
Abstract
The goal of this study was to examine weight stigma experiences during medical visits as related to provider-patient relationship factors and adherence among individuals with hypothyroidism. A total of 362 participants recruited via social media participated in an online survey. Regression and mediation analyses indicated that weight stigma was negatively associated with adherence; this relationship was mediated by decreased trust in provider, less perceived provider empathy, and lower provider-patient depth-of-relationship. Structural equation modeling with BMI controlled revealed that weight stigma is associated with worsened provider-patient relationship and adherence. Findings suggest the importance of eliminating weight stigma experiences for patients.
Keywords
Weight is a highly stigmatized personal characteristic (Puhl and Brownell, 2001). Weight stigma involves the negative attitudes or perceptions surrounding individuals who are overweight or obese. Negative stereotypes that exist in our society about those who are overweight or obese include that they are lazy, weak-willed, and lack self-control (Puhl and Brownell, 2001). These negative perceptions can lead to bias and discrimination against individuals who are overweight or obese. In fact, rates of weight discrimination are similar to rates of racial discrimination (Puhl et al., 2008).
Research to understand how weight stigma is related to psychological well-being and health is necessary because about 70% of Americans over the age of 20 are overweight or obese (FastStats CDC, 2019). Weight stigma experiences have been associated with depression and lower quality of life (Jackson et al., 2015). Limited research has examined weight stigma experiences for individuals with hypothyroidism who might be susceptible to experiences of weight stigma due to the common symptom of weight gain.
Unfortunately, weight stigma is common in health care settings. Health care professionals are not immune to the negative societal perceptions surrounding those who are overweight or obese; health care providers often hold negative attitudes about these individuals (Puhl and Heuer, 2009); these may influence how they communicate with these patients. Indeed, one study found that participants rated doctors as one of their greatest sources of weight stigma (Puhl and Brownell, 2006). In a health care setting, examples of weight stigma may include a provider blaming a patient’s conditions on their weight status or assuming that the patient is weak-willed due to their weight status.
The purpose of this study was to examine how weight stigma during medical visits is related to aspects of the provider-patient relationship and adherence in patients with hypothyroidism.
Weight stigma and the provider-patient relationship
The negative perceptions that providers may have about their patients who are overweight or obese could be related to provider-patient communication during a medical visit. Previous research indicates that provider-patient communication and relationship factors are linked to medical visit outcomes such as patient satisfaction and adherence (Beck et al., 2002).
Previous research has shown that a patient’s weight may affect the provider-patient relationship. For instance, Gudzune and colleagues examined audio-recorded medical visits and coded communication using the widely used Roter Interaction Analysis System (RIAS) (Gudzune et al., 2013). Results showed that physicians built less emotional rapport with patients who were overweight or obese. Emotional rapport included aspects such as partnership, self-disclosure, concern, legitimation, and reassurance. Ultimately, lack of rapport with patients who are overweight or obese could be associated with decreased satisfaction, worse health outcomes, and lower adherence.
Empathy is another central component of provider-patient communication that involves “putting oneself in someone else’s shoes” and can be related to medical visit outcomes. One study found that women’s weight stigma experiences in health care were associated with lower perceptions of provider empathy (Ferrante et al., 2016). When patients do not perceive their physician as empathetic, a less trusting provider-patient relationship and negative health outcomes, such as nonadherence to treatment, are possible.
Trust is another important component of the provider-patient relationship, and experiences of weight stigma during medical visits may be associated with provider trust. In one study, participants were asked to report on provider trust and if they had ever felt that their physician judged them because of their weight. Results showed that feeling judged about weight was associated with decreased trust in the provider (Gudzune et al., 2014). Studies have shown that patients who trust their providers are more likely to adhere to recommendations such as preventative screenings (O’Malley et al., 2004) and antiretroviral therapy for HIV patients (Blackstock et al., 2012). When patients who are overweight or obese do not trust their providers, they may be at an increased risk for nonadherence.
Providers may also communicate differently with their patients who are overweight or obese (Washington Cole et al., 2017). In this study, recorded prenatal visits were coded using the RIAS and then evaluated for aspects of provider-patient communication. Results showed that providers discussed lifestyle factors, such as physical activity, nutrition, and breastfeeding, less with patients who were overweight or obese. In addition, providers used fewer concern and approval statements (i.e. indicators of rapport building) during their visits with patients who were overweight.
Weight stigma and adherence
As discussed in the previous section, patients’ weight status and weight stigma during medical visits can negatively affect the provider-patient relationship and communication, which can, in turn, affect how patients perceive their medical care and outcomes after their visit.
Adherence has been defined as “the extent to which a person’s behavior corresponds with agreed recommendations from a health care provider” (Sabaté and World Health Organization, 2003). It is estimated that only about 50% of patients are adherent to their treatment across conditions (Sabaté and World Health Organization, 2003), and nonadherence is a significant problem that can lead to poor health outcomes. In hypothyroidism specifically, one study found that nonadherence to medication was associated with more healthcare spending, increased use of acute care, and comorbidity with other disorders (Hepp et al., 2018). When provider-patient communication does not include rapport, empathy, respect, and trust, adherence can be affected. Individuals who are overweight and obese may be at risk for lower adherence due to the nature of their relationships with physicians.
Obesity can reduce patient adherence to various health recommendations. For example, studies have shown that obesity is a barrier to individuals receiving the proper health care screenings. Women with obesity are less likely to be screened for cervical cancer and breast cancer (Maruthur et al., 2009a, 2009b). In addition, in a study with bariatric surgery patients, weight stigma predicted worse adherence to dietary recommendations after the surgery (Raves et al., 2016).
Additionally, weight-based discrimination was strongly associated with nonadherence in a sample of African-American women with hypertension (Richardson et al., 2014). Participants were asked to report experiences of discrimination due to weight in situations such as at work, during medical care, and in a public setting. Individuals who reported experiencing discrimination due to weight had greater odds of nonadherence. Self-efficacy mediated this relationship; thus, patients who experienced discrimination may not have felt confident that they could adhere.
In addition to lower adherence, weight stigma may be a barrier to the effective treatment of diabetes. In a study of patients with Type II diabetes, individuals who attributed discrimination to their weight reported fewer self-care behaviors related to exercise, glucose testing, and diet (Potter et al., 2015). Although this study looked at discrimination attributed to weight in all areas of life, not specific to medical visits, the results are still important. One could hypothesize that feeling health care-related discrimination could be more detrimental to effective diabetes management than feeling discrimination from other sources.
Hypothyroidism
Hypothyroidism is characterized by an underactive thyroid that does not produce enough hormones. This condition is more common in women and can result from a number of events such as thyroid surgery, medications, or an autoimmune disease (Mayo Clinic, 2020). Previous research has shown that levels of thyroid stimulating hormone (TSH) are associated with weight gain (Fox et al., 2008). Treatment for hypothyroidism generally involves taking synthetic thyroid hormone medication daily. However, even with a relatively simple treatment regimen, adherence levels to hypothyroid medications are similar to levels for other chronic illnesses with more complex treatment regimens, such as Type 2 diabetes (Briesacher et al., 2008). For example, a recent study showed that about 54% of patients were nonadherent to their thyroid replacement medication (Hepp et al., 2018).
Theoretical background of the present study
A useful theoretical model to understand this work is the Homeostatic Theory of Obesity (Marks, 2015), later extended to the General Theory of Behaviour (Marks, 2018). Within this obesity theory, the “circle of discontent” suggests a pathway through which body dissatisfaction can lead to negative emotions, which can reinforce behavior promoting obesity. A component of the Homeostatic Theory of Obesity involving obesity prevention is ending weight stigma, which is the focus of the current study.
Present study
The current study explored weight stigma experiences for individuals with hypothyroidism because of the associations between hypothyroidism and weight gain. The purpose of this study was to examine weight stigma experiences during medical visits for individuals with hypothyroidism and to determine if these experiences were related to provider-patient relationship factors and adherence.
The current study had three hypotheses. The first hypothesis was that weight stigma would be negatively associated with adherence (H1). The second hypothesis was that this relationship would be mediated by (H2a) a patient’s level of trust in their health care provider, (H2b) perceived provider empathy, and (H2c) the depth-of-relationship between the health care provider and the patient. The third hypothesis was that the relationship between weight stigma and adherence would be independent of a patient’s weight (H3).
Method
Participants
This study included 362 participants, who were recruited through posting the survey link and description to one Facebook support group, to one Facebook page, and one Reddit page, each designated for hypothyroidism support. Data were collected via Qualtrics in June and July of 2018. The inclusion criteria for the study included that individuals must be 18 years or older and have a diagnosis of hypothyroidism. Each participant provided informed consent on the first page of the online Qualtrics survey. Participants were compensated for their time by being entered into a raffle for a chance to win one of forty $50 Amazon gift cards. The Institutional Review Board at Texas State University approved this study.
Measures
Demographics and BMI
Items asking about demographic information such as age, gender, education level, height, and weight were included in the survey. BMI was used as the measure of weight in this study and was calculated by dividing self-reported weight (in pounds) by height (in inches) squared and then multiplying by 703 (About Adult BMI, CDC, 2019).
Weight stigma
Weight stigma during medical visits was measured using the 20-item Stigma Situations in Health Care Scale (Ferrante et al., 2016), which was modified from Myers and Rosen’s Stigmatizing Situations Inventory (1999). Items were modified by changing “doctor” to “health care provider’” and from asking participants to only report incidences of stigma within the last 12 months at a certain clinic to asking participants to consider any stigmatizing experiences during medical visits at any point. Response options ranged from 0 (never) to 3 (three or more times), and the highest possible score was 60.
Trust
Trust in provider was measured using one item modified from Gudzune and colleagues (2014), who used this single 10-point rating measure of physician trust in their study of weight stigma. The item was validated in previous research as part of the Consumer Assessment of Healthcare Providers and Systems (CAHPS® Cultural Competence Item Set (Weech-Maldonado et al., 2012). Participants were asked to answer based on their primary health care provider.
Empathy
The 5-item Jefferson Scale of Patient Perceptions of Physician Empathy (Kane et al., 2007) was used to measure patient perceptions of provider empathy. Participants were asked to consider their primary health care provider.
Depth of physician-patient relationship
Depth of the physician-patient relationship was measured using the 8-item Patient-Doctor Depth-of-Relationship Scale (Ridd et al., 2011). Participants were instructed to answer these questions about the provider who primarily treated their thyroid condition.
Adherence
Adherence to medication was measured using the General Adherence Scale from the Medical Outcomes Study (DiMatteo et al., 1993). This 5-item scale assessed adherence behavior in the past 4 weeks.
Procedure
This study utilized Qualtrics to administer online surveys to participants. The survey time to completion was 45–60 minutes, and participants were told that they could skip any question that they did not feel comfortable answering. Participants did not enter any identifying information; they were directed to a separate survey at the end to enter their email address to enter the raffle.
Statistical analyses
To test the first hypothesis, correlation analysis was performed among all study variables. To test the second hypothesis, mediation analyses were conducted using the bootstrap method with the SPSS Macro for Multiple Mediation provided by Preacher and Hayes (Preacher and Hayes, 2008). The tests used 1000 bootstrap samples and were used to test direct and indirect effects of weight stigma on adherence through each of the mediators. Separate mediation analyses were run for each of the hypotheses, H2a, H2b, and H2c. BMI was included as a covariate in all models. In addition, a cohesive model including all of the mediators was examined by structural equation modeling using the lavaan package (Rosseel, 2012) in R.
Results
Sample characteristics
A total of 644 individuals completed the Qualtrics survey. In addition, 134 individuals who did not report a diagnosis of hypothyroidism were excluded. From this sample, eight individuals were excluded because they reported being currently pregnant. An additional 140 participants did not finish all relevant measures. The remaining sample of 362 individuals concluded the survey and were included in the analyses for this study.
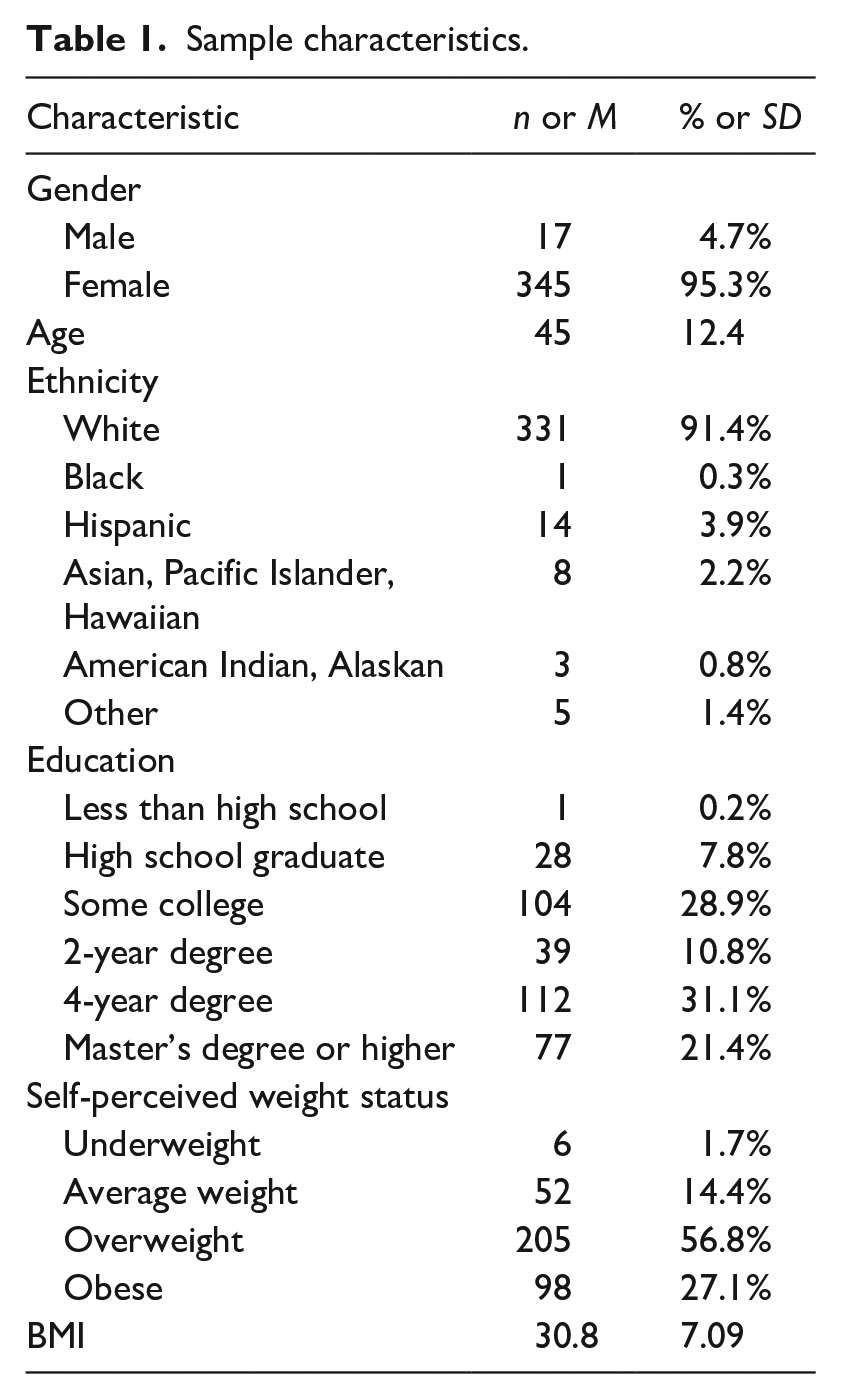
The sample was primarily female (95%) which was expected due to hypothyroidism being more common in females. Participants were primarily White (91.4%). The mean age was 45 years (SD = 12). The average level of weight stigma experienced by individuals in our study was 7.30 (SD = 9.71, range = 0–47). Results indicated that our sample did experience weight stigma. It is interesting to note that about 63% of participants reported experiencing one instance of weight stigma at least once, but we did not see a high rate of frequent or repeated instances of weight stigma. This sample had relatively high levels of adherence (M = 4.00, SD = .95). Sample characteristics are summarized in Table 1; additional descriptive statistics and reliability analyses for the scales used in this study are provided in the Supplementary Files.
Sample characteristics.
Correlations
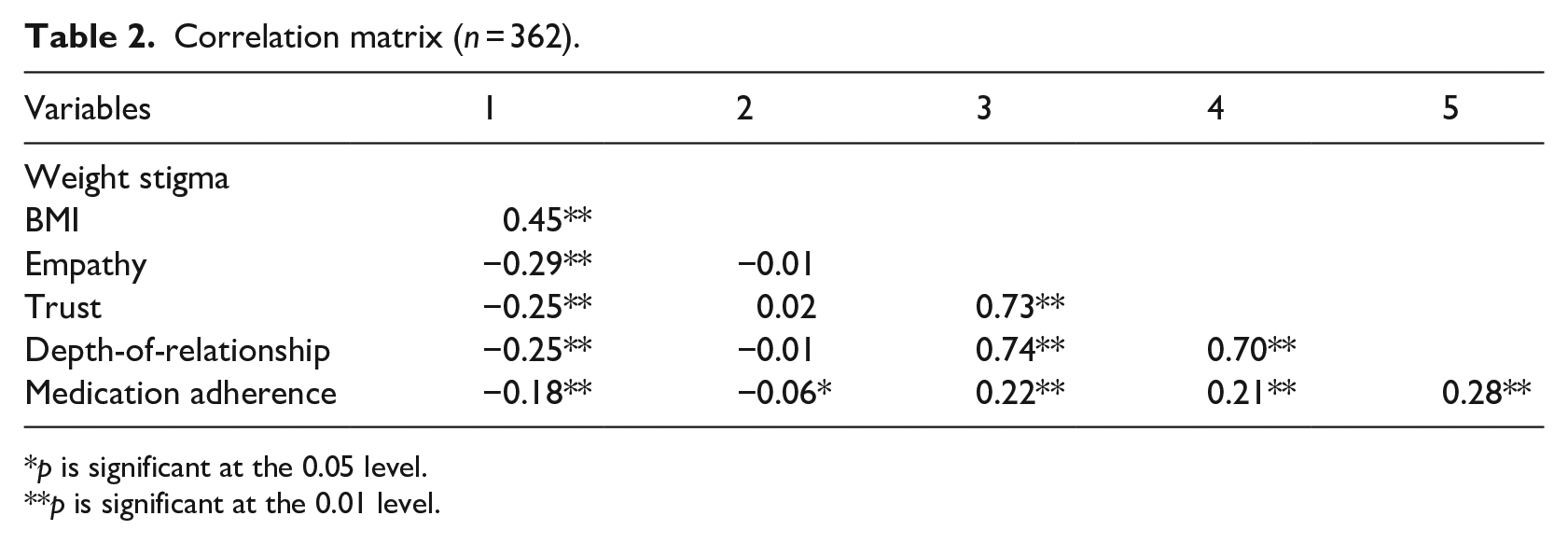
Table 2 shows the Pearson correlation coefficients between variables in this study. Weight stigma experiences during medical visits were significantly negatively correlated with adherence (r = –.18, p < .01), supporting H1. Weight stigma was also correlated with the provider-patient relationship factors (all p < .01). BMI was also negatively correlated with adherence (p < .05). Therefore, it was controlled in the following analyses to examine the unique effect of weight stigma on adherence.
Correlation matrix (n = 362).
p is significant at the 0.05 level.
p is significant at the 0.01 level.
Mediation analyses
Three mediation analyses were performed to test the second hypothesis. The figures depicting each model are included as Supplementary Files. BMI was entered into the models as a covariate. The first model used trust as the mediator. Weight stigma significantly related to adherence (c path), ß = –.20, SE = .06, t(351) = –3.52, p = .0005. Weight stigma also significantly related to trust (a path), ß = –.32, SE = .06, t(351) = –5.68, p < .001. Trust significantly related to adherence (b path), ß = .17, SE = .05, t(351) = 3.17, p = .0017. With the addition of the mediator, trust, the direct effect of stigma on adherence was reduced, suggesting a mediating effect (c’ path), ß = –.15, SE = .06, t(351) = –2.49, p = .0132. The indirect effect of weight stigma experiences on adherence through trust was significant, ß = –.05, 95% CI [–.1001, –.0195].
The second model used empathy as the mediator. Weight stigma significantly related to adherence (c path), ß = –.19, SE = .06, t(356) = –3.37, p = .0008. Weight stigma also significantly related to empathy (a path), ß = –.35, SE = .06, t(356) = –6.24, p < .001. Empathy significantly related to adherence (b path), ß = .17, SE = .05, t(356) = 3.28, p = .0012. With the addition of the mediator to the model, the direct effect of stigma on adherence was reduced, suggesting a mediating effect (c’ path), ß = –.13, SE = .06, t(356) = –2.21, p = .0277. The indirect effect of weight stigma experiences on adherence through empathy was significant, ß = –.06, 95% CI [–.1133, –.0194].
The third model used depth-of-relationship as the mediator. Weight stigma significantly related to adherence (c path), ß = –.19, SE = .06, t(352) = –3.39, p = .0008. Weight stigma also significantly related to depth-of-relationship (a path), ß = –.30, SE = .06, t(352) = –5.43, p < .001. Depth-of-relationship significantly related to adherence (b path), ß = .25, SE = .05, t(352) = 4.75, p < .001. With the addition of the mediator, depth-of-relationship, the direct effect of stigma on adherence was reduced (c’ path), ß = –.12, SE = .06, t(352) = –2.03, p = .0431. The indirect effect of weight stigma experiences on adherence through depth-of-relationship was significant, ß = –.08, 95% CI [–.1230, –.0385].
SEM models
Since trust, empathy, and depth-of-relationship all measure aspects of the provider-patient relationship and they were highly correlated with each other (see Table 2), we combined them as a latent factor, “provider-patient relationship” in a structural equation model (SEM). The SEM model also included BMI as a covariate.
Figure 1 shows the proposed SEM model with the standardized path coefficients. This model fit the data well (Hu and Bentler, 1999), X2(6) = 5.22, p = .516, CFI = 1.00 > 0.9, RMSEA = 0.00 < 0.08, 90% CI RMSEA = [0.00, 0.06]. Since this model included a path from BMI to adherence which was not significant (ß = .01, p = .91), we deleted this path. The final model fit the data equally well with more degrees of freedom, X2(7) = 5.23, p = .623, CFI = 1.00, RMSEA = 0.00, 90% RMSEA CI [0.00, 0.05]. According to the final model, with BMI controlled, weight stigma has an overall negative effect on adherence, including a direct effect (ß = –.12) and an indirect effect via provider-patient relationship as the mediator (ß = –.08). The cohesive mediation model was supported by SEM.
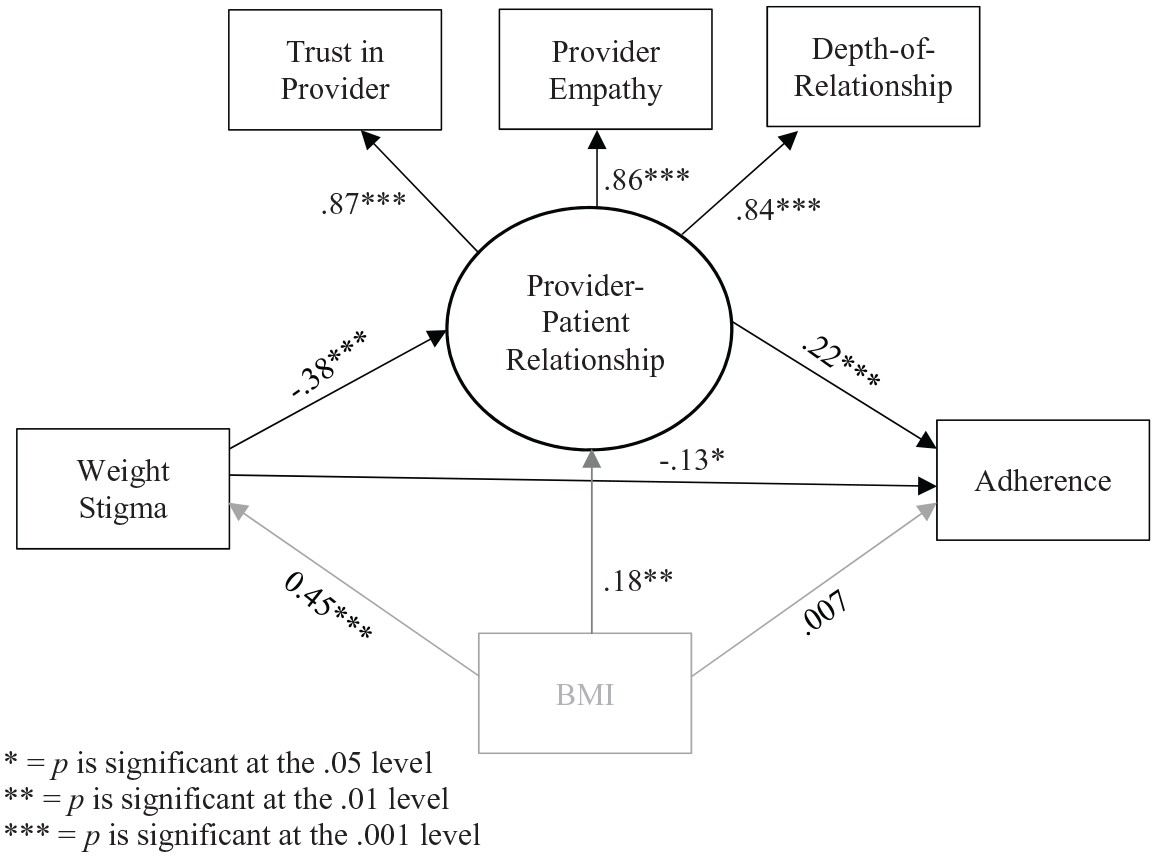
Structural equation model with standardized path coefficients.
Discussion
Our results support the three hypotheses and show that weight stigma during medical visits is related to various aspects of the provider-patient relationship and adherence. Previous research has also demonstrated that weight stigma during medical visits is related to aspects of the provider-patient relationship such as trust and empathy (Ferrante et al., 2016; Gudzune et al., 2014); thus, our results are in line with past research. Our study builds upon previous research by demonstrating that these weight stigma experiences may potentially reach further than the provider-patient relationship, and the cross-sectional data suggests that it might also be related to patient adherence.
The first hypothesis in this study was that weight stigma during medical visits would be negatively associated with adherence. Results support this hypothesis and show that the more weight stigma someone reported experiencing, the lower their level of adherence. This finding shows that weight stigma experiences during medical visits might extend beyond the provider-patient relationship and could be related to the patient’s subsequent adherence to treatment. This supports past research demonstrating a relationship between weight stigma and nonadherence to cancer screening, self-care behaviors, and dietary recommendations (Maruthur et al., 2009b; Potter et al., 2015; Raves et al., 2016).
The second hypothesis was that the relationship between weight stigma and adherence would be mediated by (a) trust in provider, (b) perceived provider empathy, and (c) depth-of-relationship. Results fully supported this hypothesis.
First, previous research has shown that weight stigma experiences during medical visits are associated with trust in the provider (Gudzune et al., 2014), as well as trust in the provider being associated with adherence (Blackstock et al., 2012). Thus, it was expected that trust would be a mediator between weight stigma experiences and adherence, supporting previous research. When patients feel less trust in their provider, they may question whether their treatment recommendations are necessary or will be beneficial, potentially leading to nonadherence.
Additionally, the relationship between weight stigma and adherence was mediated by perceived provider empathy, as well as by depth of relationship between provider and patient. Past research has shown that weight stigma experiences are associated with perceptions of empathy from the provider (Ferrante et al., 2016). Empathy may be associated with adherence. Results build upon past findings by demonstrating that the lack of provider empathy toward patients with overweight or obesity could be related to nonadherence. When a provider demonstrates empathy, a patient perceives the provider has their interests at heart, making them more confident in the benefits of treatment. Regarding the findings on the depth of the relationship between the provider and patient, past work in this area has not looked specifically at associations between weight stigma experiences and depth-of-relationship. However, the findings suggest that a deeper relationship between providers and patients might potentially promote adherence because the patient may feel more comfortable discussing concerns about their medication.
The SEM model provided solid support for the relationship between weight stigma and adherence, especially that this relationship was distinct from BMI. The model showed that the direct effect of weight stigma on the provider-patient relationship was negative when BMI was controlled, meaning that if individuals have the same BMI, weight stigma experiences are negatively related to the provider-patient relationship. Thus, it may not be a patient’s weight that is associated with the provider-patient relationship but that weight stigma during the medical visit may be especially harmful when it comes to the provider-patient relationship.
An unexpected finding in this study was that the direct effect of BMI on the provider-patient relationship was positive when weight stigma was controlled; therefore, if individuals experience the same levels of weight stigma, BMI is positively related to the provider-patient relationship. This finding may be surprising because providers may have negative attitudes regarding their patients who are overweight or obese, but this may show that unless weight stigmatization occurs, the relationship may not be impaired. It is possible that since no measure of provider-patient communication or health care provider perceptions of the patient were included in the model, BMI could be negatively associated with those aspects of medical visits rather than the provider-patient relationship factors.
Moreover, BMI has no direct effect on adherence. This further demonstrates that it may not be BMI alone that is related to the provider-patient relationship and adherence but that weight stigma may be more strongly associated with these aspects of medical care.
Limitations
This study has several limitations to consider when interpreting the results. First, this study utilized cross-sectional data while conducting mediation analyses and structural equation modeling. Thus, we cannot assume causation as the models show associations.
Additionally, this study used self-report data. Participants had to remember possible weight stigma experiences during past medical visits, and recall can be affected during sometimes stressful medical care experiences. Also, the measurement of weight stigma experiences during medical visits may not have been all-encompassing. For example, a participant may have had an experience with weight stigma that was not asked about on the questionnaire. Next, the sample is nearly all female (96%); this limits the generalizability of the findings. Furthermore, trust in provider was measured using one item; a multi-item scale could enhance measurement. Recruiting via social media support groups could also be viewed as a limitation for the study. It could be assumed that someone who is having trouble with treatment for their hypothyroidism or is having difficulty finding a supportive health care provider would be more likely to seek support through social media, potentially creating bias in our sample.
Future research
Future research should examine other possible mediators that may explain the relationship between weight stigma and adherence. Although the provider-patient relationship does seem to play a role in the association between weight stigma and adherence, there was still a direct effect of weight stigma on adherence, meaning that there are other possible explanations for this relationship.
Conclusion
Results indicate that weight stigma experiences during medical visits are negatively associated with adherence. Experiencing weight stigma during a medical visit was related to certain aspects of the provider-patient relationship, and both of these factors were then negatively related to adherence. These findings demonstrate the importance of health care providers increasing awareness of weight stigma and striving to eliminate these experiences for their patients.
Providers could help to reduce weight stigma in healthcare by using language that patients feel comfortable with when discussing body weight. For example, studies have shown that patients prefer the words “high BMI” rather than “fat” (Puhl et al., 2013). Using person-first language (e.g. “person who is overweight”) is also important when discussing weight with patients. Providers could also educate themselves further on the causes of obesity to see that the cause may be more than the patient lacking self-control. Finally, providers should avoid placing blame on patients for causing their overweight or obesity.
Supplemental Material
Supplementary_files_for_JHP_Second_Revision – Supplemental material for Weight stigma is associated with provider-patient relationship factors and adherence for individuals with hypothyroidism
Supplemental material, Supplementary_files_for_JHP_Second_Revision for Weight stigma is associated with provider-patient relationship factors and adherence for individuals with hypothyroidism by Morgan Snyder, Kelly Haskard-Zolnierek, Krista Howard and Yueqin Hu in Journal of Health Psychology
Footnotes
Data sharing statement
This manuscript includes sharing of individual de-identified participant raw data and output from all analyses presented in the manuscript. The data will be available when the article is published and will be available as long as the journal deems it appropriate. It will be shared for use by other researchers, and the dataset will be available in Figshare and as ![]() on the SAGE Journals platform
on the SAGE Journals platform
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.