
Abstract
The purpose of this study was to investigate the mediating roles of trait anxiety and daily sleep quality between childhood abuse and physical health issues later in adulthood by utilizing the Midlife in the United States Study (n = 281; Mage = 56.38 in wave 2 and Mage = 62.57 in wave 3). Individuals who reported a higher level of childhood abuse reported a higher level of trait anxiety and a lower level of daily sleep quality, leading to an increase in physical health issues. The results highlight the cascading effects of childhood abuse on serious health consequences over the life span.
Childhood abuse is a prevalent and serious public health issue worldwide (Merrick and Browne, 1999). Global estimates of the prevalence of childhood abuse, based on self-report studies, suggest that 127 per 1000 individuals have experienced sexual abuse, 226 physical abuse, and 363 emotional abuse during childhood (Stoltenborgh et al., 2015). Childhood abuse is an important type of early life stress to consider given its lasting effect on the individual’s mental and physical health throughout the life course (e.g. Petruccelli et al., 2019; Springer et al., 2003; Widom et al., 2018). According to a life-course epidemiological perspective on health and physical and social hazards during early life, childhood abuse can have a long-term health and disease risk in later life (Kuh et al., 2003). Furthermore, Kendall-Tackett (2002) claims that there are four possible pathways by which childhood abuse relates to long-term physical and mental health issues based on a health psychology framework describing social, cognitive, and emotional pathways. A growing number of studies that have found the relation between childhood abuse and long-term physical and mental health issues through these four pathways, namely, behavioral (e.g. substance abuse, sleep difficulties), social (e.g. revictimization; people who experienced childhood abuse are more likely to experience abuse again), cognitive (e.g. health perceptions), and emotional (e.g. depression) pathways, are noted in the literature (Kendall-Tackett, 2002; Springer et al., 2003). However, what is less known is the interplay between different pathways (e.g. emotional and behavioral mechanisms) and their cumulative effects on long-term health issues. Therefore, this study addresses this limitation by utilizing a life-course epidemiological perspective approach to the mental and physical health of adults as a product of biological and social factors that operate across the life span (Kuh et al., 2003).
Childhood abuse is one of the main environmental risk factors in the development of trait anxiety (Schiele et al., 2016). Also, the effect of childhood abuse on sleep quality in adulthood is well documented (see Kajeepeta et al., 2015, for review). Furthermore, while sleep, as a process that restores the body’s ability to self-regulate and keeps the body’s hormones in balance, plays a vital role in physical health (e.g. physical functional limitations) over the life span (e.g. Goldman et al., 2007), individuals with higher anxiety were found to experience poorer daily sleep quality (Lockefeer and De Vries, 2013). Given the link between childhood abuse, trait anxiety, daily sleep quality, and physical health issues, we speculated that childhood abuse leads to trait anxiety, which, in turn, leads to lower daily sleep quality, resulting in physical health issues. To date, these cascading effects of childhood abuse on physical health issues through the potential, sequential mediating roles of trait anxiety (i.e. emotional mechanism) and daily sleep quality (i.e. behavioral mechanism) have not been examined. Therefore, we investigated the role of trait anxiety and daily sleep quality as the mediators connecting childhood abuse and physical health issues in later adult life.
First, we examined whether childhood abuse affected physical health issues in later adult life and then explored the potential, sequential mediating roles of trait anxiety and daily sleep quality in these relations. We hypothesized that childhood abuse would be associated with a higher level of physical health issues in later adult life. We also hypothesized that a higher level of childhood abuse would be associated with a higher level of physical health issues and that this association would be explained by a higher level of trait anxiety and a lower level of daily sleep quality.
Methods
Participants
Study data were drawn from the Midlife Development in the United States (MIDUS) study, a longitudinal demographic, psychosocial, and health data spanning early through older adulthood collected over the course of more than two decades. This study utilized MIDUS 2 (M2: wave 2) project 4: biomarkers (data collected in 2004–2009) to measure childhood abuse, trait anxiety, and daily sleep quality; and MIDUS 3 (M3: wave 3) project 1: survey (data collected in 2013–2014) to measure physical health issues in later adult life. For the purposes of this study, we restricted our sample to those who participated in the sleep study in MIDUS 2 biomarker project (P4) and completed the M3 survey. Based on this criterion, the study sample size was N = 281 (57.3% female; 95% White). The average age of participants at wave 2 is 56.38 years (standard deviation (SD) = 11.02) and the average age of participants at wave 3 is 62.57 years (SD = 11.25).
Measures
Childhood abuse
Childhood Trauma Questionnaire
The Childhood Trauma Questionnaire (CTQ) is a 28-item measure designed to measure childhood abuse. Items are rated from 1 (never true) to 5 (very often true) (Bernstein et al., 1997). CTQ total scores range from 5 to 25, with higher scores indicating greater abuse. The CTQ comprises five subscales (physical abuse, emotional abuse, sexual abuse, physical neglect, and emotional neglect) and also includes a three-item scale for one response bias subscale, minimization and denial to identify respondents likely to underreport negative events in childhood. For the current study, physical abuse, emotional abuse, and sexual abuse were employed. Internal consistency for the CTQ subscales ranged from satisfactory (i.e. physical abuse: α = .79) to excellent (i.e. emotional abuse: α = .91; sexual abuse: α = .92).
Trait anxiety
The State-Trait Anxiety Inventory
The State-Trait Anxiety Inventory (SATI) is a 40-item measure designed to measure anxiety (Spielberger, 1989). Items are rated from 1 (almost never) to 4 (almost always). SATI total scores range from 40 to 160, with higher scores indicating greater anxiety. SATI comprises two subscales (state anxiety and trait anxiety). For the current study, trait anxiety was employed. Internal consistency for trait anxiety was excellent: α = .90).
Daily sleep quality
Participants completed a daily sleep diary over 7 days. To capture daily sleep quality, participants evaluated their prior night’s sleep using four items (e.g. overall quality of your sleep last night; how well-rested you feel this morning) rated on a scale from 1 (very good) to 5 (very poor). These items follow Pittsburgh Sleep Quality Index (a longer, validated global self-report of sleep quality; Buysse et al., 1989), with the wording changed to reflect the daily level. We reverse scored these items so that higher scores represented higher daily sleep quality. In this study, we used average daily sleep quality over 7 days (α = .93).
Physical health issues
Health status was measured with the following three variables: functional limitations in activities of daily living (ADL), functional limitations in instrumental activities of daily living (IADL), and self-rated physical health (SRPH). The three-item ADL measures the extent to which participants experience limitations in basic self-care tasks such as bathing yourself and walking one block (α = .82) (Katz, 1983). The seven-item IADL measures the extent to which participants experience limitations in slightly more complex skills such as lifting or carrying groceries (α = .93) (Katz, 1983). Each item from these variables was rated on a scale from 1 (a lot) to 4 (not at all). We reverse scored these items so that higher scores reflect a greater difficulty in performing daily physical activities. SRPH is a widely used single-item measure of global health asking the following question: “In general, would you say your physical health is excellent (1), very good (2), good (3), fair (4), or poor (5)?” (e.g. Subramanian et al., 2010).
Statistical analyses
Data were analyzed using IBM SPSS statistics (version 25; IBM Corp, 2017) for descriptive statistics and bivariate correlations among main study variables including emotional abuse, physical abuse, sexual abuse, trait anxiety, daily sleep quality, ADL, IADL, and SRPH. To test mediation effects, Mplus (version 8; Muthén and Muthén, 1998–2017) was used with 5000 bootstrap samples for significance testing (Figure 1). In the current analysis, childhood abuse was treated as a latent variable with three indicators, including emotional abuse, physical abuse, and sexual abuse. The results showed these indicators were significant (all ps < .05). Physical health was also treated as a latent variable with three indicators, including ADL, IADL, and SRPH. The results showed these indicators were significant (all ps < .05). We also controlled for age in the analysis and obtained the same significant results; however, for simpler interpretations of the model, we did not include age in the final model. The absolute fit index and incremental fit index were verified in order to confirm the model fit for this study. Following Browne and Cudeck (1993) and Hu and Bentler (1999) criteria, we defined good model fit. The χ2, root mean square error of approximation (RMSEA <.08), and standardized root mean square residual (SRMR <.05) were used to verify the absolute fit index, while Tucker–Lewis index (TLI >.95) and comparative fit index (CFI >.95) were used to verify the incremental fit index. The current study demonstrated an adequate fit.
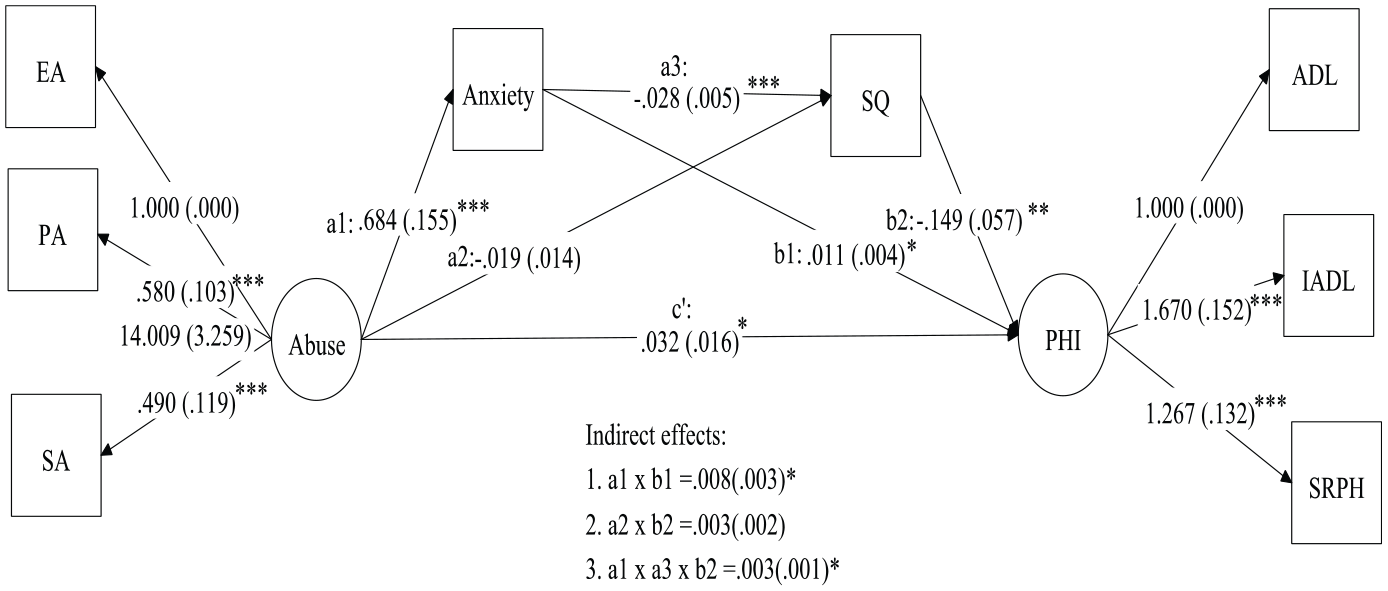
This figure reports unstandardized coefficients with standard errors in parentheses. The Mplus program examined and tested the significance of the indirect effects with 5000 bootstrapping procedures.
Results
Descriptive analyses
Descriptive statistics for the measure of total and subscale scores are presented in Table 1. The results demonstrated significant associations between all measures of interest (see Table 1).
Descriptive statistics and correlations for key study variables.

SD: standard deviation; ADL: activities of daily living; IADL: instrumental activities of daily living; SRPH: self-rated physical health.
p < .05. **p < .01. ***p < .001.
Mediation analyses
Model fit indices are as follows: χ2 = 41.67, p < .05, RMSEA = .076, TLI = .94, CFI = .97, and SRMR = .046. The results demonstrated several significant effects: (1) individuals who reported a higher level of childhood abuse reported a higher level of physical health issues in later adulthood (unstandardized coefficient (b) = .03, standard errors (SE) = .02, p = .047, confidence interval (CI) = .01 to 07); (2) individuals who reported a higher level of childhood abuse reported a higher level of trait anxiety (b = .68, SE = .16, p < .001, CI = .40 to 1.00); (3) individuals who reported a higher level of trait anxiety reported a lower level of daily sleep quality (b = –.03, SE = .01, p < .01, CI = –.04 to –.02); (4) individuals who reported a higher level of trait anxiety reported a higher level of physical health issues (b = .01, SE = .004, p = .01, CI = .002 to .02); and (5) individuals who reported a higher level of daily sleep quality reported a lower level of physical health issues (b = –.15, SE = .06, p = .01, CI = –.27 to –.04). Furthermore, a chain of trait anxiety and daily sleep quality partially mediated the association between childhood abuse and physical health issues in later adulthood (a1 × a3 × b2: b = .003, SE = .001, p = .02, CI = .001–006). In other words, individuals who reported a higher level of childhood abuse reported a higher level of anxiety and subsequently a lower level of sleep quality, leading to an increase in physical health issues.
Discussion
Conceptualizing childhood abuse is a prevalent and serious public health issue and an important type of early life stress; this study examined whether childhood abuse affected physical health issues in later adult life, guided by a life-course epidemiological perspective on health. The results indicate that childhood abuse affects physical health issues in later life, aligning with previous studies that experiencing child abuse may undermine health in adulthood (Kendall-Tackett, 2002; Springer et al., 2003). Furthermore, this study expands the previous research in a meaningful way by examining cascading effects of childhood abuse on physical health issues through the potential, sequential mediating roles of trait anxiety and daily sleep quality. In particular, the significant medicating and subsequent mediating roles of trait anxiety (e.g. emotional mechanism) and daily sleep quality (behavioral mechanism) between childhood abuse and physical health issues in later adulthood imply that different pathways (e.g. emotional and behavioral mechanisms) are interplayed and accounted for their cumulative effects on long-term health issues. All in all, the main finding is that childhood abuse not only contributes to mental distress (e.g. trait anxiety), but also has a cascading impact on adults’ physical health both directly and indirectly through trait anxiety and sleep quality.
Due to its prolonged impact, early detection and prevention of childhood abuse have a potential to reverse or at least attenuate its negative consequences. Overall, this study underscores the importance of addressing childhood abuse in particular to promote health outcomes across the life span, potentially by helping survivors of childhood abuse deal with anxiety and also sleep issues. This study suggests that it is critical to raise public awareness that recognizes the seriousness of childhood abuse due to its lasting impact later in life by creating a vicious cycle of repeated health issues. Preventions and intervention programs targeting childhood abuse are recommended.
Potential clinical implications of our findings could be that adult survivors of child abuse may benefit from treatments and interventions that have empirical support such as trauma-focused cognitive-behavioral therapy (e.g. McDonagh et al., 2005) and forgiveness therapy that minimize the effect of childhood abuse and break the vicious cycle of health issues created by adverse childhood experience (e.g. Freedman and Enright, 1996; Lee and Enright, 2014). Furthermore, intervention efforts to improve physical health might specifically tackle reducing anxiety and increasing sleep quality.
This study has some limitations. First, the MIDUS sample is comprised primarily of Caucasian adults, and this limits the generalizability of these findings to the broader population of US adults. Furthermore, this study solely used self-report measures, and the use of retrospective reporting of childhood abuse, which may introduce confounds such as recall bias. Finally, a future study with a larger sample size is required to confirm this study’s preliminary finding.
Despite its limitations, this study contributes to empirical evidence regarding childhood abuse as a life-course risk for physical health issues in later life, as well as an illustration of the roles of trait anxiety and daily sleep quality as potential mediators between childhood abuse and physical health issues in later adulthood. A more conclusive study is needed while addressing the limitations of our study. This study may encourage future research to identify protective factors that weaken the relation between childhood abuse and physical health issues in later life and examine the role of other types of child trauma such as emotional and physical neglect, violence in community (e.g. war), and traumatic experiences caused by a child’s parents or caregivers (e.g. a parent put in prison, separation of parents or divorce, and a parent who misuses substances) on health. This study also may be a foundation to explore different pathways such as social and cognitive mechanisms of these associations as well.