
Abstract
The Pandemic Anxiety Inventory (PAI) assesses anxiety symptoms individuals attribute to the presence of a pandemic. We conducted this study of 379 British adults during the COVID-19 pandemic and found that the PAI exhibited excellent reliability and solid criterion validity. Pandemic anxiety was associated with reduced social support, anticipated life changes, financial strain, job loss, economic insecurity, and the hospitalization or death of a close friend or relative. Using correlational and bifactor analyses, we found that the PAI demonstrated solid convergent and discriminant validity. The findings suggest that the PAI can be used in research and clinical practice.
Keywords
In December 2019, an outbreak of SARS-CoV-2, also known as COVID-19, occurred in China and soon spread around the world. By January 17, 2022, health authorities in the United Kingdom reported almost 152,000 deaths from COVID and more than 15,300,000 cases worldwide (GOV.UK, 2022). Also on January 17, 2022, the Centers for Disease Control and Prevention (2022) reported that there had been almost 850,000 COVID-related deaths in the United States and more than 65,000,000 cases.
Research has identified several psychological sequelae of the COVID pandemic and related public health policies (e.g. lockdowns). Notably, the pandemic has been associated with elevated levels of depressive symptoms (Targa et al., 2021), fatigue (Goërtz et al., 2020; Michel et al., 2021), sleep disturbance (Wang et al., 2021), reduced life satisfaction (Mei et al., 2022), and excessive alcohol consumption (Tudehope et al., 2021).
The focal concern of this paper is a different set of psychological symptoms, pandemic-related anxiety symptoms. Anxiety can influence behaviors that impede or accelerate the spread of a virus (Taylor et al., 2020). It is therefore important to develop a measure of pandemic-related anxiety. Our aim was to examine the validity of the recently developed Pandemic Anxiety Inventory (PAI). Anxiety is initially a normal psychological response to threat. COVID-19 has been a threat of such great magnitude that it is likely that levels of anxiety in the general population have increased substantially. People have learned that friends and loved ones have gotten sick and gone to hospitals for intensive care. Others have died. The COVID pandemic has led to economic dislocation and financial hardship. Travel to see friends and relatives has been curtailed. Those sickened and people exposed to them have had to quarantine. There is considerable evidence that COVID-19 is related to increased levels of anxiety (Li et al., 2021; Myran et al., 2022; Santabárbara et al., 2021; Xiao et al., 2020).
Existing measures of COVID-related anxiety and the PAI
For research and practice, it would be helpful to have an instrument assessing the extent to which individuals experience anxiety symptoms that they expressly attribute to the pandemic. The Coronavirus Anxiety Scale (CAS), which was developed by Lee (2020) and Lee et al. (2020a, 2020b, 2021), assesses anxiety related to the COVID-19 pandemic. Two other psychological symptom scales that were developed in response to the COVID-19 pandemic are the COVID Stress Scales (CSS; Taylor et al., 2020) and the Fear of COVID-19 Scale (FCV-19S; Ahorsu et al., 2020; Giordani et al., 2022; Sawicki et al., 2022).
The newer PAI differs from existing COVID-related instruments in several ways. The PAI is directed at assessing anxiety symptoms that develop in the context of any pandemic, not just the COVID-19 pandemic; the CAS is not. Because pandemics reoccur (Samarasekera, 2021), it is important to have such an instrument available. The CSS was developed to be easily adjusted to work in the context of future pandemics (Taylor et al., 2020).
The CAS covers five anxiety symptoms an individual may experience when exposed to information about the coronavirus. The CSS comprises 36, mostly “worry” items. Given the CSS’s length, the instrument can be burdensome to respondents. In contrast to the CAS and the CSS, the PAI and the FCV-19S are in-between, limited to 10 and 7 symptom items, respectively, although the PAI includes two complementary items. The PAI contrasts with the CAS, CSS, and FCV-19S in that the PAI’s items are derived directly from the symptoms of generalized anxiety disorder (GAD) found in the Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM-5; American Psychiatric Association, 2013). We selected these symptoms for two reasons. First, everyone sometimes experiences anxiety; our concern is for anxiety that is excessive. Second, GAD, which is common in high-income countries like the UK and US, is comorbid with other anxiety disorders and mood disorders, interferes with management of home and work life, and adversely affects close relationships (Ruscio et al., 2017). The PAI has a little overlap with symptoms on the other scales. For example, the PAI and the CAS overlap on one symptom, sleep difficulties. The overlap with other COVID-related worry/anxiety scales is limited. The PAI includes symptoms of excessive anxiety, difficulty controlling worry, restlessness, fatigue, cognitive impairment, irritability, muscle tension, and sleep difficulties.
Based on the DSM-5, we also included in the PAI two items that complement the symptom items. One complementary item asks the respondent about the extent to which anxiety symptoms affect the individual’s functioning. The other complementary item asks about major life changes respondents may be considering in response to anxiety symptoms they experienced. These items can help a clinician better understand the individual in care.
Hypotheses
We developed several hypotheses bearing on the validity of the PAI. Noting that social support is inversely related to anxiety in many facets of life (Asselmann et al., 2020; Gonzalez-Saenz de Tejada et al., 2017), including COVID-linked anxiety (Gonzalez-Saenz de Tejada et al., 2017; Khoury et al., 2021; Labrague and Santos, 2020; Rückholdt et al., 2021), we hypothesized that scores on the PAI would be inversely related to support. Other criterion-related hypotheses were also based on the anxiety literature. We hypothesized that the PAI would be negatively related to the male sex (García-Fernández et al., 2021), age (Solomou and Constantinidou, 2020; Wittenborn et al., 2020), and financial resources (Racine et al., 2021; Rudenstine et al., 2021). We also hypothesized that the PAI would be associated with COVID-related and non-COVID-related traumatic stress (Lahav, 2020; Masiero et al., 2020) and sleep problems (Jahrami et al., 2021; Wang et al., 2021). From the standpoint of a desire to damper disease-related anxiety, we anticipated that those with higher levels of pandemic-related anxiety would be more likely to consider major life changes (Ferreira et al., 2021; Hedman et al., 2016). In addition, we hypothesized that pandemic-related anxiety symptoms would be related to participants’ subjective estimates of how widespread the disease was in their localities.
The methods used to evaluate the PAI in the present study contrast with previous methods used to assess COVID-related anxiety. For example, we assessed the PAI’s reliability with McDonald’s (1999) omega, a more sophisticated approach to assessing reliability than Cronbach’s alpha. We evaluated the question of the unidimensionality of the PAI using confirmatory factor analysis (CFA). As for convergent validity, we anticipated that the PAI would correlate highly with measures of cause-neutral anxiety, everyday functioning, and stress symptoms. We further assessed the PAI’s convergent validity, along with discriminant validity, by conducting an exploratory structural equation modeling (ESEM) bifactor analysis (Rodriguez et al., 2016) with a partially specified target rotation (PSTR; Marsh et al., 2014). Two hypotheses regarding convergent and discriminant validity were evaluated vis-à-vis cause-neutral anxiety symptoms. Regarding convergent validity, we hypothesized that the PAI symptom items and cause-neutral anxiety symptom items would load highly on a general factor. Regarding discriminant validity, we hypothesized that, because PAI items assess pandemic-linked anxiety and the cause-neutral items assess anxiety more generally, the PAI and cause-neutral items would load highly (⩾0.30) on separate bifactors (specific factors). A similar procedure was employed in assessing the convergent and discriminant validity of the recently developed Occupational Depression Inventory (Bianchi and Schonfeld, 2020).
Methods
Participants
A total of 424 individuals were recruited. Eligibility criteria included living in the United Kingdom and being 18 years of age or older. We excluded 28 individuals who did not respond to any of the PAI items, the focal interest of the study. Another nine individuals were excluded because they answered affirmatively to an item asking if they responded randomly to the survey items. An additional eight individuals who failed to respond to the item asking about random responding were excluded.
The final number of participants was 379 (Mage = 33.21, SDage = 12.24) of whom 257 (67.8%) were women and 119 (31.4%) were men; 3 (0.8%) participants did not identify their gender. A total of 319 (84.2%) were White and 60 (15.8%) were Non-White. The median income of the sample was ₤50,000–₤54,000 (the interquartile range was ₤30,000–₤34,000 to ₤70,000–₤74,000). One hundred eighty respondents (47.5%) were not married or in a relationship and 199 (52.5%) were. Only 3% of the sample did not have at least some college or university training.
Data collection took place online from May to August 2021. Recruitment advertisements detailing study aims and eligibility criteria were publicized on social networking sites (e.g. Facebook, LinkedIn). Qualtrics© XM (Qualtrics, Provo UT, 2020) hosted the survey. An electronic link directed participants to read an information sheet and a consent form. They were asked to provide consent by selecting “I agree to all the above statements (e.g. being age 18 or older) and consent to participate in this research study.” After providing consent, participants were directed to complete the questionnaire. Internet surveys are as reliable and valid paper-and-pencil measures (Gosling and Mason, 2015). The study was approved by the human subjects committee at the University of Surrey.
PAI
Two of the authors (ISS and RB) developed the items for the PAI. The items were rationally based on the symptoms described in DSM-5 for generalized anxiety disorder (American Psychiatric Association, 2013). Respondents were asked to report on symptoms they experienced over the course of the last month (M = 1.731; SD = 0.601; Cronbach’s alpha = 0.924). Unlike most standard anxiety measures, which present symptom items in a “cause-neutral” manner (e.g. the Hospital Anxiety and Depression Scale), the items in the PAI are worded in such a way as to ask participants if they attribute any symptom to the pandemic (e.g. I felt nervous or anxious or on edge because of the pandemic). 1 Items are rated on a 4-point scale, from 0 (“Never or almost never”) to 3 (“Nearly every day”). Participants were instructed to check 0 if they experienced a symptom for a reason they considered unrelated to the pandemic (e.g. relationship problems) or for a reason they could not identify. The items were recoded to range from 1 to 4.
The PAI concludes with two complementary items. One item asks the participant to respond “No,” “Yes,” or “I don’t know” to a question about having considered making major life changes in response to the symptoms mentioned in the main part of the scale. The second item asks respondents to rate the extent to which the symptoms affected their everyday functioning. The response alternatives range from 1 for “Not at all” to 5 for “Very strongly.” The PAI can be found in the Supplemental Material.
Three items assessing cause-neutral anxiety
The survey included three cause-neutral anxiety items (M = 1.792; SD = 0.623; Cronbach’s alpha = 0.796). Two items (e.g. “I found myself becoming agitated”) came from the Depression, Anxiety & Stress Scales (Antony et al., 1998; Lovibond and Lovibond, 1995). The third, “I dreaded things I had to do,” was a slight variation of an item from Goldberg’s (1972) 140-item General Health Questionnaire. The items were worded with a minimum of overlap with the wording of the PAI items. The response alternatives ranged from “Did not apply to me” (1) to “Applied to me very much or most of the time” (4).
Social support
To assess social support, we used Schonfeld’s (2001) 8-item abridged version of Cohen et al.’s (1983) Interpersonal Support List (e.g. “When I have some free time, I often meet or talk on the telephone or the Internet with friends”). Items were scored from “Definitely true” (1) to “Definitely false” (4). One item, “If I needed a lift very early in the morning, I would have a hard time finding someone to take me,” was reverse scored. We made a slight change from dollars to pounds in an item that asked about having a friend who, in an emergency, could provide the respondent a loan. The scale assesses perceived support rather than received support. A problem with measures of received support is that such measures are confounded with the incidence of stressors (Schonfeld, 1991). Finally, we recoded the entire scale such that higher scores represented more support (M = 3.227; SD = 0.485; Cronbach’s alpha = 0.786).
Stress
We assessed (with slight changes in punctuation) symptoms of stress using Elo et al.’s (2003) validated single-item scale (M = 2.760; SD = 1.040). The item reads as follows: “Stress means a situation in which a person feels tense, restless, nervous, or anxious, or is unable to sleep at night because his or her mind is troubled all the time. Do you feel this kind of stress these days?” The response alternatives on this Likert scale ranged from “Not at all” (1) to “Very much” (5).
COVID-related questions
To better understand participants’ experience of the COVID-19 pandemic, we presented a series of mostly Yes-No questions to the participants. The questions concerned whether the individual had the disease, was hospitalized for the disease (only five were, too few for analyses), had been vaccinated against COVID-19, whether a close friend or relative had the disease or had been hospitalized with COVID-19, whether a close friend or relative died from COVID-19, or experienced any other type of trauma. In addition, the participants were asked to provide their own estimate of how widespread COVID-19 was in the area in which they lived. Response choices ranged from “Not widespread at all” (1) to “Very widespread” (4).
Sleep and fatigue
Participants were posed two global, single-item scales. With the Sleep Quality Scale (SQS), participants rated the quality of their sleep over the past 7 days (Snyder et al., 2018). The SQS is a validated scale that ranges from “Terrible” (0) to “Excellent” (10) (M = 5.730; SD = 2.010). Their fatigue was assessed with Van Hooff et al.’s (2007) validated, single-item scale (“How fatigued do you currently feel?”). Response alternatives ranged from “Not at all” (1) to “Extremely” (5) (M = 2.820; SD = 1.100).
Other life stresses related to COVID-19
Finally, participants were asked three Yes-No questions about the personal impact of the pandemic. The questions asked if they experienced financial strain, job loss, and job insecurity.
Data analysis
To study the criterion and convergent validity of the PAI, Pearson correlation coefficients for continuous variables were calculated. For criterion validity purposes, t-tests and one-way ANOVAs were used to examine the relation of several categorical variables to mean scores on the PAI. We used Mplus 8.1 (Muthén and Muthén, 2018) to conduct the CFA required to calculate the PAI’s omega reliability coefficient and to check model fit.
ESEM bifactor analysis (Marsh et al., 2014) was employed to evaluate the convergent and discriminant validity of the PAI symptom items vis-à-vis the three cause-neutral anxiety items. All items were treated as ordinal here and in the CFA. We employed a PSTR, with an oblique bifactor rotation, hypothesizing that items on both scales would load highly on a general anxiety factor. However, because the PAI assesses pandemic-attributed anxiety symptoms in contrast to the three cause-neutral anxiety symptoms, we specified two bifactors, one for the PAI items and the other for the cause-neutral items. We expected a degree of discriminant validity would be evident by virtue of the loadings on the bifactors. Bifactors are orthogonal to the general factor.
Results
Table 1 presents the correlations involving the PAI and other continuous measures. The table indicates that the PAI was highly related to the three-item, cause-neutral anxiety scale; the stress symptoms measure; and the measure of everyday functioning. The PAI was also related to reduced sleep quality and increased fatigue. Older individuals and individuals with greater financial resources tended to experience lower levels of pandemic-related anxiety symptoms. As shown in the note under Table 1, the correlation of the PAI with either sleep quality or fatigue was barely affected when either a sleep item or a fatigue item was deleted from the PAI scale score.
Correlations among pandemic anxiety inventory and other continuously measured factors.

PAI is the pandemic anxiety inventory. Cause-neutral anxiety represents the scale comprising three cause-neutral anxiety items. We recalculated the PAI–Sleep Quality correlation after deleting the one sleep item from the PAI. The correlation was reduced to −0.207. We recalculated the PAI–Fatigue correlation after deleting the one fatigue item from the PAI. The correlation was 0.307.
p < 0.001. **p < 0.01. *p < 0.05. t < 0.10.
Table 2 displays t-test findings bearing on binary categorical variables as well as the relevant effect sizes (a rule-of-thumb with Cohen’s d suggests that d = 0.20 represents a small effect, d = 0.50, a medium effect; and d = 0.80, a large effect). The table indicates that women had a higher mean PAI than men, with a medium effect size. Individuals who were neither married nor in a relationship had a marginally higher mean PAI than their counterparts who were married or in a relationship. Racial differences in mean PAI were not significant. The mean PAI was highly related to the individual considering major life changes; the effect size was commensurately large. Mean PAI was significantly related to financial strain, job insecurity, and losing one’s job; effect sizes were medium. Having had COVID was not significantly related to a higher mean PAI score.
Mean scores of different groups on the pandemic anxiety inventory.

v indicates that, based on a test of homogeneity of variance, we did not assume equal variances in the two groups in the t-test. ES = effect size.
Although having a close friend or relative with COVID was not significantly related to an elevated mean PAI, having a close friend or relative who was hospitalized with COVID or having a close friend or relative who died from COVID was related to an elevated mean PAI, with effect sizes ranging from small to large. In addition, individuals who experienced other types of trauma also showed a significantly higher mean PAI, with a small-to-medium effect size. These other types of trauma included being unable to see relatives living a distance away, breakup of a relationship, bereavements, diagnosis with a serious disease other than COVID (e.g. cancer), death of a close friend or relative, etc.
We also found that mean scores on the PAI were related to how widespread the participant believed the virus to be in his or her local area: Group 1 (“Not at all”), M = 1.445 (SD = 0.506, n = 60); Group 2 (“Somewhat widespread”), M = 1.660 (SD = 0.528, n = 181); Group 3 (“Quite widespread”), M = 1.881 (SD = 0.633, n = 93); and Group 4 (“Very widespread”), M = 2.093 (SD = 0.687, n = 45). The eta2 for the widespread variable was 0.101, corresponding to a medium-to-large effect. The differences were significant, F (3, 375) = 14.062, p < 0.001. Tukey post hoc tests indicated that the means of Group 1 and 2 were significantly (p < 0.05) different from the means of Groups 3 and 4. We, however, found no significant mean PAI differences among individuals who had gone unvaccinated (M = 1.671, SD = 0.590, n = 63), had one vaccination (M = 1.798, SD = 0.640, n = 122), or had two vaccinations (M = 1.709, SD = 0.579, n = 194), F(2, 376) = 1.184.
The CFA results indicate that the model fit for the 10 PAI symptom items loading on latent Pandemic Anxiety was satisfactory (RMSEA = 0.074; CFI = 0.990; TLI = 0.988; SRMR = 0.031). Figure 1 displays a diagram with the standardized loadings. Using the CFA results, the reliability of the PAI was calculated and found to be excellent, with omega equal to 0.954. The omega result implies that PAI scores correlated with the underlying factor 0.977.
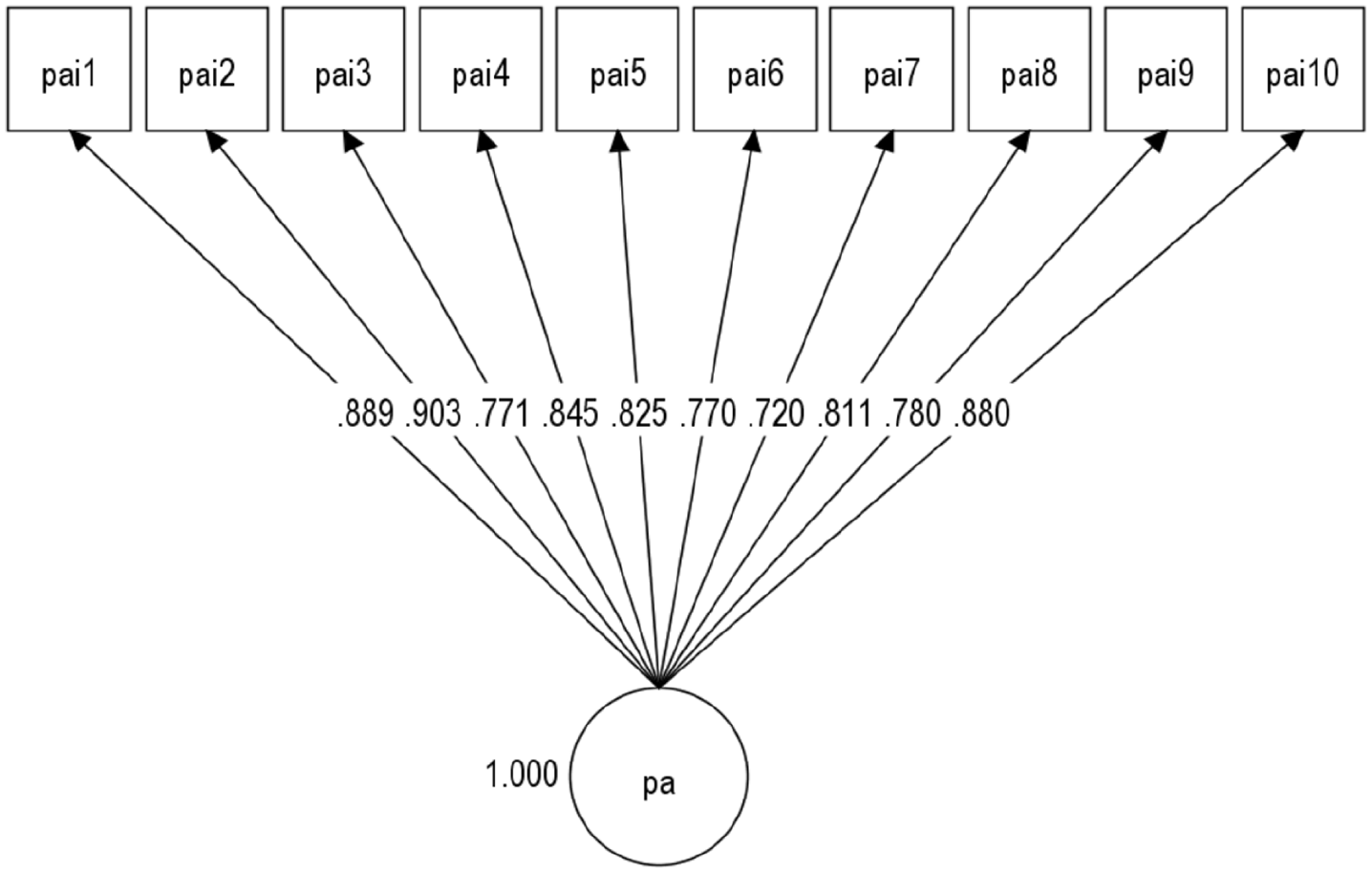
Standardized factor loadings of the pandemic anxiety inventory items on the latent pandemic anxiety factor.
For purposes of studying the convergent and discriminant validity of the PAI, we ran an ESEM bifactor analysis of the 10 PAI symptom items and the 3 cause-neutral anxiety items. Using PSTR, we modeled a general factor and two bifactors, one for the PAI items and one for the cause-neutral items. The results, which are in Table 3, show a general factor on which all items loaded highly and two bifactors on which the items on the two scales secondarily loaded and differentiated themselves (RMSEA = 0.050, CFI = 0.995, TLI = 0.991; SRMR = 0.020). More than half the PAI items loaded >0.30 on the first bifactor; all the cause-neutral items loaded >0.30 on the second.
Loadings from the ESEM bifactor analysis with partially specified target rotation of the PAI items and the three cause-neutral anxiety items.

Discussion
The general aim of the study was to examine the psychometric and structural properties of the PAI. Several findings emerged to indicate that the PAI is a valid instrument. First, the PAI, as reflected in the coefficients alpha or omega, was highly reliable. Second, regarding criterion validity, the PAI, as hypothesized, was related to fatigue, considerations for a major life change, and beliefs about how widespread the virus was in the respondent’s locality. The PAI was related, in the expected direction, to social support, being female, financial strain, job insecurity, job loss, hospitalization and death of someone close, and other traumatic events (García-Fernández et al., 2021; Gonzalez-Saenz de Tejada et al., 2017; Khoury et al., 2021; Lahav, 2020; Masiero et al., 2020; Racine et al., 2021; Rückholdt et al., 2021; Rudenstine et al., 2021; Solomou and Constantinidou, 2020; Wang et al., 2021; Wittenborn et al., 2020).
Third, the PAI, as per the CFA, demonstrated high factorial validity and showed unidimensionality. Fourth, regarding convergent validity, correlational evidence indicated that the PAI had high zero-order correlations with measures of cause-neutral anxiety, everyday functioning, and stress symptoms. The ESEM bifactor analysis took a granular approach to convergent validity, demonstrating that the PAI items and cause-neutral anxiety symptom items had solidly high loadings on the general factor. The PAI and cause-neutral items, however, also showed a degree of discriminant validity with distinct patterning in their loadings on the two specified bifactors.
The PAI compares favorably with the CAS, CSS, and FCV-19S as a measure of psychological symptoms. Unlike the research on the aforementioned instruments, we examined the relationship of the pandemic-related anxiety symptoms to social support and a host of other factors; these factors included a variety of traumatic events (Masiero et al., 2020), such as the COVID-related hospitalization of a close friend or relative and death of a close friend or relative.
We examined income and job loss. Although we used different methods, our results, like that of Taylor et al. (2020), indicate that personal economic instability is related to higher pandemic-linked psychological symptoms. According to the Resolution Foundation (2021), in the UK, where the present study was conducted, the safety net during the COVID-19 pandemic was not as sturdy as the safety net in neighboring countries like France or Germany; the living standards in British households suffered commensurately more. Our study and the study by Taylor et al. (2020) highlight the importance of having in place a financial safety net to mitigate the economic dislocation a pandemic can cause. The research on the PAI also underlines the importance of having supportive others in one’s life during a pandemic. Psychological support is potentially more helpful than instrumental support (Zysberg and Zisberg, 2022).
A finding supportive of the validity of the PAI is that scores on the instrument varied with the magnitude of respondents’ estimates of the extensiveness of the pandemic in their local communities. Although we were unable to assess the health authorities’ more objective assessments of the prevalence of the pandemic in the respondents’ localities, it would be of interest to assess the realism of local residents’ subjective estimates.
Limitations
The study has at least four limitations. First, we relied on a convenience sample that is unlikely to be representative of the UK population. For instance, the sample overrepresented individuals who had some college or more education. It would be helpful to have individuals with more diverse socioeconomic backgrounds. We also recommend that the PAI be translated and studied in different national groups, including countries, regions, and localities in which the prevalence of the pandemic varies. While variations in pandemic-related anxiety among national groups are likely, measurement invariance analysis could help estimate the extent to which the PAI has a similar structure, or meaning, across such groups (see Bianchi et al., 2022). Second, the study was cross-sectional, thus preventing an assessment of test-retest reliability and temporal relationships among the variables of interest. A third limitation is that we could not learn why a small number of participants declined to identify their gender. We did not include a non-binary category, an underrepresented group. Fourth, some of our criterion variables were single-item scales. By using several single-item scales, we could cover many characteristics that multi-item scales cover at the cost of being more burdensome to respondents (Bowling, 2005). Although multi-item measures are generally desired (Fisher et al., 2016), single-item scales have greater reliability and validity than are often credited to them (Mõttus et al., 2019). For example, a single-item scale assessing self-rated health is a good indicator of overall health and predicts mortality (DeSalvo et al., 2006; Idler and Benyamini, 1997).
Conclusions
CFA and ESEM bifactor results underline the structural and psychometric validity of the PAI and its potential for use in research and clinical practice. The instrument is reliable. The results show evidence of criterion validity vis-à-vis important variables, including fatigue, consideration of a major life change, beliefs about the local prevalence of the virus, the hospitalization or death of someone close, and other traumatic events. The PAI’s inverse relation to social support suggests that support can be helpful in reducing pandemic-related anxiety symptoms as long as the support is perceived to be available. The relation of pandemic-linked anxiety to financial strain, job insecurity, and job loss is also consistent with the idea that an improved economic safety net would help individuals whose financial situation has been harmed by the pandemic.
One future application of the PAI would involve a study of the relation of pandemic-linked anxiety symptoms to fluctuations in the incidence, prevalence, and mortality rates of a pandemic disease (cf. Sønderskov et al., 2021; Vistisen et al., 2022), including during the period when a disease first emerges as a pandemic threat (e.g. Ebola virus disease) and during surges and times when the incidence of a pandemic disease recedes. Given our having found that pandemic-related anxiety was related to the respondents’ estimates of the prevalence of COVID-19 in their localities, it would be helpful to study PAI scores in relation to both subjective and objective estimates of the prevalence of a pandemic in individuals’ localities.
In addition to its research applications, the PAI can be used by clinicians concerned about the impact of a pandemic on the mental health of their patients. A clinician can use the PAI to identify patients with excessive levels of COVID-related anxiety, get an idea of the impact of symptoms on their daily functioning and plans for making life changes, and then help them gain a sense of control within the pandemic context (e.g. by emphasizing the usefulness of protective measures such as vaccinations). The clinician can also encourage patients to reach out to friends and family members perceived as supportive.
Supplemental Material
sj-docx-7-hpq-10.1177_13591053221106129 – Supplemental material for The Pandemic Anxiety Inventory: A validation study
Supplemental material, sj-docx-7-hpq-10.1177_13591053221106129 for The Pandemic Anxiety Inventory: A validation study by Irvin Sam Schonfeld, Tasmyn Prytherch, Mark Cropley and Renzo Bianchi in Journal of Health Psychology
Research Data
sj-docx-8-hpq-10.1177_13591053221106129 – for The Pandemic Anxiety Inventory: A validation study
sj-docx-8-hpq-10.1177_13591053221106129 for The Pandemic Anxiety Inventory: A validation study by Irvin Sam Schonfeld, Tasmyn Prytherch, Mark Cropley and Renzo Bianchi in Journal of Health Psychology
Research Data
sj-pdf-1-hpq-10.1177_13591053221106129 – for The Pandemic Anxiety Inventory: A validation study
sj-pdf-1-hpq-10.1177_13591053221106129 for The Pandemic Anxiety Inventory: A validation study by Irvin Sam Schonfeld, Tasmyn Prytherch, Mark Cropley and Renzo Bianchi in Journal of Health Psychology
Research Data
sj-pdf-2-hpq-10.1177_13591053221106129 – for The Pandemic Anxiety Inventory: A validation study
sj-pdf-2-hpq-10.1177_13591053221106129 for The Pandemic Anxiety Inventory: A validation study by Irvin Sam Schonfeld, Tasmyn Prytherch, Mark Cropley and Renzo Bianchi in Journal of Health Psychology
Research Data
sj-pdf-3-hpq-10.1177_13591053221106129 – for The Pandemic Anxiety Inventory: A validation study
sj-pdf-3-hpq-10.1177_13591053221106129 for The Pandemic Anxiety Inventory: A validation study by Irvin Sam Schonfeld, Tasmyn Prytherch, Mark Cropley and Renzo Bianchi in Journal of Health Psychology
Research Data
sj-pdf-4-hpq-10.1177_13591053221106129 – for The Pandemic Anxiety Inventory: A validation study
sj-pdf-4-hpq-10.1177_13591053221106129 for The Pandemic Anxiety Inventory: A validation study by Irvin Sam Schonfeld, Tasmyn Prytherch, Mark Cropley and Renzo Bianchi in Journal of Health Psychology
Research Data
sj-pdf-5-hpq-10.1177_13591053221106129 – for The Pandemic Anxiety Inventory: A validation study
sj-pdf-5-hpq-10.1177_13591053221106129 for The Pandemic Anxiety Inventory: A validation study by Irvin Sam Schonfeld, Tasmyn Prytherch, Mark Cropley and Renzo Bianchi in Journal of Health Psychology
Research Data
sj-xlsx-6-hpq-10.1177_13591053221106129 – for The Pandemic Anxiety Inventory: A validation study
sj-xlsx-6-hpq-10.1177_13591053221106129 for The Pandemic Anxiety Inventory: A validation study by Irvin Sam Schonfeld, Tasmyn Prytherch, Mark Cropley and Renzo Bianchi in Journal of Health Psychology
Footnotes
Authors’ note
The paper is dedicated to the memory of Charles Steven (Charley) Kleinberg.
Data sharing statement
The current article is accompanied by the relevant raw data generated during and/or analysed during the study, including files detailing the analyses and either the complete database or other relevant raw data. These files are available in the Figshare repository and accessible as Supplemental Material via the SAGE Journals platform. Ethics approval, participant permissions, and all other relevant approvals were granted for this data sharing.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.