennison et al., 2010). In contrast, positive self-concept in individuals with MS has been found to be associated with lower depressive and anxiety symptom scores, higher levels of illness acceptance and better intimate relationship quality (Bogart, 2015; Brooks and Matson, 2012; Wright and Kiropoulos, 2017) and better psychological and physical status (Wilski et al., 2016).
In summary, high levels of depressive and anxiety symptoms are found in individuals with MS. Self-concept and illness acceptance are factors that have been shown to be associated with depression and anxiety. In this study, we examined associations between self-concept, illness acceptance and symptoms of depression and anxiety in individuals with MS. We hypothesised higher illness acceptance would moderate the association between self-concept and symptoms of depression and anxiety with a significant portion of self-concept-related variance in symptoms of depression and anxiety accounted for by reduced illness acceptance.
Method
Participants and procedure
Participants with self-reported MS were recruited from online advertisements of the study on the MS Research Australia website, various MS-related online forums and the MS Society Australia newsletter, which is sent out to all members who have MS. Participants were directed to an online survey link, and once they provided informed online consent, they were able to proceed to complete the questionnaire. At the end of the questionnaire, participants were directed to debriefing information on support services. This cross-sectional study and its consent procedures were approved by the University of Melbourne University Human Ethics Committee. Participants were not compensated for their participation.
Measures
Demographic data (gender, age, relationship status, level of education, employment status and ethnic background) and medical information (length of time since MS diagnosis and first MS symptoms experienced, type of MS diagnosed, length of time since MS-related relapse, current MS, anti-depressant and anti-anxiety medication use, previous depression and/or anxiety diagnosis) were collected.
Expanded Disability Status Scale
A self-administered Expanded Disability Status Scale (EDSS-S) is a self-report measure of level of ambulation (Bowen et al., 2001). Participants were asked to estimate their ability to walk various distances with or without assistance. Scores ranged from 0 to 8. Scores of 4 and above indicate difficulties with the level of ambulation.
Acceptance of Chronic Health Conditions scale
Acceptance of Chronic Health Conditions (ACHC) scale is a 10-item scale, which measures illness acceptance and has been adapted for use with an MS population (Stuifbergen et al., 2008). Items portraying a positive attitude towards MS are reverse scored so that a higher overall score indicates greater levels of acceptance. Cronbach’s α for the total ACHC score in this study was 0.81.
Depression, Anxiety and Stress Scale
Depression, Anxiety and Stress Scale (DASS-42) is a 42-item questionnaire, which contains three subscales designed to examine the presence of depressive, anxiety and stress symptoms in the past week (Lovibond and Lovibond, 1995). Each subscale contains 14 items with a separate score generated for each scale and increased scores denoting increasing severity of symptoms. Cronbach’s α for this study is 0.95 for the Depression subscale total score and 0.89 for the Anxiety subscale total score.
Tennessee Self-Concept Scale
Tennessee Self-Concept Scale (TSCS-2) is a 82-item scale that measures an individual’s self-concept and associated level of self-esteem (Fitts and Warren, 1996). Higher scores indicate a more positive self-concept. In this study, Cronbach’s α for the total self-concept score was 0.94.
Statistical analysis
All analyses were carried out using the Statistical Package for Social Sciences (SPSS 24.0). Little’s (1988) test indicated that the missing data were missing at random and ignorable, χ2(5378) = 1813.03, p = 1.00. To test our hypothesis that self-concept would be associated with level of depressive and anxiety symptoms and that these relationships would be moderated by illness acceptance, we conducted a multiple regression analysis. This regression included the main effects of both self-concept and illness acceptance and a multiplicative interaction term that assessed if the effect of self-concept varied by level of MS illness acceptance. To avoid potentially problematic high multicollinearity with the interaction term, the variables were centred and an interaction term between self-concept and illness acceptance was created (Aiken and West, 1991). Additional regression analyses were conducted to include level of ambulation as a potential confounding covariate.
Results
Descriptive statistics
The sample consisted of 515 adults with self-reported MS, with ages ranging from 18 to 72 years (M = 42.10 years, SD = 10.95), with the majority being female (87.6%) and having 7.38 years since diagnosis. Means, standard deviations and ranges for all study variables are shown in Table 1.
Demographics and characteristics of the study sample.
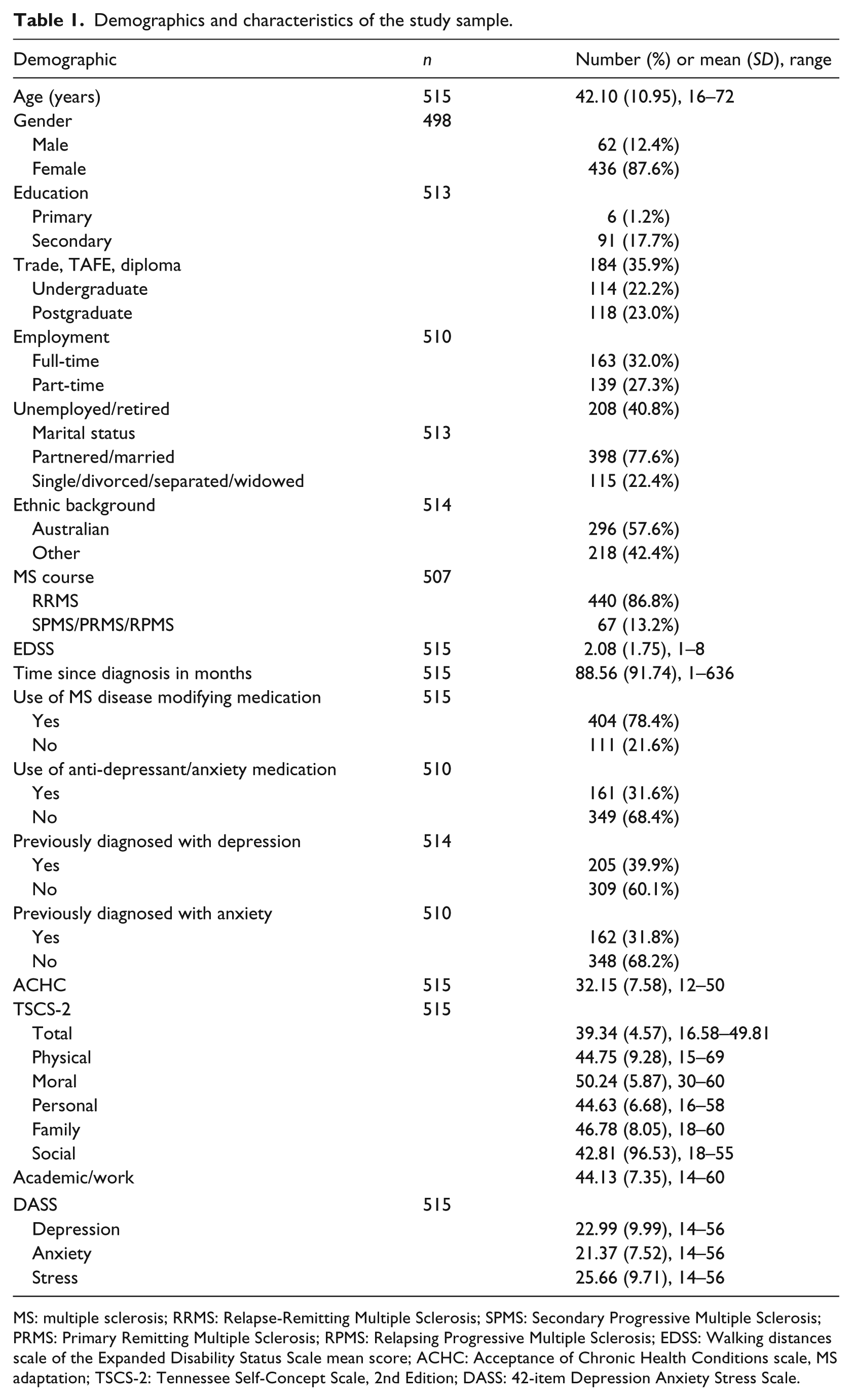
MS: multiple sclerosis; RRMS: Relapse-Remitting Multiple Sclerosis; SPMS: Secondary Progressive Multiple Sclerosis; PRMS: Primary Remitting Multiple Sclerosis; RPMS: Relapsing Progressive Multiple Sclerosis; EDSS: Walking distances scale of the Expanded Disability Status Scale mean score; ACHC: Acceptance of Chronic Health Conditions scale, MS adaptation; TSCS-2: Tennessee Self-Concept Scale, 2nd Edition; DASS: 42-item Depression Anxiety Stress Scale.
Consistent with our hypotheses, there was a significant correlation between higher level of self-concept and lower level of depressive, r = –.64, p < .001, and anxiety, r = –.53, p < .001, symptoms. There was also a significant correlation between higher levels of self-concept and higher levels of illness acceptance, r = .30, p < .001, in our sample of individuals with MS. In addition, there was a significant correlation between higher level of illness acceptance and lower level of depressive, r = –.41, p < .001, and anxiety, r = –.33, p < .001, symptoms. Table 2 presents the correlations between demographic, MS illness variables, self-concept, illness acceptance and depressive and anxiety symptoms.
Correlations between demographic, MS illness variables, self-concept, MS illness acceptance and depressive and anxiety symptoms.
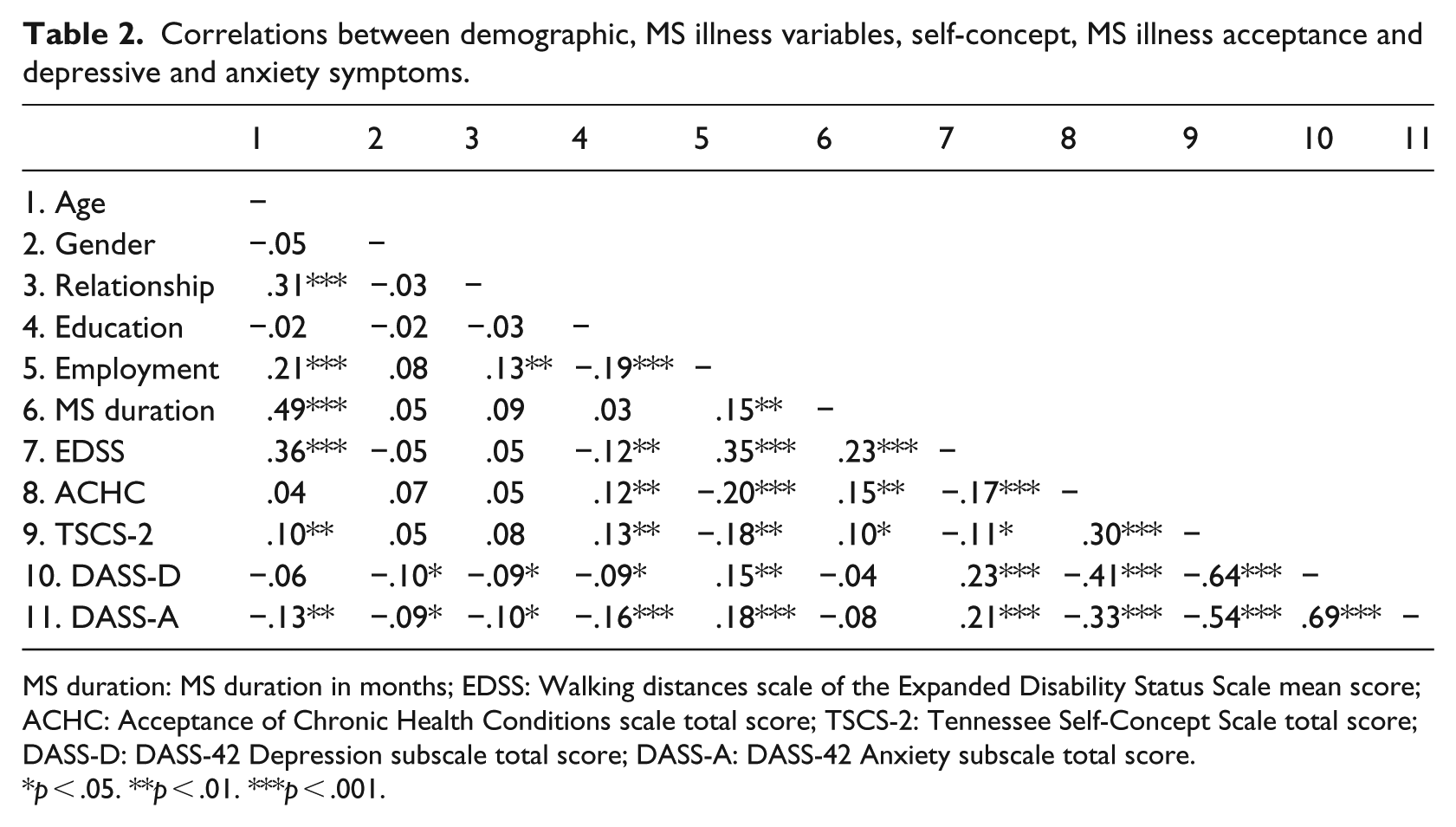
MS duration: MS duration in months; EDSS: Walking distances scale of the Expanded Disability Status Scale mean score; ACHC: Acceptance of Chronic Health Conditions scale total score; TSCS-2: Tennessee Self-Concept Scale total score; DASS-D: DASS-42 Depression subscale total score; DASS-A: DASS-42 Anxiety subscale total score.
p < .05. **p < .01. ***p < .001.
Hypothesis testing
A moderated linear regression was used to examine the main effects of self-concept and illness acceptance on depressive symptoms, and to investigate whether the relationship between self-concept and depression was moderated by participant illness acceptance. The overall model accounted for a significant proportion of variance in depression, R2 = .48, F(3, 511) = 160.04, p < .001. Both self-concept, t(514) = –8.36, p < .001, and illness acceptance, t(514) = –5.02, p < .001, directly predicted depression. Furthermore, there was evidence of moderation, with a significant interaction between self-concept and illness acceptance in predicting participant depression, t(514) = 4.01, p < .001. These results did not change when level of ambulation was included in the model.
Figure 1 illustrates the interaction by depicting the regression lines of the relation between self-concept and depressive symptoms at high, medium and low (+1 SD, mean, –1 SD) scores of the illness acceptance scale. Examination of the interaction plot showed a buffering effect that as self-concept and illness acceptance increased, level of depressive symptoms decreased. Individuals with highest self-concept and illness acceptance had the lowest level of depressive symptoms. Furthermore, there was a stronger relationship between illness acceptance and depression for participants with low self-concept compared to those with high self-concept. That is, at low self-concept, individuals who also had low illness acceptance scored higher on the depression measure compared to individuals with average and high illness acceptance, while this effect was less pronounced for individuals with medium self-concept and even further reduced for those with high self-concept.
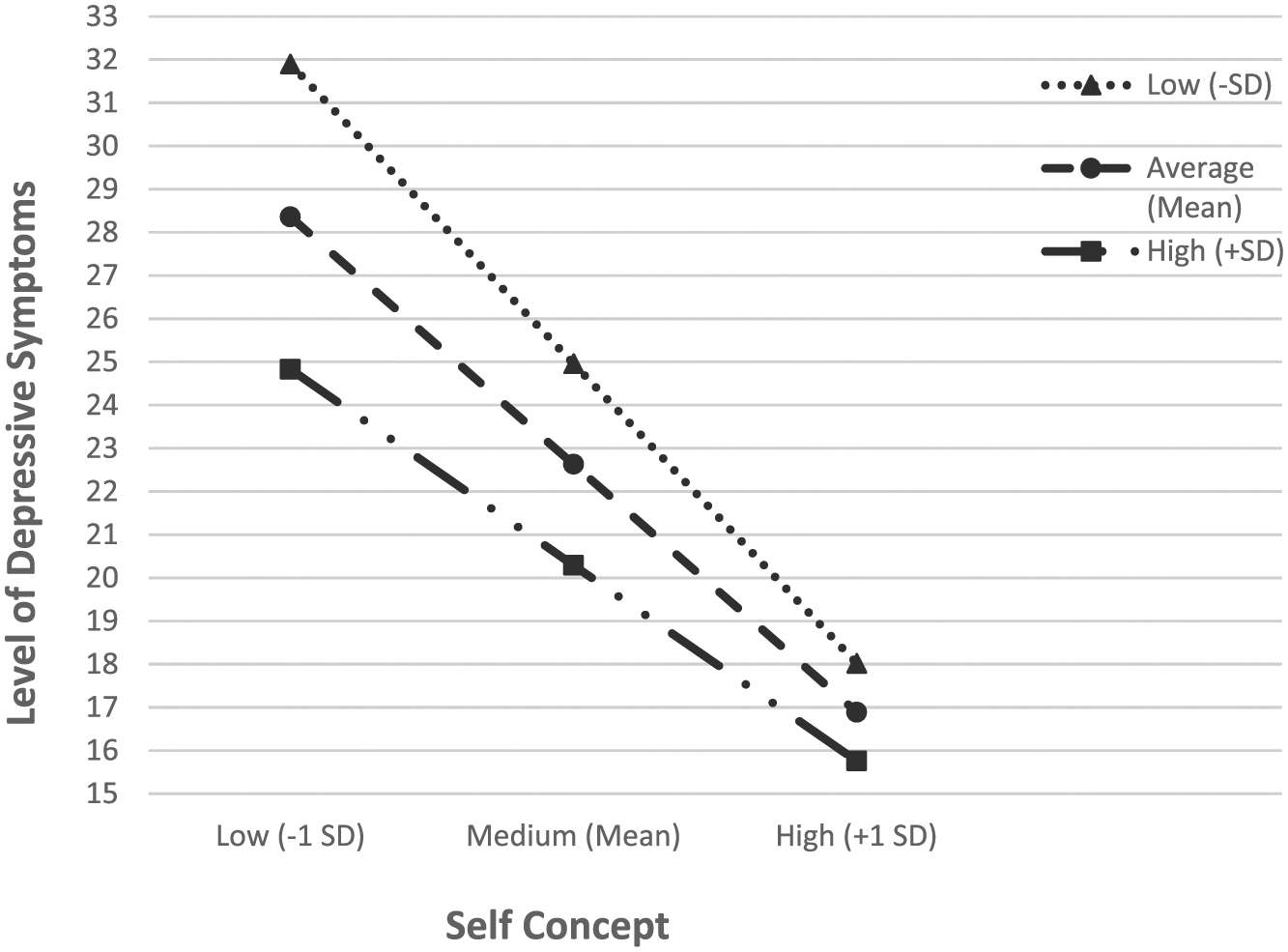
Moderating effect of MS illness acceptance.
A moderated linear regression was used to examine the main effects of self-concept and illness acceptance on anxiety symptoms, and to investigate whether the relationship between self-concept and anxiety was moderated by participant illness acceptance. The overall model accounted for a significant proportion of variance in anxiety, R2 = .32, F(3, 511) = 79.94, p < .001. Both self-concept, t(514) = –5.62, p < .001, and illness acceptance, t(514) = –3.12, p = .001, directly predicted anxiety. Furthermore, there was evidence of moderation, with a significant interaction between self-concept and illness acceptance in predicting participant anxiety, t(514) = 2.57, p = .010. These results did not change when level of ambulation was included in the model.
Figure 2 illustrates the interaction by depicting the regression lines of the relation between self-concept and anxiety symptoms at high, medium and low (+1 SD, mean, –1 SD) scores of the illness acceptance scale. Examination of the interaction plot showed a buffering effect that as self-concept and illness acceptance increased, level of anxiety symptoms decreased. Individuals with highest self-concept and illness acceptance had the lowest level of anxiety symptoms. As with depression, there was a stronger relationship between illness acceptance and anxiety for participants with low self-concept compared to those with high self-concept. That is, at low self-concept, individuals who also had low illness acceptance scored higher on the anxiety measure compared to individuals with average and high illness acceptance, while this effect was less pronounced for individuals with medium self-concept and even further reduced for those with high self-concept.
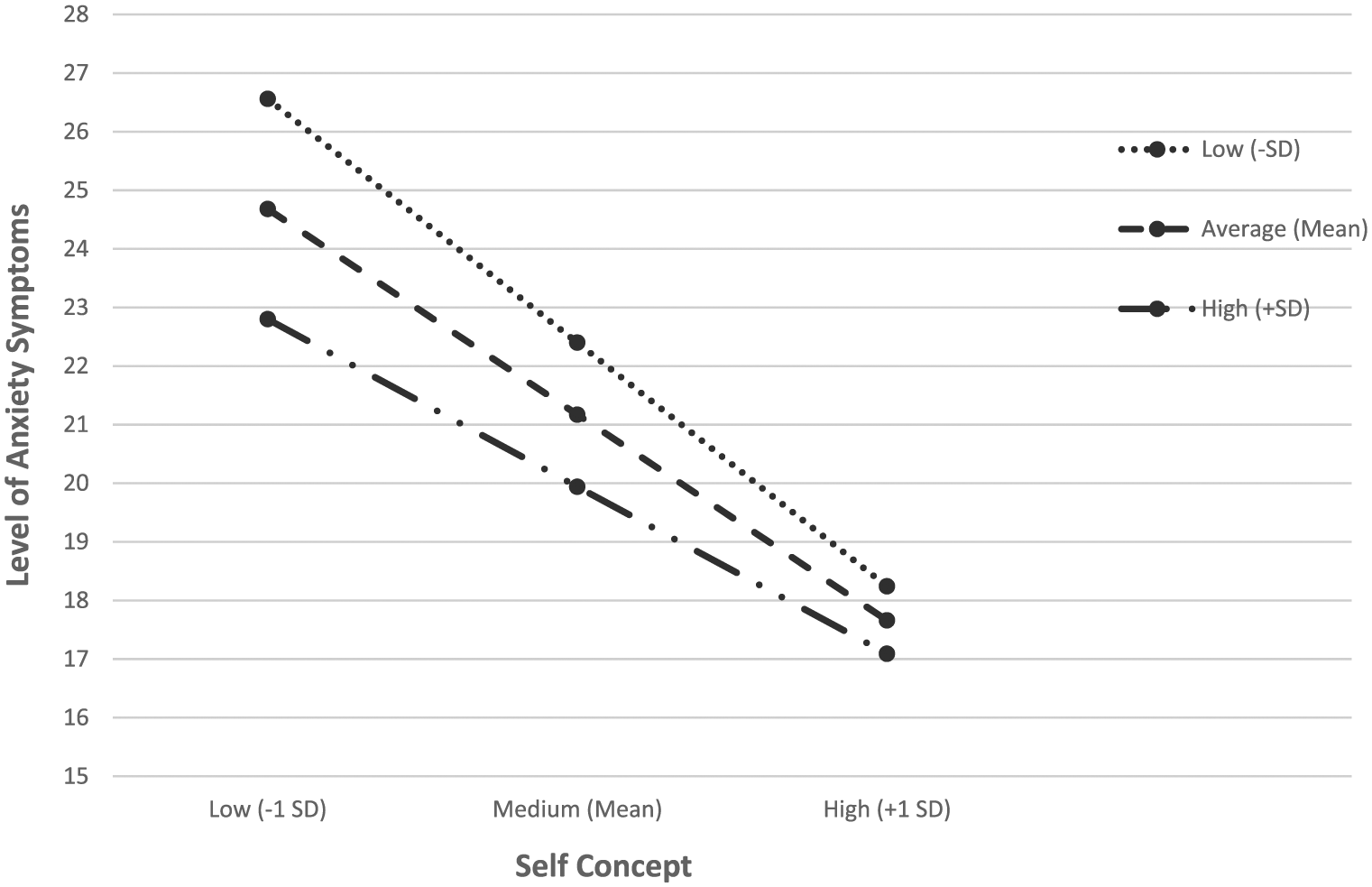
Moderating effect of MS illness acceptance.
Discussion
This study investigated the relationships between self-concept, illness acceptance and depressive and anxiety symptoms in individuals with MS. In support of our hypothesis, we found a significant association between higher levels of self-concept and lower depressive and anxiety symptoms. These findings add to the previous literature by showing that illness acceptance is one valid pathway by which self-concept impacts depressive and anxiety symptoms in individuals with MS. We found that illness acceptance moderated the association between self-concept and depressive and anxiety symptoms such that individuals with highest self-concept and illness acceptance had the lowest levels of depressive and anxiety symptoms. Furthermore, there was a stronger relationship between illness acceptance and depression and anxiety for participants with low self-concept compared to those with high self-concept. That is, at low self-concept individuals who also had low illness acceptance scored higher on the depression and anxiety measure compared to individuals with average and high illness acceptance, while this effect was less pronounced for individuals with medium self-concept and further reduced for those with high self-concept.
In our current sample, we found that self-concept is an important factor in individuals with MS with symptoms of depression and anxiety. This is in line with a meta-analysis, which found that low self-concept is associated with depression and anxiety (Sowislo and Orth, 2013). The current results also suggest that higher illness acceptance is associated with positive self-concept and lower depressive and anxiety symptoms in individuals with MS. These results are consistent and expand on previous work which found that depression and anxiety were inversely correlated with illness acceptance in individuals with MS (Pakenham and Fleming, 2011) and that illness acceptance was found to increase after individuals newly diagnosed with MS undertook an 8-week tailored Cognitive Behavioural Therapy (CBT) intervention for depression and anxiety symptoms (Kiropoulos et al., 2016). Furthermore, the current data contribute to our understanding of illness acceptance in those with MS as it indicates that high levels of illness acceptance appear to confer positive benefits to individuals with MS, who have otherwise been shown to experience higher levels of depressive and anxiety symptoms, and lower levels of self-concept than healthy individuals (Brooks and Matson, 1982; Kessler et al., 2003). The current results also provide evidence for illness acceptance as one potential pathway through which self-concept may positively affect levels of depressive and anxiety symptoms and is consistent with one study which found significant relationships between illness acceptance and self-concept (Wright and Kiropoulos, 2017).
Our findings also corroborate past evidence, which has found a relationship between illness acceptance and symptoms of depression and anxiety in individuals with MS. In one of the few studies examining acceptance of MS and its relationship to depressive and anxiety symptoms, Pakenham and Fleming (2011) found that measures of acceptance were significantly negatively correlated with measures of depressive and anxiety symptoms in an MS sample. Our results provide further support for the relationship between greater illness acceptance and lower levels of depressive and anxiety symptoms in an MS population.
There are some limitations to the current study. First, the study employed a cross-sectional design, which does not allow inferences about causality to be made. However, the current results provide the important first step in examining the causal link between self-concept, illness acceptance and depressive and anxiety symptoms in an MS population. Second, the current self-report questionnaires were completed online, and the authenticity of the subjects recruited for this study cannot be validated. However, the recruitment support of MS-related organisations was enlisted. Finally, the majority of participants (87.6%) were females who had at least a diploma as the highest level of education and reported having relapse remitting MS, which may limit the generalisability of the current results obtained. Future studies should employ a randomised control trial design with an active comparison group for the treatment of symptoms of depression and anxiety with the aim of increasing illness acceptance and fostering more positive self-concept in order to track changes in illness acceptance and self-concept in individuals with MS. In addition, this design can examine the moderating role of illness acceptance in the pathway between self-concept and symptoms of depression and anxiety longitudinally.
In conclusion, the present study makes an important contribution to the current understanding of the psychological impact of having MS. A significant relationship between self-concept and symptoms of depression and anxiety was found. Displaying high illness acceptance was associated with positive outcomes for individuals, including lower levels of depressive and anxiety symptoms and higher overall self-concept. These promising relationships indicate that illness acceptance is an important avenue of research to pursue in future psychological interventions for symptoms of depression and anxiety.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.