
Abstract
The Sickness Questionnaire (SicknessQ) is a 10-item inventory used to measure sickness-related symptoms. This study extended its psychometric properties in the Chinese context. A total of 992 clinical and non-clinical participants from three samples were included. Exploratory and confirmatory factor analyses indicated a 9-item two-factor structure (mental and physical symptoms) of the Chinese version of Sickness Questionnaire (SicknessQ-C). The internal consistency of the two subscales in this instrument ranged from .71 to .85. The incremental and predictive validities of SicknessQ-C demonstrated that this instrument contributed more to explaining the variance of flourishing than the measurement of negative emotion symptoms.
Sickness behavior refers to the coordinated set of behavioral alterations caused by inflammatory activation in sick individuals (Dantzer, 2001). This behavior includes a wide range of symptoms, including malaise, fatigue, fever, anorexia, insomnia, and pain (Holmes et al., 2011). Previous studies only assessed limited parts of sickness behavior independently, for example, fatigue, anxiety, depressed activities, and physical pain (Chalder et al., 1993; Radloff, 1977; Roberts et al., 1990; Spitzer et al., 2006; Stieglitz et al., 2015; Zwakhalen et al., 2009). Thus, Andreasson et al. (2018) developed a 10-item self-reporting Sickness Questionnaire (SicknessQ) to measure the comprehensive characteristics of sickness behavior. The development of SicknessQ was divided into three phases. First, a pool of 25 items pertaining to sickness behavior was established on the basis of previous evidence-based literature and team members’ clinical experience. Then, a medical experiment was conducted to select items. Endotoxin or placebo was injected into healthy people to provoke sickness response. Then thirteen responsive items were identified. In the third phase, using a sample consisting of primary care patients, a cross-sectional design revealed a one-factor 10-item SicknessQ with adequate reliability (Cronbach’s alpha = .86), concurrent criterion validity (significantly related to anxiety, depression, and self-rated health), and sensitivity to change.
However, SicknessQ has not been translated from Swedish into languages other than English (Andreasson et al., 2020), and its applicability to the Chinese context is unclear. A modified version of the English translation of the Sickness Questionnaire that is used in North American populations has suggested that feeling sick is often context dependent, and preliminary evidence showed that sociocultural factors influence how sickness symptoms are defined, given significance, and acted upon (Shattuck et al., 2020). Different from the Western perspective, traditional Chinese medicine emphasizes “body-mind connection”, which is a holistic viewpoint with the core postulate that the notions of body and mind are mutually dependent yet distinctly different (Chan et al., 2002). The harmony within the body and the mind is the key to human health. Physical illness and discomfort are concurrently accompanied by weakness, fatigue, and sorrow in the mental aspect. Influenced by this viewpoint, most Chinese people are likely to consciously notice and distinguish functional changes in their body and mind when perceiving their sickness conditions and experience. Therefore, the single-factor SicknessQ may manifest into two distinct factors, namely, physical and mental aspects, in the Chinese cultural context.
In addition, incremental validity is a generic form of criterion validity that indicates whether a new measure adds to the prediction of a criterion beyond what can be predicted by other sources of data, as emphasized in assessment practice by previous researchers (Hunsley and Meyer, 2003). Predictive validity is a form of criterion validity that shows how well the variable predicts a known criterion, which has been obtained sometime after the variable has been tested. As mentioned, sickness behavior is manifested by various mental and physical symptoms, such as fatigue, pain, and reduced sociability. Studies have shown that mental and physical symptoms are closely related to individual well-being, which is either “hedonia” (feelings or evaluations about pleasure) or “eudaimonia”, that is, flourishing, which is appropriate to the Chinese people, whose culture emphasizes the values of a virtuous and meaningful life, as well as interpersonal relations (Cheng, 2004; Tang et al., 2016; Tsaousis et al., 2007). For example, Duan and Xie (2019) adopted the Depression Anxiety Stress Scale (DASS) to assess the psychological symptoms of participants. Their results indicated that individuals who had more depression and anxiety symptoms reported less flourishing. Tong and Wang (2017) also demonstrated that psychological symptoms, such as negative emotional experiences, are negatively correlated with flourishing. Moreover, Winter et al. (2013) indicated that somatoform disorders significantly reduce people’s well-being. Compared with instruments that independently measure mental or physical symptoms, such as DASS and Screening for Somatoform Symptoms-7, SicknessQ includes a wide range of mental (e.g. I don’t wish to do anything at all) and physical (e.g. I have a headache) symptoms. Accordingly, the newly developed SicknessQ is expected to contribute to the explanation of well-being more than the other instruments.
The current study aimed to do the following: (a) translate the Sickness Questionnaire into Chinese version (SicknessQ-C) according to the WHO (2009) guidelines on the translation and adaptation of instruments and examine its factor structure; and (b) extend the reliability and concurrent criteria validity from the original study by investigating whether SicknessQ-C accounts for the incremental validity over the established predictor of well-being (flourishing) and further testing its predictive validity on flourishing after 6 months.
Method
Participants and procedures
A total of 992 participants from three sample populations were included. This strategy of obtaining measures of variables from different participant cohorts was performed to eliminate or minimize the common method bias, which is common in social science studies measuring two or more constructs with the same method (Podsakoff et al., 2003). All participants were recruited at convenience. They were asked whether they would like to take part in the study. They signed consent forms before completing the questionnaires. Participants filled out the questionnaire by themselves through the pencil-and-paper method. Ethics approval was granted by the Human Subjects Ethics Sub-Committee of the Department of Sociology, Wuhan University.
Sample 1 comprised 346 community residents (100 males and 246 females, mean age = 45.05 years old, SD = 10.44) recruited from10 communities in Wuhan, China. Sample 2 comprised 423 inpatient university students recruited from the school hospital in Wuhan University (88 males and 335 females, mean age = 19.48 years old, SD = 1.20). They were clinically diagnosed with a wide range of medical problems and hospitalized, such as muscle or joint pain, symptoms from asthma or allergy, accident/injuries, and others. Sample 3 comprised 223 general university students recruited from Wuhan University (42 males and 181 females, mean age = 21.45 years old, SD = 1.15). For all the three samples, the inclusion criteria were as follows: a) age ⩾18 years; and b) willing and able to respond to the questionnaire. Persons with chronic or severe illness, mental disorders, pregnant women, and the disabled were excluded.
The participants in Samples 1 and 2 provided demographic information and completed SicknessQ-C. The participants in Sample 3 were asked to complete a questionnaire package at Times 1 and 2 (6 months later). The package included demographic information, SicknessQ-C, and DASS-21, and Flourishing Scale (FS).
Instruments
SicknessQ
SicknessQ is a brief tool with 10 items used to assess the perceived sickness behavior of people (Andreasson et al., 2018). Participants were asked to rate how they currently feel on a four-level scale ranging from 0 to 3 (0 = disagree, 1 = somewhat agree, 2 = mostly agree, 3 = agree). The translation procedures of SicknessQ recommended by WHO (2009) were considered to achieve equivalence. First, the English-version SicknessQ was translated into Chinese by a PhD student. Then, another PhD student back-translated the Chinese translation into English. Both of them are English as their major and are proficient in English-Chinese translation. The corresponding author supervised the entire translation process and was responsible for verifying the conformity of the translated English items to the original ones, as well as the precision of the Chinese items. Discrepancies were discussed thoroughly and revised by the triangular group.
DASS
Negative emotion symptoms were measured using the 21-item DASS. Lovibond and Lovibond (1995) indicated that the total mean score of DASS measures the individual’s negative feelings in the past week. Respondents completed the DASS on a four-point scale from 0 (did not apply to me at all) to 3 (applied to me very much or most of the time). The DASS displayed good reliability and validity when used in a Chinese population (Wang et al., 2016).
FS
Well-being was evaluated using the FS on a seven-point Likert scale, with 1 = strongly disagree and 7 = strongly agree. Developed by Diener et al. (2010), FS consists of eight items that measure the eudaimonic perspective of psychological well-being, highlighting the flourishing of human functioning. The mean score of the scale indicates the level of flourishing. The scale showed a solid one-factor structure with good reliability and validities in a Chinese population (Duan and Xie, 2019; Tang et al., 2016).
Data analysis
Data were analyzed using SPSS 24.0 and Mplus 7.0. First, exploratory factor analysis (EFA) was conducted to obtain the factor structure of SicknessQ using Sample 1. Principal axis factor analysis and varimax rotation method were adopted. An eigenvalue greater than 1 criterion was used to determine number of factors (Hair et al., 1998). Second, confirmatory factor analysis (CFA) was performed to confirm the factor structure using Sample 2. Some of the more frequently recommended measures of fit and their criteria were adopted, as follows: comparative fit index (CFI) >.90, Tucker-Lewis Index (TLI) >.90, standardized root mean square residual (SRMR) <.08 and root mean square error of approximation (RMSEA) <.08 (McDonald and Ho, 2002; Marsh et al., 2004). Third, Sample 3 was used to check the incremental validity and predictive validity of SicknessQ-C. After descriptive and correlation analyses among the main variables under scrutiny, hierarchical regression models were constructed. Specifically, in the regressions, DASS and SicknessQ-C measured at Time 1 were used as predictors, which were entered step by step. FS measured at Time 1 was set as the dependent variable in the first set of regression to test the incremental validity of SicknessQ-C, whereas FS measured at Time 2 was included as the dependent variable in the second set of regression to further check the predictive validity of the instrument.
Results
Factor structure
EFA
The KMO value (.846) and Bartlett’s test (p < .001) indicated that the current data pool was appropriate for EFA analysis. Ten items in the instrument converged to two factors with eigenvalues of 4.29 and 1.45. According to the meanings of items in each factor, the first factor was named Mental Symptoms (MS, 3 items; e.g. I don’t wish to do anything at all), whereas the other factor was named Physical Symptoms (PS, 7 items; e.g. I have a headache), each reflecting a series of physical responses of sickness. The item loadings ranged from .54 to .85, and the item—total correlations ranged from .65 to .86. In total, the two subscales explained 57.37% of the observed variance. The details are provided in Table 1. However, according to Wymer and Alves (2013), items that cross-load too highly on more than one-factor (e.g. >.32) or cross-loadings less than .15 difference from an item’s highest factor loading should be deleted. In the current case, Item 5 (“I feel depressed”) was identified as a cross-loading item with a loading difference of .14.
Summary of exploratory factor analysis (N1 = 346).

p < 0.05.
CFA
A total of three comparable models were developed: the original single-factor model [χ2 = 240.155, df = 35, χ2/df = 6.862; CFI = .825; TLI = .775; SRMR = .075; RMSEA = .118, 90% CI = .104 –.132], the two-factor correlated model [χ2 = 138.712, df = 34, χ2/df = 4.080; CFI = .911; TLI = .882; SRMR = .057; RMSEA = .085, 90% CI = .070 –.10], and the revised two-factor correlated model after deleting Item 5 [χ2 = 86.844, df = 26, χ2/df = 2.412; CFI = .939; TLI = 0.915; SRMR = 0.051; RMSEA = .074, 90% CI = .057 – .092]. We concluded that the 9-item revised two-factor correlated model (without Item 5) was a better fit compared with the other two models. Standardized path coefficients are shown in Figure 1.
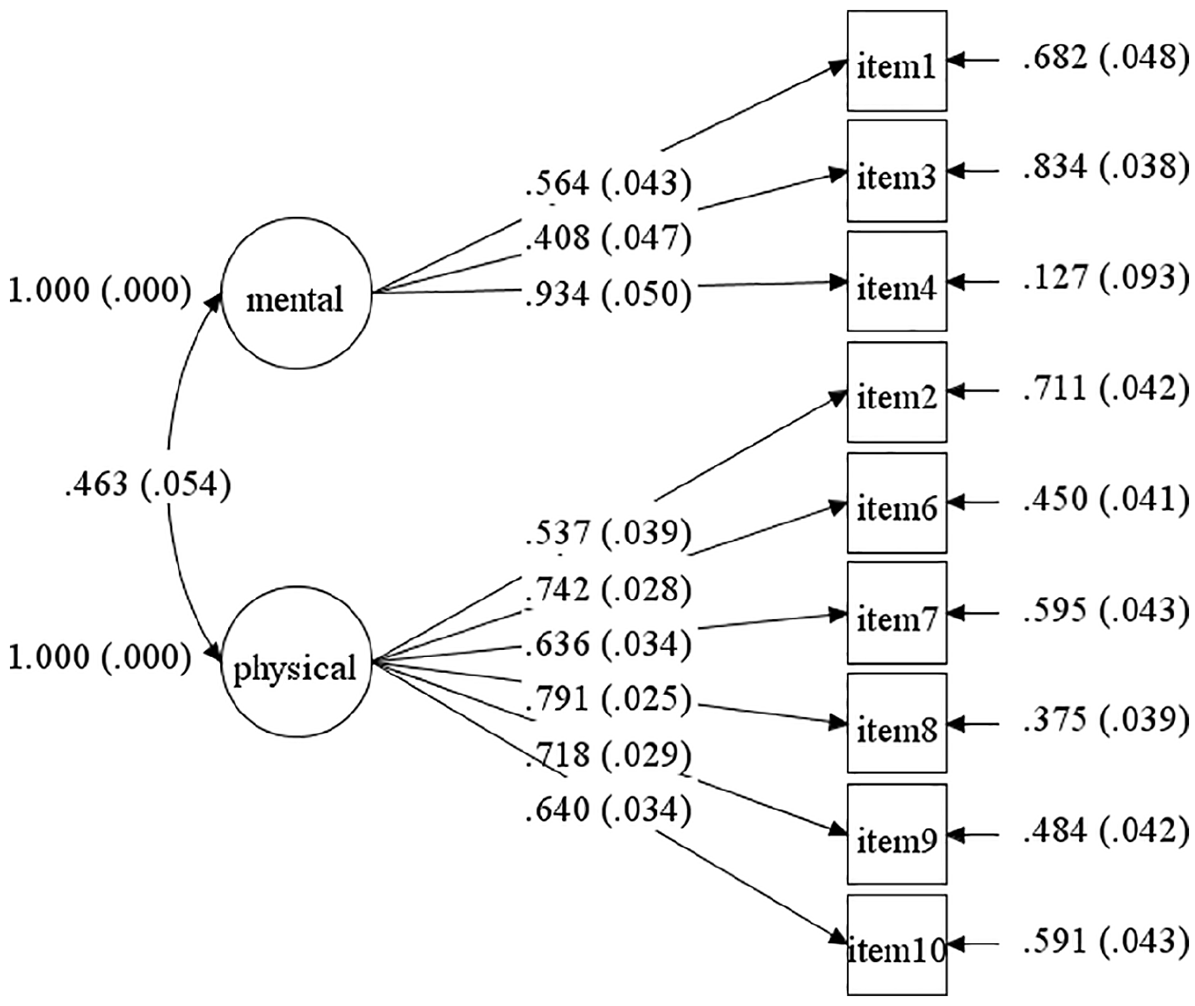
Confirmatory factor analysis model of SicknessQ-C with standardized path coefficients (N2 = 423).
Descriptive statistics and correlation analysis
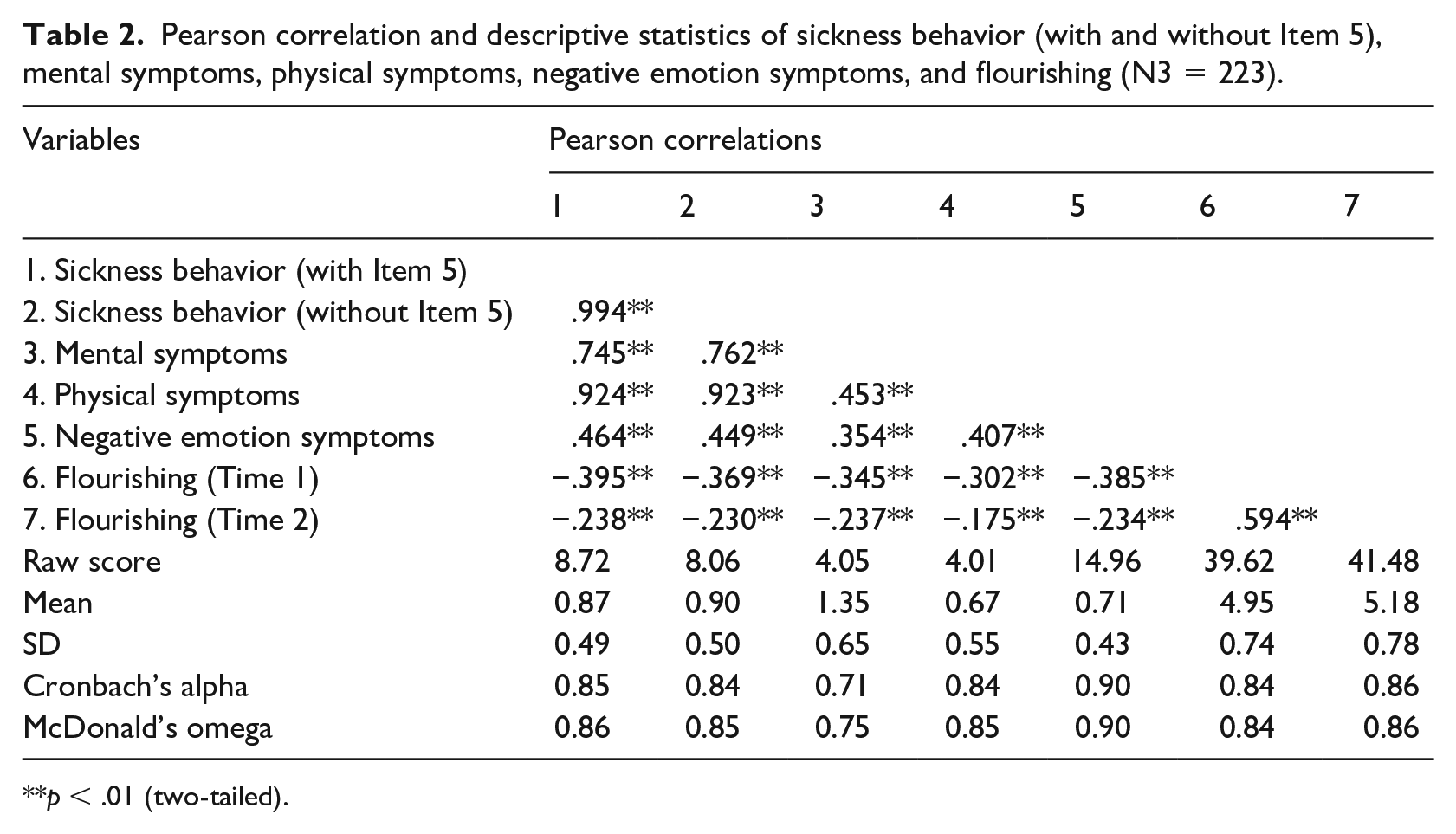
Descriptive statistics and correlations were presented in Table 2. As expected, sickness behavior (with Item 5 “I feel depressed”) was positively related to negative emotion symptoms (γ = .464, p < .01) and negatively related to flourishing (Time 1: γ = −.395, p < .01; Time 2: γ = −.238, p < .01). Moreover, sickness behavior (without Item 5 “I feel depressed”) was positively related to negative emotion symptoms (γ = .449, p < .01) and negatively related to flourishing (Time 1: γ = −.369, p < .01; Time 2: γ = −.230, p < .01). All measures indicted good Cronbach’s alpha values, which were higher than .71, and McDonald’s omega values higher than .75.
Pearson correlation and descriptive statistics of sickness behavior (with and without Item 5), mental symptoms, physical symptoms, negative emotion symptoms, and flourishing (N3 = 223).
p < .01 (two-tailed).
Hierarchical regression analysis
According to the EFA and CFA results, hierarchical regression models were established to further examine the incremental validity and predictive validity of SicknessQ-C (with and without Item 5 “I feel depressed”). Results are summarized in Table 3. For incremental validity, the first set of regression in Model 1 revealed that after controlling negative emotion symptoms (F = 38.362, R2 = .148, Beta = −.385, t = −6.194, p < .001), sickness behavior (with Item 5) (Beta = −.276, t = −4.071, p < .001) at Time 1 contributed 5.2% additional variances of flourishing at Time 1. The first set of regression in Model 2 revealed that after controlling negative emotion symptoms (F = 38.362, R2 = .148, Beta = −.385, t = −6.194, p < .001), sickness behavior (without Item 5) (Beta = −.245, t = −3.627, p < .001) at Time 1 contributed 4.8% additional variances of flourishing at Time 1. These results indicated that compared with the 10-item SicknessQ-C, the 9-item SicknessQ-C also significantly contributed to flourishing with incremental validity. For predictive validity, the second set of regression in Model 1 showed that after controlling negative emotion symptoms at Time 1 (F = 12.766, R2 = .055, Beta = −.234, t = −3.573, p < .001), sickness behavior (with Item 5) (Beta = −.165, t = −2.250, p < .05) at Time 1 contributed 2.1% additional variances of flourishing at Time 2. In the second set of regression in Model 2, after controlling negative emotion, sickness behavior (without Item 5) (Beta = −.157, t = −2.156, p < .05) at Time 1 contributed 2.0% additional variances of flourishing at Time 2. The 9-item and 10-item SicknessQ-C still significantly predicted flourishing even after 6 months.
Hierarchical linear regression of negative emotion symptoms, sickness behavior (with and without Item 5), and mental and physical symptoms on flourishing (N3 = 223).

p < 0.001; **p < 0.01; *p < 0.05.
Furthermore, we conducted Model 3, in which physical and mental symptom subscales of the 9-item two-factor Sickness Q-C were entered in the regression model. As shown in Table 3, the first set of regression in Model 3 revealed that after controlling negative emotion symptoms, the two dimensions of sickness behavior (without Item 5) at Time 1 contributed 5.7% additional variances of flourishing at Time 1. In the second set of regression, after controlling negative emotion, two dimensions of sickness behavior (without Item 5) at Time 1 contributed 2.8% additional variances of flourishing at Time 2. The two-factor solution still significantly predicted flourishing after 6 months. In general, the two-factor solution without Item 5 better explained and predicted flourishing after 6 months compared with the original 10-item unidimensional scale (with Item 5) and the 9-item unidimensional scale (without Item 5).
Discussion
This study extended the psychometric properties of SicknessQ in the Chinese social-cultural context. The 9-item SicknessQ-C was demonstrated to be a two-factor structure scale (i.e. physical and mental symptoms) with adequate reliability. Meanwhile, its incremental validity and predictive validity were examined. Specifically, physical and mental symptoms increased the explained variance in flourishing and predicted additional variances of flourishing beyond the pre-existing assessment of negative emotion symptoms after 6 months.
Interestingly, a two-factor structure rather than the original one-factor model was identified in the Chinese context. The difference might be due to the characteristics of validation cohorts across studies. The present study involved samples comprising general community residents and university students, as well as hospitalized university students, and excluded persons with chronic illness. In contrast, in the development and validation of the original instrument, Andreasson et al. (2018) included healthy participants injected with endotoxin in an experimental study and primary care patients with various disorders. To further evaluate the properties of SicknessQ in an Australian sample, Andreasson et al. (2020) used a combination of patients and university students (18–25 years old) with chronic medically unexplained symptoms. Variations in age, seriousness of diseases, and kinds of symptoms might have led to the inconsistent factor structures of SicknessQ.
Considering the “body-mind connection” viewpoint popular among Chinese people, the differences in factor structures can be explained by the difference in perspective on the concept of sickness between Eastern and Western cultures. Chinese people usually notice their physical and mental manifestations when reporting their sickness conditions and experience. By contrast, such clear distinction in identifying sickness behavior seems uncommon in the Western perspective (Andreasson et al., 2018; Dantzer, 2001). The inconsistent factor structures of the validated instrument in different cultures is not unique. For instance, the Chinese version of Posttraumatic Growth Inventory (Tedeschi and Calhoun, 1996) has four factors versus the five-factor model of the original English version (Ho et al., 2004). Character strengths, which comprised six core virtues proposed by Peterson and Seligman (2004), demonstrated inconsistent factor structures, including five-factor models (Ruch et al., 2010; Singh and Choubisa, 2010) and four-factor models (Brdar et al., 2011) in different cultures, whereas the three-factor structure was found in Chinese culture with qualitative interviews and quantitative data (Duan and Bu, 2017; Duan et al., 2012).
We deleted the cross-loading item “I feel depressed” (Item 5) after factor analysis. Without this item, the model performance in CFA improved, and the ΔR2 in the two-factor solution (without Item 5) was greater in incremental and predictive validity tests compared with the unidimensional solutions (with or without Item 5). Quantitatively, without Item 5, we obtained a robust structure of sickness behavior among Chinese samples. From the theoretical perspective, excluding this item can be explained in the Chinese cultural context. The feeling of being depressed is regarded as one of the minor mental health problems due to heavy stigmatization of people with mental disorders among the Chinese. The feeling of being depressed is not regarded as sickness but a kind of normal and common life problem by traditional medicine professionals and lay people, which is associated with lifestyle and primarily socially explained (Kolstad and Gjesvik, 2012). Therefore, the two-factor solution with 9 items seems reasonable.
The incremental and predictive validities demonstrated that SicknessQ-C contributed more in explaining variance of flourishing than DASS. DASS is designed to assess individual emotional or mental symptoms, whereas SicknessQ-C is a more comprehensive method to measure sickness behavior in humans and captures the physical and mental aspects. Hence, SicknessQ-C had stronger incremental validity in predicting individual well-being than tools assessing only one aspect. This finding is plausible and is supported by other studies. For instance, the Brief Inventory of Thriving (BIT) was created to assess comprehensive well-being (Su et al., 2014), including subjective and psychological well-being, whereas the Satisfaction with Life Scale (SWLS) (Diener et al., 1985) and Flourishing Scale (Diener et al., 2010) were used to measure subjective well-being and psychological well-being, respectively. BIT contributed more variance to negative emotions than SWLS and FS (Duan et al., 2016). Nevertheless, 5.7% and 2.8% (ΔR2 = .057 and ΔR2 = .028) are not a large increase in variance. Cohen (1988) proposed that the average size of the validity increment was about r = .30 (the square root of the R2 change value), and studies from various domains have supported this position; most observed relationships fall in the small to medium range (i.e. r = .10 to .30 or ΔR2 = .01–.09) (Haranin et al., 2007; Meyer, 2000; Rode et al., 2008). The effects were modest in magnitude but were statistically significant, and the validities under scrutiny were acceptable.
In summary, this study indicated that the 9-item two-factor SicknessQ-C was a reliable and valid measure of sickness behavior among Chinese samples and reflected physical and mental aspects of sickness responses in individuals. In practice, SicknessQ-C can be used as an effective tool to assess mental and physical symptoms caused by inflammatory activity among Chinese. It provides important information and insights into individual sickness situations and promotes further actions and timely treatments.
Several limitations should be addressed. First, our samples were obtained through convenience sampling method. Thus, the generalizability of the results may be limited. A sample that includes both clinical and non-clinical participants is needed in future research to further elucidate the interpretation and reporting of sickness behavior and to lend more evidence to the factor structure and the predictive and incremental validity of the instrument. Second, the study favored a theoretically meaningful two-factor model rather than the unidimensional scale developed by Andreasson et al. (2018). As we mentioned, this might be partly explained by the difference in perspective on the concept of sickness between Eastern and Western cultures. However, empirical evidence on this kind of cultural difference is lacking. Hence, qualitative material, such as cognitive interviews with individuals and healthcare practitioners about their understanding and interpretation of sickness manifestations, might help. In addition, more samples from similar cultural contexts, such as Hong Kong, Taiwan, and other Asian societies, might offer more evidence to support the two-factor structure. The current study examined the limited aspects of validities, primarily the predictive and incremental validity, in terms of relationships with negative emotion symptoms and flourishing. Other psychometric properties, such as the measurement invariance for SicknessQ-C across groups of diverse characteristics and the convergent and discriminant validities, should be investigated in the future.
Footnotes
Acknowledgements
The authors thank the participants for their generous contributions to this research.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by “The Fundamental Research Funds for the Central Universities (Youth Innovation Program), Zhongnan University of Economics and Law”.
Data availability statement
Please contact the corresponding author for the data of this article.