
Abstract
This study examined the contributions of parents’ characteristics, normative stressors, coping strategies, and social support to psychological distress and neuroticism among 1000 Syrian refugees. The conditions of being older, mothers, partnered parents, and resettlement in Lebanon increased the risk of mental health problems. Mental health problems decreased with fathers’ employment, large families, and time spent in the host country. Types of daily stressors had differential effects on psychological distress and neuroticism. While emotion-focused coping increased psychological distress and neuroticism, the use of problem-focused coping, and informational support reduced neuroticism. The clinical and policy implications of these conclusions were discussed.
Keywords
Introduction
Since 2011, the armed conflict in Syria has forced many Syrians to migrate. According to UN data, approximately 5.6 million Syrians have resettled in neighboring and developed countries, of whom 15.8% resided in Lebanon and 11.8% in Jordan (UNHCR, 2020).
Refugees who have been forced to flee the war in Syria are reported to be at high risk for mental health problems (Alpak et al., 2015), psychiatric illness, dysfunctional behavior and psychological distress (Georgiadou et al, 2017; Khamis, 2019a, 2019b; Naja et al., 2016) due to exposure to war trauma or economic hardship, experience of physical harm and separation, and poor socioeconomic conditions, such as social isolation and unemployment in the destination country (Alpak et al., 2015; Porter and Haslam, 2005; UNHCR, 2014).
The effects of forced displacement and resettlement on the family unit and in particular parents can be far-reaching, restrictive, and disruptive, and they may be economic, social, and emotional in nature. Scientific knowledge relevant to understanding refugees’ mental health has substantially increased during the past decade. Most studies indicate increased risk of psychological distress, psychopathology and more symptoms of neuroticism amongst refugee populations (Fazel et al., 2005; Khamis, 2019b). Neuroticism has been directly linked to psychopathology. A growing body of literature has documented that there is a close relation between neuroticism and PTSD and depression symptoms (Paulus et al., 2016; Xia and Ding, 2011). Prevalence rates in Syrian refugees range from 21% to 46% for PTSD (Cheung Chung et al., 2018; Kazour et al., 2017) from 20% to 44% for depression and from 19% to 32% for anxiety (Georgiadou et al., 2017; Naja et al., 2016). Given the high prevalence rates of mental health problems within these populations, there is a great need for research examining post-resettlement factors that may contribute to, or protect against, the development and maintenance of these mental health problems among refugee parents in various host countries.
There has been a great deal of research on the impact of war atrocities on refugees’ mental health before or during flight, however, only recently have researchers come to recognize how profoundly post-resettlement circumstances impact refugees’ well-being (Li et al., 2016; Miller and Rasmussen, 2010; Tinghög et al., 2017).
While pre-flight trauma is recognized as a key predictor of psychological distress in refugees, life events and changes, both normative and situational, which are experienced by the family in the resettlement context may actually account for greater variance in refugees’ mental health status (Carswell et al., 2011; Fernando et al., 2010; Laban et al., 2005; Miller et al., 2008; Rasmussen et al., 2010). The experience of resettlement confronts refugees with a host of stressful challenges, including the asylum process and immigration policy (Li et al., 2016; McCarthy and Marks, 2010), learning a new language and culture, adapting to the loss of family, friends, and home with inadequate social support or material possessions in an environment where there is widespread discrimination, unemployment, and financial difficulties (Akesson and Sousa, 2019; Fazel and Stein, 2002; Lustig et al., 2004). In addition, research clearly indicates that refugees’ mental health is highly influenced by the conditions that they live in post-migration. Those residing in refugee camps in low-income countries show the highest prevalence of anxiety and depression, reflecting the highly stressful conditions typically encountered in the camps (Li et al., 2016). Greater levels of family disruption and transitions can create environments that lack stability and structure, which in turn are likely to be a source of stress for parents and can adversely affect their mental health (Miller et al., 2018). However, little is known about the mechanisms by which these stressors have an impact on mental health, particularly among refugee parents (Li et al., 2016; Tinghög et al., 2017). Understanding these mechanisms has the potential to illustrate the specific contribution of a particular stressor to one or more adverse outcomes as well as the types of stressors contributing to a single adverse outcome. An understanding of parental functioning that considers post-resettlement stressors is particularly salient to child and family well-being as well as the capacity of parents to deliver competent, quality parenting to children (Akesson and Sousa, 2019; Gavidia-Payne et al., 2015).
Research suggests that personal, familial, and social attributes affect individuals’ psychological adaptation to the experience of resettlement in a host country.
Studies on the effects of socio-demographic variables in the etiology of mental health problems among refugees have produced mixed findings. Some studies have indicated that female gender (Gerritsen et al., 2006), younger age (Cantekin et al., 2017), and high socio-economic status (Carswell et al., 2011; Lindencrona et al., 2008) are associated with heightened risk for psychological distress among refugees, whereas in other studies the opposite pattern has been reported (Bhui et al., 2003; Gerritsen et al., 2006; Laban et al., 2008; Rasmussen et al., 2010). Specific social factors that may be especially important for refugees’ mental health include marital status. Research has further suggested that the refugees without a partner (separated, widowed, divorced) had more psychosocial problems than those who were with spouses (Cantekin et al., 2017; Georgiadoua et al., 2020).
A central question for the study of psychological distress and neuroticism among Syrian refugee parents in post- resettlement contexts is whether specific styles of coping impact specific outcomes. Coping strategies are the constantly changing cognitive and behavioral efforts to manage external and/or internal demands that are appraised as taxing or exceeding the resources of the person (Lazarus and Folkman, 1984). This construct has received considerable attention in the psychological literature (e.g. Billings and Moos, 1981; Pearlin and Schooler, 1978), most frequently as a factor that mediates the relation between stress and physical or mental disorders. Coping responses are classified in many ways. Pearlin and Schooler (1978) differentiate between efforts to change the situation and attempts to control distress, as well as responses that alter the cognitive appraisal of stress. Billings and Moos (1981) suggest a related typology consisting of active-behavioral strategies, active-cognitive strategies, and avoidance strategies. Lazarus and Folkman (1984) describe two forms of coping: problem-focused strategies that are directed toward the management of a problem and emotion-focused strategies that are directed toward amelioration of the associated level of emotional distress. In several different studies, problem-focused strategies have been reported to have positive association with well-being. A reliance on emotion-focused strategies, on the other hand, tends to be associated with poor mental health (Khamis, 2019a, 2019b; McGregor et al. 2015). However, previous research (e.g. Folkman and Lazarus, 1985) has shown that people use both forms of coping in virtually every type of stressful encounter. The efficacy of problem- and avoidance-focused coping strategies is also thought to be situationally contingent (Folkman et al., 1986). Emotion-focused coping is believed to be particularly useful in situations in which the source of threat cannot be influenced, whereas problem-focused coping is thought to be most effective in situations in which threat can be altered. For example, in the families of those who were killed in the conflict, reliance mainly on emotion-focused coping may be considered effective and appropriate, since not much can be done. In contrast, in the case of families of those who were injured, resorting to emotional discharge would not be appropriate as a substitute for the direct action of seeking professional help (Khamis, 2000). Thus, the presence and type of specific daily stressors may create or promote specific coping strategies. Although there is a growing body of qualitative research on coping mechanisms that refugee parents use in caring for their children (Akesson and Sousa, 2019; El-Khani et al., 2017; Schweitzer et al., 2007), there is a paucity of literature on what coping strategies best promote refugees’ mental health in the face of the many challenges posed by adjustment to new circumstances in the host country. In particular, quantitative studies that examine coping styles differences in relation to the various forms of post- resettlement stressors and mental health in refugee parents are scarce.
One challenge of forced displacement for many refugees involves the loss of social ties in their home country and the rebuilding of their social support system in the host country (Garcıá et al., 2002). For refugee parents, a supportive social network can help alleviate adversities that arise in the process of adapting to a new environment, which can have important implications for their psychological well-being (Shin et al., 2007). Specific social factors that may be especially important for refugee mental health includes perceived social support from family and institutions (Khamis, 2000; Veronese and Pepe, 2017). Vulnerabilities recognized as major causes of psychological distress among Syrian refugees include ongoing family separation, lack of social support and social resources, such as social belonging, social support networks, and social capital (Akesson and Sousa, 2019; Cantekin and Gencoz, 2017), and lack of access to information (Care Jordan, 2012). Social support can take several forms, including emotional support (e.g. empathy, companionship), informational support (e.g. information about available services, or how to address resettlement-related stressors), and tangible support such as financial support (Kaniasty and Norris, 2009). All three forms of support are thought to play a significant role in shaping the post resettlement experience, helping refugee parents with daily stressors, and protecting against adverse mental health outcomes. Although the influence of social support on psychological well-being appears to depend on the forms of support provided (e.g. emotional vs instrumental support), the unique effects of specific forms and sources of formal and informal support (family, institutions) among Syrian refugee parents have not been examined.
Drawing on these various theoretical paradigms, this research investigates the psychosocial sequelae of forced displacement among Syrian refugee parents in Lebanon and Jordan. Three departures from previous investigations should be noted. First, previous studies on Syrian refugees in host countries were on children and adolescents (Khamis, 2019a, 2019b; Lustig et al., 2004), and excluded consideration of how resettlement bears on changes in the lives of refugee parents. Secondly, most of the studies aimed to understand the pathways through which war and displacement affect parenting and ultimately child psychosocial adjustment. (e.g. Deng and Marlowe, 2013; Sim et al., 2018) and not on how the post- resettlement experience affects the mental health status of refugee parents. Thirdly, investigators have discussed consequences of traumatic events for refugees but given limited attention to the daily stressors encountered by the refugees in the resettlement context (Miller and Rasmussen, 2010; Miller et al., 2008; Porter and Haslam, 2005).
Hypothesis
The purpose of the current study was twofold: (1) to explore whether the primary symptom dimensions of psychological distress and neuroticism in Syrian refugees vary by parents’ characteristics; and (2) to identify predictors of psychological distress and neuroticism in Syrian refugee parents. It was also hypothesized that a combination of parents’ characteristics, risk variables (i.e. normative stressors), and protective variables (i.e. variations across parents’ in coping strategies and social support) would be predictive of psychological distress and neuroticism.
This study contributes evidence on the largely understudied particularities related to refugee parents. As the Syrian crisis is relatively recent, research is important to better inform holistic interventions and culturally appropriate policy responses.
Method
Sample selection and procedure
A multistage stratified cluster sample was used to identify parents of 1000 Syrian refugee children and adolescents who fled their country during the war and now resided in Lebanon and Jordan. Data from the Ministry of Education in both countries were used to locate Syrian refugee parents. First, children were selected from the two countries (Lebanon and Jordan), representing various governorates, schools, grade levels (1–12), and both genders (see Khamis, 2019a). Second, a consent form was sent home to parents whose children were selected for the study, explaining the purpose and process for data collection.
Informed consent was obtained from 87% of the parents who were selected to participate in the study, and as a result, 130 other parents were selected as replacements. Two trained psychologists between March and June 2017 administered questionnaires in an interview format with parents at home. Completion of the interview took from 35 to 45 minutes. Ethics approval for the study was obtained from the American University of Beirut.
Measures
Demographics questionnaire
A brief questionnaire was developed to secure demographic and background information about the refugee parents including age, gender, parents’ education and employment, family size, host country, and time spent in host country since they fled from Syria.
Daily stressors
The Family Inventory of Life Events and Changes (FILE) was used to assess the pile-up of life events and changes experienced by the family in the past year (McCubbin and Patterson, 1991). The FILE questionnaire comprised 71 items, which represent critical events in various domains of life, such as intrafamily strains or difficulties in family relationships, such as strains between parents and children or between ex-spouses; marital strains; pregnancy and childbearing strain; finance and business strains; work–family transitions and strains; illness and family care strains; losses (deaths in nuclear and extended family); transitions “in and out”(children being launched or returning home after leaving); and family legal violations. Parents were asked to indicate whether the event had occurred in their family over the past year on a dichotomous scale: 0 (no), 1 (yes). The overall score on that measure ranged from 0 to 71: Higher scores indicate a greater accumulation of normative stressors. Cronbach’s alpha for the total scale was 0.92 indicating that the scale has a very good reliability.
Psychological distress
Psychological distress was assessed by the Symptom Checklist-90–Revised (SCL-90-R). The SCL- 90-R is a 90-item self-report symptom inventory that assesses psychological distress in terms of nine primary symptom dimensions and three summary scores termed global scores (Derogatis, 1983). The principal symptom dimensions are labeled Somatization (SOM), Obsessive-Compulsive (OBS), Interpersonal Sensitivity (INT), Depression (DEP), Anxiety (ANX), Hostility (HOS), Phobic Anxiety (PHOB), Paranoid Ideation (PAR), and Psychoticism (PSY). Reliability was very good. The internal consistency measures for the nine dimensions were quite satisfactory ranging between a low of 0.77 for psychoticism to a high of .90 for depression. The test−retest reliability ranged between .80 and .90 which is an appropriate level for measures of symptom constructs (Derogatis, 1983). In this sample, Cronbach’s alpha was 0.98 indicating that the scale is very reliable. There are three global indices of distress associated with the SCL-90-R, the Global Severity Index (GSI), the Positive Symptom Distress (PSDI), and the Positive Symptom Total (PST). The GSI combines information on numbers of symptoms and intensity of perceived distress. The PSDI is a pure intensity measure, in a sense, corrected for the number of symptoms. It functions very much as a measure of response style in the sense of communicating whether the person is augmenting or attenuating symptomatic distress in his or her style of reporting his or her disorder. The PST is simply a count of the number of symptoms the person reports as positive, that is, the experiences as having to any degree. In this study, only the GSI was used to assess parents’ psychological distress because it provides the most sensitive single numeric indicator of the respondent’s psychological distress, combining information on numbers of symptoms and intensity of distress ((Derogatis, 1983).
Neuroticism
Neuroticism was assessed by the neuroticism scale of the Eysenck Personality Questionnaire (Eysenck and Eysenck, 1975). Parents were asked to complete the 23-item Arabic version of the neuroticism scale (El Khalek, 1978), which asked them to answer “yes” or “no” questions about their negative affectivity. Composite scores may range from 0 to 23, with higher scores indicating higher neuroticism. Cronbach’s α for the total scale in this sample was 0.89.
Coping strategies
The Ways of Coping Questionnaire (WCQ) was used to assess a broad range of cognitive and behavioral strategies that people use to manage internal and external demands in a stressful situation (Folkman and Lazarus, 1985; Folkman et al., 1986). A large body of research supports the reliability and construct validity of the WCQ (e.g. Folkman et al., 1986). Each subscale is scored by averaging the 4-point Likert scale responses for each of the subscale items. The emotion-focused coping included distancing (e.g. “Didn’t let it get to me; refused to think about it too much”; “Went on as if nothing had happened”), avoidance (e.g. “Wished that the situation would go away,” slept/ate/drank), self-controlling (e.g. “I tried to keep my feelings to myself”). The problem-focused strategies included problem solving (e.g. “Just concentrated on what I had to do next, the next step”), seeking social support (e.g. “Talked to someone who could do something concrete about the situation”), and confrontation (e.g. “Tried to get the person responsible to change his or her behavior”). Cronbach’s alpha for the total scale in this sample was 0.94.
Social support
The refugees social support inventory is a 24 -item self-report measure that was designed for the purpose of this study. It examined to what degree immediate family members (i.e. nuclear family), collateral relatives (i.e. extended family), friends, and community (institutions) provided emotional support (expressions of empathy, love, trust, and caring), instrumental support (tangible aid and service), and informational support (advice, suggestions, and information) for refugees after they have fled their homes and resettled in their host country. Responses ranged from 1 = never to 4 = many times. The statements of RSSI were generated from previous observations and interviews with refugees and from a review of related theoretical and empirical research. Four specialists in the areas of psychology and sociology were asked to judge the overall format of the inventory and to assess each item for its presumed relevance to the property being measured. A factor analysis of 24 items, using principal components with varimax rotation, resulted in the identification of five factors that explained 64.13 % of the variance. Only items that had factor loadings of at least 0.50 were selected. Factor 1, informational support provided by institutions, explained 36.39 % of the variance. Factor 2, instrumental support provided by the family, explained 10.78 % of the variance. Factor 3, informational support provided by family, explained 1.64 % of the variance. Factor 4: instrumental support provided by institutions, explained 1.40 % of the variance. Factor 5: emotional support provided by the family, explained 1.03% of the variance. Examples of items from the RSSI included after you fled the country, how often did members of the family, relatives or institutions offered you housing, financial assistance, food, clothing, medicine, education of your children, provided assistance, gave advice, were reassuring, or listened empathically, gave you suggestions and information about whom to seek for help. Cronbach’s alpha for the total scale is 0.98.
Statistical analysis
A series of multivariate analysis of variance (MANOVA) and t- tests were employed to examine the differences in psychological distress and neuroticism and various independent variables, followed by univariate analysis. Then separate hierarchical regression models were used to predict psychological distress for the total sample. Model 1 included only the parents’ sociodemographics (i.e. gender, age, host country). Model 2 included the daily stressors (i.e. FILE) as well as the variables in Model 1. Model 3 included all the variables in Model 2 plus the coping strategies (i.e. WCQ). Model 4 included all of the variables in Model 3 plus the social support inventory (i.e. RSSI). The predictor blocks were entered in the order listed. This order was based upon chronology of occurrence. The early entry of a variable block into the regression equation provided a statistics control for the impact of those variables upon psychological distress and neuroticism. Analyses were conducted using PASW Statistics 25.0 (IBM Corp, 2017).
Results
Participants
The sample consisted of 1000 Syrian refugee parents, with an equal size from both countries (Lebanon and Jordan), of whom 456 were fathers and 544 were mothers. Parents ranged in age from 25 to 67 years (M = 39.18; SD = 8.29). Approximately 88 % of the participants reported that they were married and the remaining were singles including those who were divorced or widowed. They had a large average family size (M = 6.40; SD = 1.92). For the entire sample, the mean level of education for mothers and fathers was grade 8, with the range extending from illiteracy to graduate study. Approximately 42 % of the fathers and 4.4% of the mothers indicated that they were working. The time these parents had spent in the host country ranged from 1 to 72 months (M = 48.64, SD = 15.58).
Demographic, psychological distress, and neuroticism
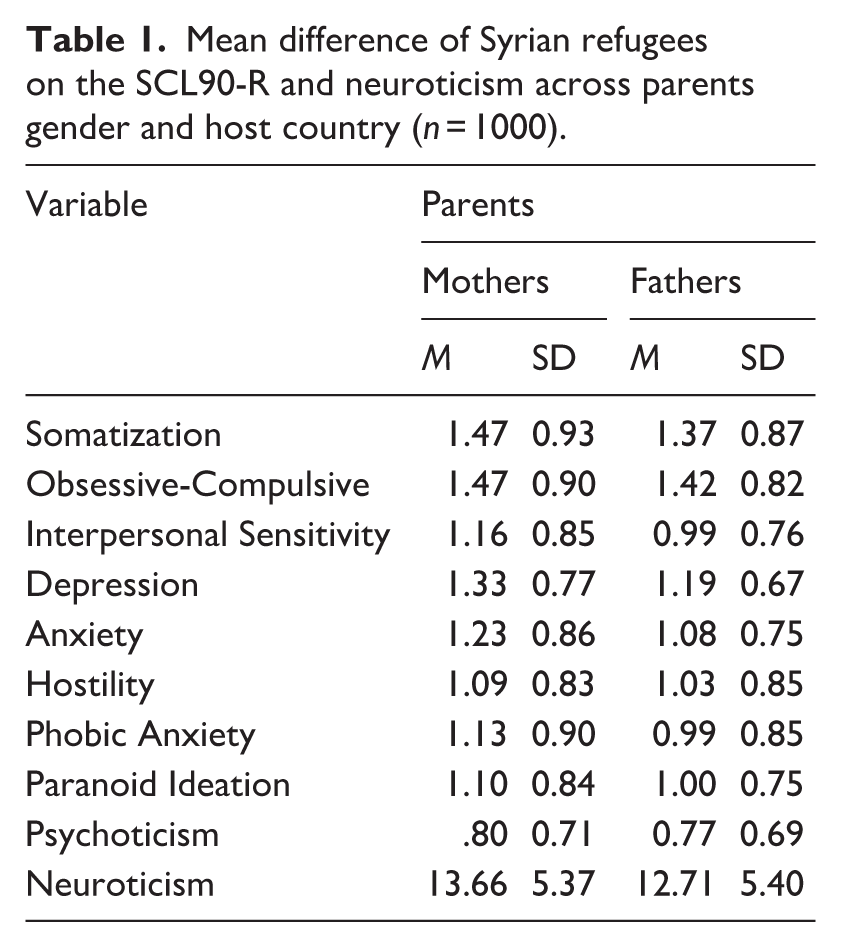
Psychological distress was determined using the nine domains of SCL90-R. Multivariate analysis of variance (MANOVA) was employed to examine differences between mothers and fathers on somatization, obsessive-compulsive, interpersonal sensitivity, depression, anxiety, hostility, phobic anxiety, paranoid ideation, and psychoticism. Results indicated a significant multivariate effect (Wilks’ λ = 0.954, F [1,997] = 5.27, p < 0.001). Follow-up t-test analyses revealed that mothers exhibited more interpersonal sensitivity t (998) = 3.33, p < 0.001, depression t (998) = 3.06, p < 0.002, anxiety t (998) = 3.04, p < 0.002, and phobic anxiety t (998) = 2.46, p < 0.01, than fathers. In addition, t-test results indicated that mothers exhibited more neuroticism compared to fathers t (998) = 2.77, p < 0.006 (see Table 1).
Mean difference of Syrian refugees on the SCL90-R and neuroticism across parents gender and host country (n = 1000).
In addition, MANOVA results indicated a significant multivariate effect (Wilks’ λ = 0.965, F [1,997] = 3.95, p < 0.001) for marital status. The t-test analyses revealed that married individuals exhibited more somatization t (998) = 3.33, p < 0.001, and neuroticism t (998) = -2.60, p < 001 than did singles.
Pearson correlation results indicated that high levels of obsessive-compulsive disorder (r = −.07, p < 0.04), and depression (r = −.10, p < 0.004) were more common among younger refugee parents whereas neuroticism was more in older refugee parents (r = .028, p < 0.001).
Refugee parents who had resettled in Jordan had higher levels of psychological distress compared to refugee parents who had resettled in Lebanon. The results were significant for all SCL90R dimensions except for the obsessive–compulsive disorders in which the effect of host country was not significant. Also, a significant effect was found for host country on neuroticism t (998) = 2.23, p < 0.02 with refugee parents who resettled in Jordan having higher scores than those who lived in Lebanon.
The results indicated that parents’ obsessive-compulsive (r = −.06, p < 0.05) and phobic anxiety (r = −.07, p < 0.05), decreased significantly with the passage of time spent in the host country.
Prediction of psychological distress
Regression results are presented in Tables 2 and 3; table entries reflect the effect size attributable to each predictor variable when other variables in the equation are held constant (i.e. squared semi-partial correlation). Table 2 indicates that the total variance in psychological distress scores explained by the model was 43.4 %. Each predictor block separately accounted for the following percentage of parents’ psychological distress variance: 4.2 % by parents’ sociodemographics, 17.7 % by daily stressors, and 20.6 % by coping strategies, and .009 by social support. The absolute increase in R2 is small for parents’ sociodemographics, .042; and social support, .009; and medium for daily stressors, .177; and coping strategies, .206. Cohen’s (1988) guidelines for small, medium (those typical in behavioral research), and large effect sizes are .02, .15, and .35, respectively. In Table 2, the column denoted beta contains the standardized or beta coefficients of the 26 individual variables contained in the model. The absolute magnitude of the beta coefficients indicated the relative strength of 26 variables as predictors of parents’ psychological distress.
Regression weights for hierarchical models predicting psychological distress (GSI) in refugee parents.
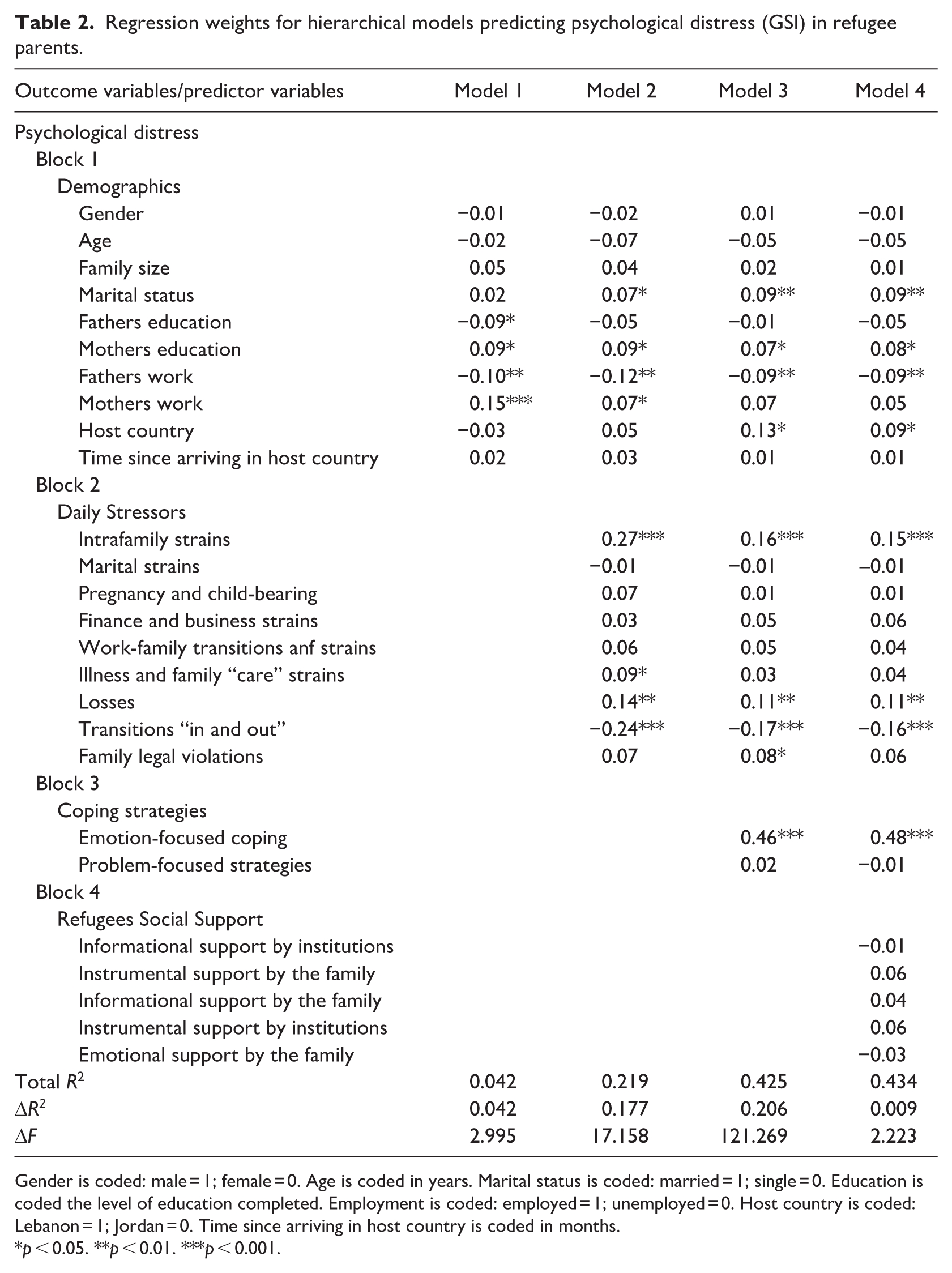
Gender is coded: male = 1; female = 0. Age is coded in years. Marital status is coded: married = 1; single = 0. Education is coded the level of education completed. Employment is coded: employed = 1; unemployed = 0. Host country is coded: Lebanon = 1; Jordan = 0. Time since arriving in host country is coded in months.
p < 0.05. **p < 0.01. ***p < 0.001.
Regression weights for hierarchical models predicting neuroticism in refugee parents.
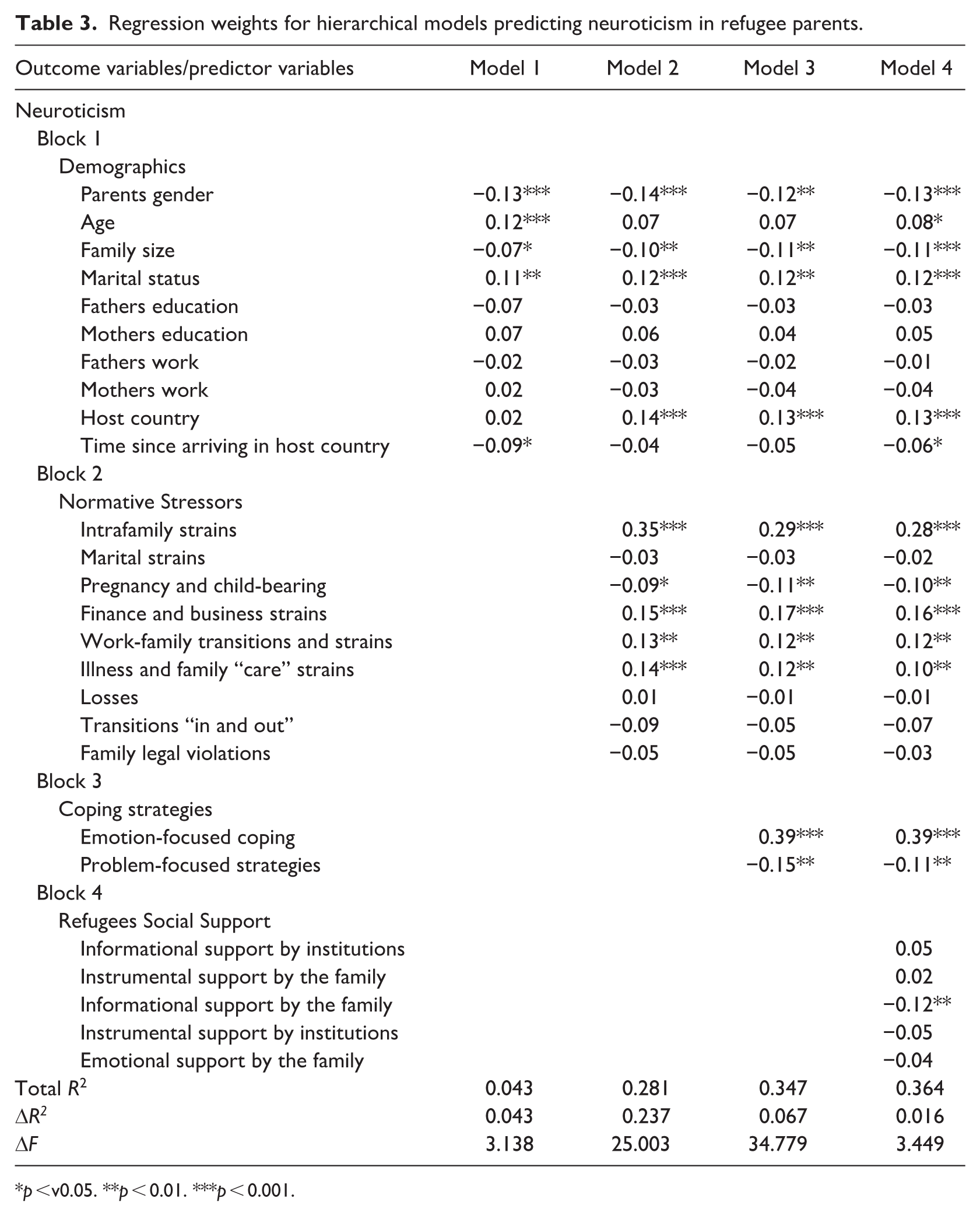
p <v0.05. **p < 0.01. ***p < 0.001.
In the first step marital status, mothers’ education, father’s work, and host country significantly predicted GSI, indicating that the partnered parents, mothers with higher levels of education, unemployed fathers and parents who resettled in Lebanon scored higher in GSI compared to the singles, mothers with lower levels of education, employed fathers and parents who resettled in Jordan. All the other demographic variables were not significant predictors including gender, age, family size, father’s education, mother’s work, and the passage of time spent in the host country.
Among daily stressors, intrafamily strains, losses, and transitions in and out were related to GSI. Parents who reported more family stressors and losses had higher GSI scores whereas parents who reported more transitions in and out had lower levels of GSI.
As for the coping strategies, parents who used emotion-focused coping reported higher levels of GSI. Problem-focused coping was not a significant predictor.
In reference to social support, none of the social support variables appeared to be significant predictors at the family and institutional level.
Prediction of neuroticism
Table 3 indicates that the total variance in neuroticism scores explained by the model was 36.4 %. The absolute increase in R2 is small for parents’ sociodemographics, .043; coping strategies, .067; and social support, .016; and medium for daily stressors, .237.
Of the sociodemographic characteristics, gender, age, and marital status had a statistically significant B weighting, suggesting that mothers, older participants, and the married people reported higher levels of neuroticism compared to fathers, younger participants, and singles. Family size was a significant predictor, indicating that parents who live with large families have lower levels of neuroticism.
Also, host country was a significant predictor with parents who were in Lebanon having higher levels of neuroticism compared to parents who lived in Jordan. In addition, parents who had spent more time in the host country reported a decrease in the levels of neuroticism.
Among the various daily stressors, intrafamily strains, pregnancy, financial strains, and illness-related strains were related to neuroticism. Parents who reported more family stressors, financial strains and illness strains had higher neuroticism scores whereas parents who reported more pregnancy strains had lower levels of neuroticism.
As for the coping strategies, parents who used emotion-focused coping reported higher levels of neuroticism. Problem-focused coping was not a significant predictor.
In reference to social support, none of the social support variables appeared to be significant predictors at the family and institutional level except for informational support provided by the family.
Discussion
The findings regarding the relation between psychological distress and predictors in Syrian refugee parents were revealing.
Consistent with previous studies, the results indicated that mothers had higher levels of psychological distress and neuroticism compared to fathers. This finding was in line with previous evidence about family roles: Motherhood is often associated with psychological distress (Van Ee et al., 2012, 2016). Although the exact reasons behind these parental role disparities remain uncertain, differences in psychological distress may be due to changes in social roles, which influence the stressors to which people are exposed and to the personal and social mediating resources that can be utilized to deal with hardship. Research has indicated that changes in gender roles among refugees have created intense levels of stress for women. Women are burdened with the dual responsibilities of their reproductive and family roles and often also of assuming the men’s responsibilities as economic providers in host countries (Care, 2020; El-Masri et al., 2013). Understanding parental roles in psychological problems requires being aware of gender-role constructs, which may very well affect the type of stressors that exist, their associated symptoms and people’s response to their problems (Khamis, 2000, 2014). Further, the dual nature of gender and refugee status for Syrian mothers are often stressful experiences, beginning with early marriage, exploitation at work and continuing to current inequities in social resources (IPSOS Group SA, 2018; UNICEF, 2017).
Contrary to previous research, the results showed that partnered parents were at higher risk of subsequent psychological distress than were divorced, widowed, or seperated parents (Baruch and Barnett, 1986). This finding may be attributed to the post- resettlement changes that increased marital conflict between refugee couples in the host countries such as increased poverty and economic hardship, long or irregular working hours, changes in gender roles and responsibilities (Hyman et al., 2008) as well as aggression, and intimate partner violence against women (Wachter et al., 2018).
Consistent with previous research, the results of the study indicated that higher educational attainment of mothers appeared to be a heightened vulnerability that increased the risk for higher levels of psychological distress (Brännlund and Edlund, 2020), whereas fathers’ employment was associated with lower levels of psychological distress (Warfa et al., 2012).
These results do not imply that higher educational attainment per se leads to poorer mental health. They rather suggest that refugees experience smaller economic returns from schooling and that education is likely to intersect with multiple forms of resources such as father’s employment (Krahn et al., 2000). Consistent with previous research the results showed that neuroticism increased with age (Gerritsen et al., 2006; Laban et al., 2008). The results also showed that family size was negatively related to neuroticism. This is especially valid within the range of this study data. Children in large families are regarded as sources of support which can have a positive impact on physical and mental health (Eriksen and Gerstel, 2002; Moor and Komter, 2011). Research has indicated that Syrian refugee families reported increased family closeness and communication (Akesson and Sousa, 2019), and as a result families of a large size could have significant benefits for the well-being of both refugee children and their parents. Previous research on Syrian refugee children provided a rich picture of the potential protective factors operating within the family environment (Khamis, 2019a, 2019b).
In addition, parent’s neuroticism decreased significantly with the passage of time spent in the host country. This finding is in line with other studies (Porter and Haslam, 2005; Steel et al., 2002) which found that the greater the time spent in the host country the more positive the effect on the mental health of refugees.
Consistent with previous research on refugees, the results of this study have found some evidence for the impact of life events and changes on mental health (Li et al., 2016) with a distinction between positive and negative life events. Furthermore, the various types of stressors had differential effects on various mental health outcomes. For example, intrafamily strains were found to be positively related to both mental health outcomes (psychological distress and neuroticism), whereas finance and business strains, work-family transitions and strains, illness, and family care strains were related to neuroticism, and losses were particularly problematic for psychological distress. In contrast, transitions “in and out” were negatively related to psychological distress; and pregnancy and child-bearing were negatively related to neuroticism.
The findings indicate that emotion-focused coping is closely linked to psychological distress and neuroticism whereas problem-focused coping was associated with less psychological distress but not neuroticism. When both types of coping were considered simultaneously after controlling for a number of potential confounding variables, emotion-focused coping was linked with greater psychological distress in both domains: psychological distress and neuroticism. In contrast, problem-focused coping was associated with less psychological distress but not in neuroticism. These results support the assertion that reliance on negative coping such as an emotion-focused coping style contributes to persistent psychological distress, and neuroticism, and that problem-focused coping is associated with reduced neuroticism and PTSD symptoms (Huijts et al., 2012; Littleton et al., 2007; Taylor and Stanton, 2007). These results represent two distinct strategies for intervention. A reduction of emotion-focused coping may lessen future psychological distress symptoms whereas problem-focused coping may improves refugee parents functioning.
Of the various types of social support only informational support provided by the family was significantly associated with neuroticism. Indeed, previous studies have indicated that refugees sought informational support such as advice and suggestions from peers, relatives and friends that helped solve problems and explain circumstances, (Berkman and Glass, 2000; House, 1981). For refugees, a key protective mechanism came through informational supports—informing refugee children and their parents about services or preparing them for obstacles they might encounter in their host country (Weine et al., 2014). This stands in contrast to previous research that supports the link between social support and mental health among refugees (Schweitzer et al., 2006), others do not (Alemi et al., 2017).
Strengths, limitations and future directions
This study has numerous strengths: a quantitative research design, a large sample drawn from two host countries, two measures of mental health outcomes, and a focus on refugee parents. There are also limitations that should be acknowledged. First, the study is cross-sectional in nature; longitudinal research is needed for elucidating the directionality of the relationship between post-resettlement stressors and psychological distress. Secondly, as with any study utilizing retrospective self-report, there is the possibility of bias and distortion. Thirdly, as this is a sample of parents of school-age children, the findings cannot be generalized to the overall population of refugee parents (e.g. unregistered refugees, refugee camps) in Lebanon and Jordan. Further empirical inquiry is required to determine whether the findings of this study will generalize to unregistered refugees and to refugee parents who resettled in other countries and cultures with distinct backgrounds and traditions. Results suggest that optimal impact on mental health could be attained through the development of policies that work to protect the rights of Syrian refugees with mental health disorders in a variety of settings, including the workplace, schools, and in treatment. Together, these findings help to clarify the longstanding argument that daily stressors are central to mental health by showing that their role is important but crucially dependent on which stressors (e.g. work strains, family roles) and types of effects (e.g. psychological distress, neuroticism) are being considered.
Conclusion
The results of this study contribute to the growing literature highlighting the adverse effects of post- resettlement stressors on the mental health of refugee parents. The findings provide strong support for the powerful associations between sociodemographic characteristics, family roles, and refugees’ psychological status in the resettlement contexts. In addition, various types of daily stressors had differential effects on psychological distress and neuroticism with a distinction between positive and negative life events. The findings also highlight the important distinction between emotion-focused coping and problem-focused coping given that these constructs are differentially associated with psychological distress. This study also identifies the significance of informational support in protecting refugee parents against psychological distress and neuroticism. These results point to the need for social policies and interventions that focus on reducing proximal daily stressors that are salient to Syrian refugee parents in their host countries and that would meet refugees’ needs for security, work, health, and wellbeing. Interventions focusing on communication and problem-solving skills among parents may have promise in decreasing psychological distress and neuroticism in the resettlement communities (Khamis, 2019b) and may contribute to maintaining good mental health. In addition, the results illustrate the need for an ongoing collaborative effort of all stakeholders to improve the understanding of refugee parents’ mental health needs, and the effectiveness of the available resources.
Footnotes
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.