
Abstract
Pain disability is a primary target of treatment for chronic pain. Self-compassion shows promise as an intervention to reduce pain disability, but mechanisms linking self-compassion with less pain disability remain to be identified. This study examined two potential mechanisms, health self-efficacy and future self-identification (FSI), as parallel mediators of the relation between self-compassion and pain disability. Adults (N = 188; Mage = 40.34, SD = 11.53; 70.9% female) screened for chronic pain were recruited through online convenience sampling. Participants completed self-report measures of demographics, health status, and primary study variables. Self-compassion was positively associated with FSI and self-efficacy, but only self-efficacy was found to mediate the negative relation between self-compassion and pain disability, such that self-compassion was associated with higher self-efficacy, which was associated with less pain disability. Future experimental and longitudinal studies can establish whether the negative relation between self-compassion and pain disability is causal and mediated via health self-efficacy.
Pain disability is costly, accounting for greater pain severity, decreased emotional well-being, and greater health care use in those with chronic pain (Pitcher et al., 2019). Trait self-compassion, which represents an attitude of kindness toward oneself and one’s experiences without judgment, particularly during challenging circumstances (Neff, 2003), has been associated with better functioning and lower disability among people with chronic pain (Carvalho et al., 2020a; Davey et al., 2020). Unsurprisingly, self-compassion has garnered attention in the field of chronic pain as a resilience factor and target of intervention to decrease disability and improve functioning (Edwards et al., 2019; Purdie and Morley, 2016). However, little is known about the mechanisms by which self-compassion is associated with pain disability in chronic pain patients.
Pain elicits cognitive and affective processes that can motivate behavioral responses (Eccleston and Crombez, 1999). Issues can arise when breakdowns in self-regulation allow pain to become the sole motivator of behaviors, such as limiting movement to avoid pain or pushing beyond one’s capacities when pain is present (Hamilton et al., 2004). Adaptive self-regulation enhances the ability to function with persistent pain (Sauer et al., 2010). Self-compassion is thought to facilitate healthy functioning to due to its effects on self-regulatory processes (Terry and Leary, 2011). Self-regulation in chronic pain is influenced by multiple factors, but arguably the most often-studied such factor is health self-efficacy (Arnstein et al., 1999; Lee et al., 2015). More recently, one’s self-identify, particularly identity that incorporates a future time perspective, also has been proposed as a key element affecting adaptive self-regulation for chronic pain (Daugherty and Brase, 2010; Van Damme and Kindermans, 2015).
Health self-efficacy and future self identification as predictors of pain disability
Health self-efficacy refers to the extent to which people feel they have the skills and capacity to accomplish health goals (Sheeran et al., 2016), and is an important contributor to pain disability, above and beyond pain severity, emotional distress, and fear of movement (Asghari and Nicholas, 2001; Costa et al., 2011). Importantly, health self-efficacy alone may be insufficient to fully prevent pain disability. For example, many individuals with chronic pain may feel they have the skills to achieve health-related goals, but still may overexert themselves, resulting in greater pain disability. Similarly, even individuals with high self-efficacy will encounter challenges in achieving their health-related goals. Adaptive self-regulation can help individuals navigate obstacles that threaten self-efficacy. Thus, other elements of self-regulation can add to the effects of self-efficacy on reduced pain disability. When making choices about how to respond to pain, a person’s sense of their future self, or future self-identification (FSI), is another important factor to consider.
Imagine a person with chronic pain who must complete household chores. Avoiding the chores comes with the immediate gratification to one’s current self of avoiding pain. Similarly, completing all the chores despite high pain comes with the immediate gratification to one’s current self of completing a task. However, the consequences of both choices are greater pain disability for the future self by way of inactivity in the first example or overexertion in the second. On the other hand, a person who makes choices on behalf of their future self may choose to complete only some of the chores to preserve future functioning, satisfying goals of both the current and future self. The benefits of future self-identity on self-regulation has been discussed in the field of chronic pain (Van Damme and Kindermans, 2015). FSI assesses the extent to which the future self is viewed as positive, the ease with which one can visualize the future self, and the strength of connection to the future self (Bixter et al., 2020) and has been linked to a number of health outcomes, including drug use, exercise frequency, and overall health both in cross-sectional and experimental studies (Moss et al., 2018; Rutchick et al., 2018). For example, studies find that individuals with pain who have a discrepancy between their current and future self show higher levels of depression, anxiety, distress, and pain (Waters et al., 2004). Cross-sectional findings from studies involving adults with chronic pain bear this out. For example, stronger FSI has been negatively associated with self-blame and depression (Dany et al., 2016), and viewing the future self as positive and capable of change has been associated with less pain severity (Chang et al., 2019). In a similar vein, greater discrepancies between current and future selves predict persistence (i.e. overexertion) and avoidance behavior as measured through objective activity monitors (Huijnen et al., 2011). Together, holding a positive and easily visualized view of the future self that can achieve goals may be especially important for influencing pain disability in individuals with chronic pain, who must make decisions regarding how to manage their pain that can have long-term implications for functioning (Andrews et al., 2012).
Self-compassion as a predictor of health self-efficacy and future self-identification
Identifying resilience factors that predict adaptive self-regulation is important for the development of interventions to reduce pain disability for individuals with chronic pain. Self-compassion is both a trait and an acute emotion regulation strategy involving reappraisal of oneself in relation to suffering. Meta-analytic findings support positive associations between trait self-compassion and self-efficacy (Liao et al., 2021). Moreover, according to the self-regulatory resource model, trait self-compassion is associated with adaptive health behaviors through greater health self-efficacy (Sirois, 2015). In fact, empirical evidence suggests that trait self-compassion predicts greater health self-efficacy, which leads to more adaptive health behavior in healthy samples (Sirois and Hirsch, 2019). However, no studies have examined these associations in a chronic pain sample, nor whether health self-efficacy mediates important pain outcomes, like pain disability.
Less research has examined the relation between self-compassion and FSI in adults with chronic pain. There is reason to expect that self-compassion may facilitate FSI by allowing people with chronic pain to remain connected with their current suffering, but with a kind presence that hopes for a better future (Garland et al., 2010; Neff et al., 2005). Self-compassion has been examined in the context of attachment theory, which links cultivation of kindness toward oneself as akin to the type of kindness one would receive from an attachment figure (Joeng et al., 2017). Researchers highlight the importance of temporal focus on the future when generating self-compassion (Garland et al., 2010). For example, one cross-sectional study found that the effect of self-compassion on well-being was mediated by pleasurable anticipation about the future (Phillips, 2018). Fostering kindness to one’s current self and wishing well for one’s future self through self-compassion may bridge the current- and future-self discrepancy faced by many individuals with chronic pain.
This study aimed to determine whether health self-efficacy and FSI, two factors implicated in self-regulation, mediate the association between trait self-compassion and pain disability in adults with chronic pain. We hypothesized that the association between self-compassion and pain disability is mediated by health self-efficacy and FSI when examined as parallel mediators.
Influence of mindful decentering
This study also examined whether the parallel mediation paths between trait self-compassion and pain disability were maintained when trait mindful decentering, a concept similar to self-compassion, but one that encompasses an attitude of awareness and nonreactivity as opposed to self-kindness and nonjudgment, was included in the model. Mindful decentering, defined as nonjudgmental awareness of internal and external experiences, is a concept that overlaps with self-compassion (Fresco et al., 2007). In healthy individuals, the ability to observe, describe, and respond nonjudgmentally to internal and external experiences is positively associated with both self-efficacy (Gilbert and Waltz, 2010) and future prospection (Naisani Samani and Busseri, 2019). Moreover, 8 weeks of Mindfulness-Based Stress Reduction (MBSR) increased self-efficacy compared to usual care in adults with chronic low back pain (Turner et al., 2016) and a mindfulness intervention versus a control condition reduced negative thinking about the future in healthy adults (Rönnlund et al., 2019). Thus, a second aim of the current study was to determine whether the association between self-compassion and pain disability is mediated by health self-efficacy and FSI when controlling for mindful decentering. We hypothesized that the parallel mediation model would hold, controlling for mindful decentering because: (1) self-compassion explicitly has been described as future-oriented and (2) self-compassion is geared toward changing self-evaluations more directly than is mindfulness. Thus, despite the overlap of these concepts, we expected self-compassion versus mindful decentering would have stronger associations with the self-regulatory mechanisms examined in this study.
Method
Participants and procedure
Study procedures were approved by the Institutional Review Board at Arizona State University. Efforts were made to recruit at least 200 participants from the Amazon Mechanical Turk (MTurk) for the final analysis. MTurk is an online crowdsourcing platform and allows individuals to screen for and complete human intelligence tasks (HITs), such as surveys and experiments, for monetary compensation. The benefits of this method of sampling are the ability to study participants who might not otherwise be able to attend an in-person laboratory session. Participants were required to have at least a 90% approval rating on prior completed HITs to access the screening survey. The final sample consisted of 188 participants. This sample size provides 80% power to detect small effects of d = 0.30. These values were calculated a priori using G*Power 3 software (Faul et al., 2007).
Initially, 1000 participants were recruited via MTurk to complete a screening survey to identify individuals with chronic pain using criteria reported previously (Tompkins et al., 2016) including: (1) aged 18 years or older; (2) United States resident; (3) correctly respond to questions designed to detect inattention; (4) report persistent pain for at least the prior 6 months; (5) report past-week pain intensity on a 5-point scale (consisting of “none,” “mild,” “moderate,” “severe,” and “very severe”) of at least moderate intensity during the worst pain episode, and at least mild on average; and (6) report intensity of the last pain experienced as at least 2 using a 10 cm visual analog scale (VAS) categorized into an 11-point scale ranging from 0 “low intensity” to 10 “high intensity.” Two hundred fifty-three people met criteria for chronic pain and were invited to participate in a second survey presented as an assessment of future and past selves approximately 1 week later. Two-hundred and twenty-one participants responded completely to the second survey that included questions regarding demographics and primary study variables. Several attention checks were included in the survey that asked that participants respond in a particular way to a given question (e.g. to a question framed as “Please select 2,” participants who were paying attention should select the answer corresponding to number 2). Thirty-three participants were excluded from analyses due to failed attention checks; thus, 188 participants were included in final analyses. There were no significant differences in pain severity between adults who chose to participate in the second survey and those who did not, t(251) = 1.44, p > 0.05. Participants were paid $2.55 for completing the HIT, which took an average of 15 minutes to complete. All participants were provided informed consent at the beginning of both surveys. Consent was indicated by clicking to continue to the survey.
Measures
Chronic pain
Participants were asked questions to assess the presence and extent of chronic pain. First, they were asked whether they had experienced pain for at least 6 months (yes or no). They were then asked to rate the intensity of their average and worst pain in the past week from 0 (None) to 4 (Very Severe) and the intensity of the most recent pain experienced from 0 (No Pain) to 10 (Worst Possible Pain) using the Brief Pain Inventory (Cleeland and Ryan, 1994). They also asked how long they had been living with chronic pain in years and/or months. In the second survey, participants indicated whether they had been diagnosed with any of 27 pain and/or chronic illness conditions based on those most commonly seen in pain clinics and based on combined lists from the Centers for Disease Control and Centers for Medicare and Medicaid of what constitutes a chronic illness (Centers for Medicare & Medicaid Services, 2015; National Center for Chronic Disease Prevention and Health, 2017).
Trait self-compassion
Self-compassion was measured using the Self-Compassion Scale (SCS; Neff, 2003), which assesses the extent to which individuals treat themselves with kindness when experiencing suffering. This study used 12 items from the 26-item scale that assess “compassionate responding” including self-kindness, mindfulness, and common humanity. Answers range from 1 (Almost Never) to 5 (Almost Always). Total scores were generated by calculating a mean of the items. Higher scores indicate greater self-compassion. Internal consistency of the SCS in the current sample was α = 0.95.
The compassionate responding subscales were chosen for this study as these were thought to assess concepts associated with self-regulation. There is ongoing debate about use of the full SCS scale to measure self-compassion or whether it is more accurate to consider SCS using a two-factor structure of compassionate and uncompassionate responding (Muris and Petrocchi, 2017). A previous study examining adults with chronic pain found that individuals with greater pain acceptance also scored higher on kindness, mindfulness, and common humanity subscales (rather than the uncompassionate responding subscales) compared to adults with less pain acceptance (Costa and Pinto-Gouveia, 2011). Another study found that the relation between self-compassion and illness interference was primarily driven by talking benevolently about oneself (Terry et al., 2013). Other studies specific to chronic pain have also used the compassionate responding items (Carvalho et al., 2020b).
Future self-identification
FSI was evaluated using the Future Self-Identification Scale (FSIS; Bixter et al., 2020). The FSIS assesses the extent to which individuals can identify and visualize their future selves. The FSIS is a 6-item scale divided into three subscales measuring similarity, vividness, and positivity. Responses range from 1 (Less similar, vivid, positive) to 7 (More similar, vivid, and positive). Total scores are calculated by computing the mean of all the items across subscales. Higher scores indicate greater FSI. In the current sample, internal consistency of the scale was α = 0.93.
Health self-efficacy
The Control Beliefs Index (CBI; Sirois, 2003) is a 26-item scale that assesses four health-related beliefs in adults with chronic health issues. For this study, eight items from the mastery/self-efficacy subscale were used to measure the extent to which participants felt confident and capable of doing what is necessary to control their pain. Responses range from 1 (Strongly Disagree) to 6 (Strongly Agree). After reverse-scoring three items, total scores are calculated by computing the mean across items. Total scores range from 1 to 6 with higher scores indicate greater health self-efficacy. In the current sample, internal consistency was α = 0.85.
Pain disability
Pain disability was measured using the Pain Disability Index (PDI; Tait et al., 1990). The PDI is a 7-item instrument used to measure the impact that pain has on the ability of a person to participate in life activities. Participants are asked to rate the level of ability they experience when engaging in activities, such as family/home responsibilities, recreation, social activity, occupation, sexual behavior, and self-care. Responses range from 0 (Completely able) to 10 (Not at all able). Total scores are calculated by computing the sum of all items with scores ranging from 0 to 70. Higher scores indicate greater pain disability. In the current sample, internal consistency was α = 0.87.
Trait mindful decentering
The 7-item decentering subscale of the Toronto Mindfulness Scale (TMS; Lau et al., 2006) was used to assess the decentering facet of mindfulness. The TMS is a 13-item measure of state mindfulness. The mindful decentering subscale was selected for this study because it is a robust mechanism in the cultivation of state and trait mindfulness (Bieling et al., 2012; Davis et al., 2009). The 7-item subscale consists of items assessing the extent to which participants are disidentified and not attached to their thoughts and feelings. Items were modified to reflect trait mindful decentering, as opposed to state mindful decentering. Examples of items include, “I am receptive to observing unpleasant thoughts and feelings without interfering with them” and “I approach each experience by trying to accept it, not matter whether it is pleasant or unpleasant.” Answers range from 0 (Not at all) to 4 (Very much). Total scores were generated by calculating a mean of the items. Scores range from 0 to 4 with higher scores indicating greater mindful decentering. Internal consistency of the mindful decentering subscale in the current sample was α = 0.75.
Demographics
Demographics included age, gender, ethnicity, social class (defined as lower class, working class, middle class, upper-middle class, or upper class), and education (defined as some high school, GED or high school equivalent, some college, associate degree, bachelor degree, or master degree and above).
Data analytic plan
Analyses were conducted using IBM SPSS Statistics Version 28, beginning with computation of descriptive statistics and intercorrelations among key study variables. Mediation was tested using Mplus Version 8.1. The first parallel mediation model assessed the direct effect of self-compassion on pain disability and the indirect effects via FSI and self-efficacy using 1000 bootstrapped samples (Preacher and Hayes, 2008) without controlling for mindful decentering. The second parallel mediation model was the same as the first except for the addition of controlling for mindful decentering. Both models controlled for age, gender, race/ethnicity, education, social class, years living with pain, and average past week pain severity. Variables that were not normally distributed (i.e. years living with chronic pain) were log transformed. Significance levels for all analyses were set at p < 0.05. Standardized scores are reported.
Results
Sample characteristics
Table 1 displays the demographic characteristics of the sample. The sample comprised mostly female participants (70.9% female; 29.1% male). Participants were majority White (73.7%) followed by Asian (9.1%), Black (7%), Bi-racial (4.8%), and Hispanic (4.3%), and were 40 years old on average (Mage = 40.34, SDage = 11.53; range 20–72 years). Participants reported living with chronic pain for between 6 months to 58 years (M = 8.68 years, SD = 10.27). Values were strongly skewed, with over 75% of the sample reporting 10 or fewer years with chronic pain. Most participants self-reported experiencing musculoskeletal pain, such as back pain and sciatica pain (78.8%), followed by headache & facial pain (59.2%), rheumatologic pain (31.2%), visceral pain (20.7%), fibromyalgia pain (9.5%), and neuropathic pain (9%). Average past week of pain intensity was reported as moderate (M = 2.16, SD = 0.37).
Sample characteristics (N = 188).
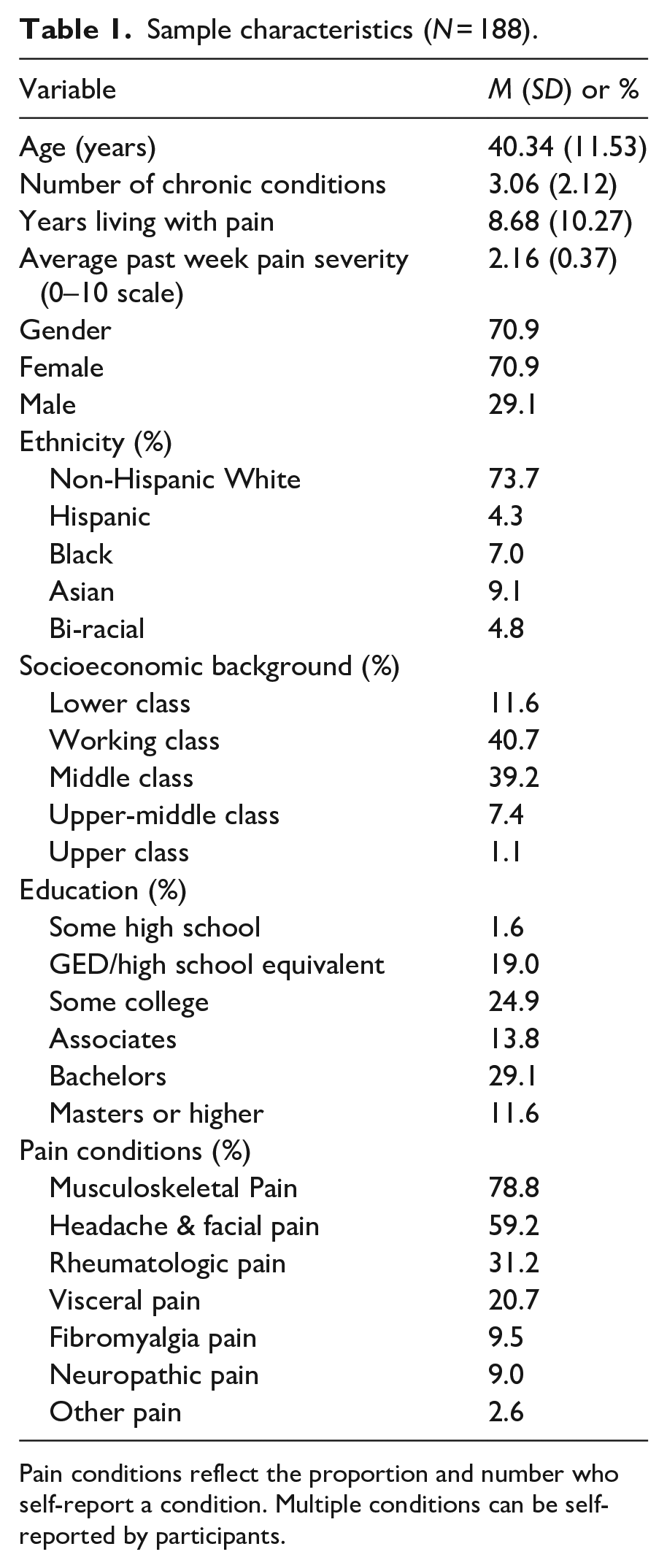
Pain conditions reflect the proportion and number who self-report a condition. Multiple conditions can be self-reported by participants.
Participant scores indicated that they were compassionate about their own experiences of suffering “some of the time” (M = 3.10, SD = 0.96), and able to decenter themselves from their emotions and feelings “some of the time” (M = 2.91, SD = 0.71). On average, they reported pain disability that was less than moderate (M = 32.84, SD = 13.31) and they mildly agreed with statements regarding their sense of their own health self-efficacy (M = 3.60, SD = 0.79). They also perceived their future selves to be slightly more similar versus dissimilar to their current self, slightly easier versus difficult to visualize, and slightly more positive versus negative compared to the current self (M = 4.37, SD = 1.33). Self-compassion was positively associated with FSI (r = 0.48, p < 0.01), health self-efficacy (r = 0.53, p < 0.01), and mindful decentering (r = 0.38, p < 0.01) and negatively associated with pain disability (r = −0.24, p < 0.01). Mindful decentering was not significantly associated with pain disability (r = 0.09, ns). FSI was positively associated with health self-efficacy (r = 0.48, p < 0.01) and negatively associated with pain disability (r = −0.18, p < 0.01). Health self-efficacy was also negatively associated with pain disability (r = −0.38, p < 0.01). Predictably, pain disability was positively associated with self-reported pain severity (r = 0.19, p < 0.01) and age was positively associated with years living with chronic pain (r = 0.35, p < 0.01). There were no significant differences in levels of self-compassion, decentering, self-efficacy, FSI, or pain disability based on gender, ethnicity, education, social class, pain severity, and years living with pain. Models were run with and without demographic variables and findings were unchanged. Reported results include demographic variables.
Self-compassion – Pain disability relation: Test of parallel mediation
The two parallel mediations, the first of which did not control for mindful decentering and the second of which controlled for mindful decentering, showed similar findings. Results of the first parallel mediation model are presented in Supplemental Material. Results for the second parallel mediation model, controlling for mindful decentering, are presented here and in Figure 1. Inconsistent with hypotheses, there was no direct relation between self-compassion and pain disability (
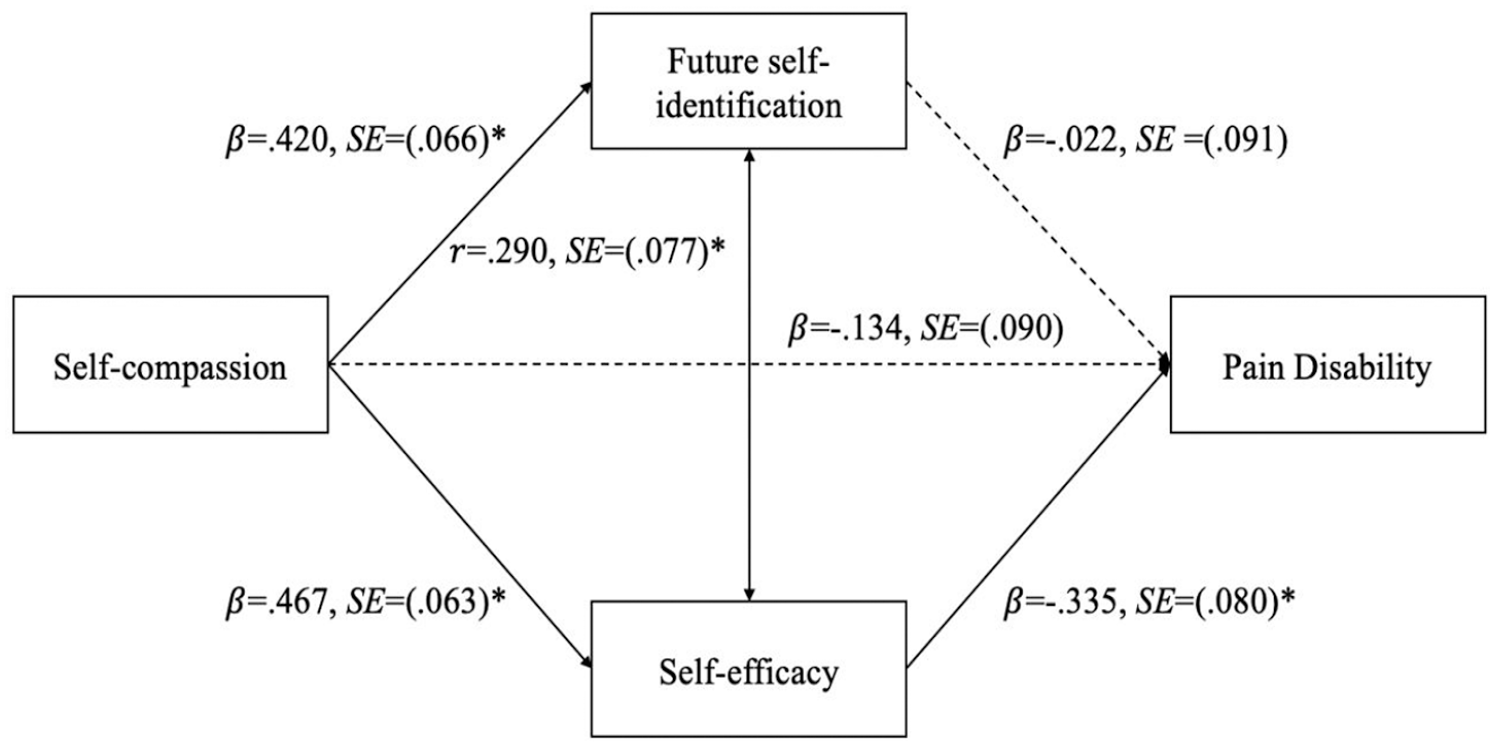
p < .001; Model of self-compassion as a predictor of pain disability, mediated by self-efficacy. Model controlling for mindful decentering, age, sex, ethnicity, social class, pain severity, and length of time living with pain. Solid lines denote significant paths.
Discussion
The current study examined the direct and indirect relations linking self-compassion and pain disability in a sample of adults with chronic pain. Self-compassion did not have a direct relation with pain disability but showed an indirect relation through health self-efficacy. Self-compassion was also strongly related to FSI, but FSI did not predict pain disability. These findings suggest that among diverse individuals with chronic pain, higher levels of self-compassion are associated with less pain-related disability via enhanced health self-efficacy.
There was no direct relation between self-compassion and pain disability. Although self-compassion was negatively correlated with pain disability in univariate analyses, the inclusion of self-regulatory mechanisms (specifically health self-efficacy), fully explained this relation. This finding is inconsistent with a previous cross-sectional study which found that self-compassion predicted physical and psychosocial functioning, controlling for similar factors including pain duration, average pain, age, and gender (Edwards et al., 2019). However, Edwards et al. (2019) did not include other factors associated with self-regulation. The findings from the present study contribute to our understanding of how self-compassion may affect pain disability.
Self-compassion was negatively associated with pain disability through health self-efficacy. This finding is consistent with past literature. For example, studies show that trait self-compassion is positively associated with self-efficacy (Liao et al., 2021), and that the relation between self-compassion and adaptive health behaviors is mediated by higher self-efficacy according to the self-regulation resource model (Sirois, 2015). This study expands upon prior work to demonstrate that this relation holds in a chronic pain sample. According to these findings, trait self-compassion may be an important resilience factor predicting self-efficacy and less pain disability in people with chronic pain.
Self-compassion was positively associated with FSI, but FSI was not associated with pain disability. This is the first study to examine relations between these concepts. The relation between self-compassion and FSI coincides with theoretical models of self-compassion and attachment, which propose that being self-compassionate involves a connection to a future, wiser self (Garland et al., 2010). The fact that this relation was found in adults with chronic pain is noteworthy. For instance, chronic pain has been shown to narrow one’s attention to present-focused pain and/or catastrophic thoughts about one’s future (Garland et al., 2013). Self-compassion may represent an avenue to increase acceptance of current pain and reduce catastrophic thinking about the future. Importantly, FSI was not associated with pain disability. This is inconsistent with literature, which finds that future prospection and FSI is associated with adaptive health outcomes (Daugherty and Brase, 2010). One reason for the weaker association between FSI and pain disability could be due to the correlation between FSI and health self-efficacy. However, this correlation was modest and not suggestive of multicollinearity. It is possible that FSI may facilitate health self-efficacy, such as through serial mediation wherein self-compassion facilitates enhanced FSI, which facilitates health self-efficacy, which facilitates less pain disability. One meta-analysis found that the effects of FSI on health outcomes is partially explained by self-regulatory mechanisms, like self-efficacy (Baird et al., 2021), suggesting that the two may work in sequence. This cross-sectional study already limits the conclusions that can be drawn from parallel mediation, but future work with a larger sample size and temporal precedence could examine serial mediation.
These findings have important clinical implications in the treatment of chronic pain. Research suggests that self-compassion is useful for individuals with chronic pain due to its proposed effects on reducing negative self-evaluations, improving regulation of negative emotions, and fostering positive affect and affiliative drives (Purdie and Morley, 2016). The present findings offer preliminary evidence that self-compassion may also impact pain disability in chronic pain patients. There is research exploring the effects of self-compassion interventions for chronic pain. For example, Compassion Focused Therapy (CFT) increased self-compassion and reduced pain disability in a sample of adults with chronic pain who engage in over-activity (Malpus et al., 2023). Another randomized controlled trial found that Mindful Self-Compassion training (MSC) reduced pain interference to a greater extent than Cognitive Behavioral Therapy (CBT) in chronic pain patients (Torrijos-Zarcero et al., 2021). Although these efforts are promising, more research is needed, and the evidence for self-compassion interventions is limited.
An alternative to interventions focused on self-compassion is identifying ways that current evidence-based approaches might (1) increase emphasis on intervention components that include self-compassion in some capacity, or (2) introduce self-compassion explicitly to enhance effects on pain disability. Several evidence-based treatments include self-compassion in some capacity. For example, Emotional Awareness and Expression Therapy (EAET) aims to address emotional factors (e.g. trauma) that underlie poor pain processing. EAET includes self-compassion training to identify emotional defenses and develop more adaptive responses (Lumley and Schubiner, 2019). Enhancing the self-compassion elements in EAET may instill greater self-efficacy to handle emotional distress, which may indirectly influence pain disability. MBSR aims to influence pain functioning by helping individuals develop a nonjudgmental attitude around their internal and external experiences (Day et al., 2014). MBSR courses often include self-compassion training at the end of treatment (Kabat-Zinn, 1990). A greater emphasis on self-compassion throughout MBSR training may increase self-efficacy around approaching sensations with a nonjudgmental and kind attitude, which may reduce pain disability.
Other evidence-based therapies do not teach self-compassion explicitly. CBT aims to adapt individual’s cognitions and appraisals about their pain to increase functioning (Williams et al., 2020). Pain catastrophizing is a common maladaptive cognition targeted in CBT and is a predictor of greater pain disability (Severeijns et al., 2001). Self-compassion may be explicitly added to CBT protocols to help individuals reappraise themselves and their future pain with compassion, which could enhance self-efficacy and reduce pain disability.
Strengths and limitations
Although this study highlights important relations between self-compassion and pain disability, the cross-sectional design prevents describing these associations as causal. However, cross-sectional designs are useful to identify mechanisms that can be explored in longitudinal and experimental work. Importantly, research finds that effects found in cross-sectional mediation can be weaker when examined longitudinally (Maxwell et al., 2011). In the current study, the ordering of study variables was theoretically driven. Nevertheless, the ordering of these constructs is limited in this cross-sectional design and should be further examined experimentally. The small size of the mediated relation might suggest limited clinical relevance, but small effects can have a large impact given the prevalence and duration of chronic pain and pain disability. Future work should explore these relations among adults in chronic pain clinics. Participants were recruited using MTurk whose workers are not representative of the population but tend to be more diverse demographically and clinically than samples used clinical studies (e.g. students and community samples; Chandler and Shapiro, 2016). Additionally, intervention research could investigate how self-compassion inductions alter health self-efficacy, in turn yielding benefits for pain outcomes, including pain disability.
To conclude, the present study found that trait self-compassion was indirectly associated with pain disability via health self-efficacy in a sample of adults with chronic pain. Findings expand upon prior work demonstrating the effects of self-compassion on health outcomes to a chronic pain sample. Future experimental work is needed to determine causality. The present study identified self-efficacy as a possible mechanism explaining the link between self-compassion and pain disability. Further, the study identifies how evidence-based approaches might include self-compassion or strengthen self-compassion elements to reduce pain disability.
Research Data
sj-csv-6-hpq-10.1177_13591053231167275 – Supplemental material for Self-compassion and pain disability in adults with chronic pain: The mediating role of future self-identification and self-efficacy
sj-csv-6-hpq-10.1177_13591053231167275 for Self-compassion and pain disability in adults with chronic pain: The mediating role of future self-identification and self-efficacy by Erin G Mistretta, Mary C Davis, Eva M Bartsch and Meryl S Olah in Journal of Health Psychology
Research Data
sj-docx-1-hpq-10.1177_13591053231167275 – Supplemental material for Self-compassion and pain disability in adults with chronic pain: The mediating role of future self-identification and self-efficacy
sj-docx-1-hpq-10.1177_13591053231167275 for Self-compassion and pain disability in adults with chronic pain: The mediating role of future self-identification and self-efficacy by Erin G Mistretta, Mary C Davis, Eva M Bartsch and Meryl S Olah in Journal of Health Psychology
Research Data
sj-docx-4-hpq-10.1177_13591053231167275 – Supplemental material for Self-compassion and pain disability in adults with chronic pain: The mediating role of future self-identification and self-efficacy
sj-docx-4-hpq-10.1177_13591053231167275 for Self-compassion and pain disability in adults with chronic pain: The mediating role of future self-identification and self-efficacy by Erin G Mistretta, Mary C Davis, Eva M Bartsch and Meryl S Olah in Journal of Health Psychology
Research Data
sj-docx-5-hpq-10.1177_13591053231167275 – Supplemental material for Self-compassion and pain disability in adults with chronic pain: The mediating role of future self-identification and self-efficacy
sj-docx-5-hpq-10.1177_13591053231167275 for Self-compassion and pain disability in adults with chronic pain: The mediating role of future self-identification and self-efficacy by Erin G Mistretta, Mary C Davis, Eva M Bartsch and Meryl S Olah in Journal of Health Psychology
Research Data
sj-docx-7-hpq-10.1177_13591053231167275 – Supplemental material for Self-compassion and pain disability in adults with chronic pain: The mediating role of future self-identification and self-efficacy
sj-docx-7-hpq-10.1177_13591053231167275 for Self-compassion and pain disability in adults with chronic pain: The mediating role of future self-identification and self-efficacy by Erin G Mistretta, Mary C Davis, Eva M Bartsch and Meryl S Olah in Journal of Health Psychology
Supplemental Material
sj-docx-8-hpq-10.1177_13591053231167275 – Supplemental material for Self-compassion and pain disability in adults with chronic pain: The mediating role of future self-identification and self-efficacy
Supplemental material, sj-docx-8-hpq-10.1177_13591053231167275 for Self-compassion and pain disability in adults with chronic pain: The mediating role of future self-identification and self-efficacy by Erin G Mistretta, Mary C Davis, Eva M Bartsch and Meryl S Olah in Journal of Health Psychology
Research Data
sj-pdf-2-hpq-10.1177_13591053231167275 – Supplemental material for Self-compassion and pain disability in adults with chronic pain: The mediating role of future self-identification and self-efficacy
sj-pdf-2-hpq-10.1177_13591053231167275 for Self-compassion and pain disability in adults with chronic pain: The mediating role of future self-identification and self-efficacy by Erin G Mistretta, Mary C Davis, Eva M Bartsch and Meryl S Olah in Journal of Health Psychology
Research Data
sj-pdf-3-hpq-10.1177_13591053231167275 – Supplemental material for Self-compassion and pain disability in adults with chronic pain: The mediating role of future self-identification and self-efficacy
sj-pdf-3-hpq-10.1177_13591053231167275 for Self-compassion and pain disability in adults with chronic pain: The mediating role of future self-identification and self-efficacy by Erin G Mistretta, Mary C Davis, Eva M Bartsch and Meryl S Olah in Journal of Health Psychology
Footnotes
Author contribution
The first and second authors designed the study. The first author executed the study and analyzed the data. All authors contributed to the writing and editing of the final manuscript and approved the final version for submission.
Data sharing statement
The current article is accompanied by the relevant raw data generated during and/or analysed during the study, including files detailing the analyses and either the complete database or other relevant raw data. These files are available in the Figshare repository and accessible as Supplemental Material via the Sage Journals platform. Ethics approval, participant permissions, and all other relevant approvals were granted for this data sharing.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
This study has been approved by the Institutional Review Board at Arizona State University (STUDY00011310) and therefore performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Pre-registration
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.