
Abstract
Previous studies have indicated that cancer patients may have a lower level of subjective well-being (SWB); nevertheless, the underlying factors for this phenomenon remain insufficiently investigated. Based on the characteristics of Chinese breast cancer patients and the unique culture, this study explored the independent contributions of death anxiety, self-esteem, and social support to SWB from the protective and risk perspectives. A cross-sectional survey recruited 514 females with breast cancer and collected participants’ demographic and the above variables. The results found that death anxiety independently predicted SWB in a negative direction (β = −0.36, p < 0.001). In addition, self-esteem (β = 0.38, p < 0.001) and social support (β = 0.14, p < 0.001) also had the unique positive effects on SWB. These findings offer new insights into strengthening breast cancer patients’ SWB, for instance, using relevant interventions to reduce death anxiety and improve self-esteem and social support.
Introduction
According to the Global Cancer Statistics Report 2020, the incidence and mortality of breast cancer were 11.7% and 6.9% respectively, and breast cancer was the fifth leading cause of cancer mortality worldwide (Sung et al., 2021). In China, the incidence and mortality rates of breast cancer were increasing (Ding et al., 2022; Zhang et al., 2021). In particular, age-specific incidence rates showed the greatest increase in younger age groups (Lei et al., 2021). Additionally, breast cancer patients reported higher levels of death anxiety than other types of cancer (Soleimani et al., 2020). Moreover, it is worth noting that discussing death is a taboo in traditional Chinese culture (Wang et al., 2023; Zheng et al., 2015), and Chinese people generally refrain from related topics even with great fear, which may be great challenges for breast cancer patients. Therefore, it is necessary and reasonable to spotlight breast cancer patients in China in relation to their characteristics and the culture.
Some empirical studies have advocated that the mental health of breast cancer patients should receive more attention (Abrahams et al., 2018; Carreira et al., 2018; Zainal et al., 2013). The current study heeds such a call by examining subjective well-being (SWB) that refers to how people evaluate and experience their lives in positive ways (Diener, 1984). To date, existing research and reviews have shown that SWB is associated with health behaviors, immune and cardiovascular systems (Cohen et al., 2003; Diener and Chan, 2011; Diener et al., 2017), underscoring the importance role of SWB in health. Nevertheless, some evidence suggested that cancer patients were vulnerable to low levels of SWB (Rudaz et al., 2019). For example, some patients experienced a decline in mental health following diagnosis, and they reported high levels of psychological distress, which may have additional implications for functioning and well-being (Badana et al., 2019; Bloom et al., 2012; Park et al., 2020; Ruini et al., 2013; Schreiber and Brockopp, 2012), such as negative effects on physical possibilities, social relationships, independent living skills, and life satisfaction. Considering the link between SWB and patients’ health, it is crucial to address the decline in SWB among breast cancer patients.
In the present study, we concentrated on Chinese breast cancer patients and investigated the influencing factors of their SWB. As mentioned previously, given the potential threat of high mortality in these patients, we examined whether death anxiety was negatively associated with SWB. Moreover, studies have indicated the central roles of self-esteem and social support in human well-being (Baumeister et al., 2003; Siedlecki et al., 2014), which were widely acknowledged as important resources for managing and adapting to stressful situations (Di Paula and Campbell, 2002; Taylor, 2011). Therefore, we also explored the effects of self-esteem and social support on SWB. More importantly, the study tested the unique contributions of death anxiety, self-esteem, and social support to SWB from the protective and risk viewpoints, which provided a more comprehensive understanding of low levels of SWB among Chinese breast cancer patients.
Death anxiety and SWB
Death anxiety is one of the most common psychological distresses (Karampour et al., 2018) and is defined as a negative emotion of anxiety and fear caused by the desire to live and the inevitability of death (Neimeyer, 1994). It is well known that death is inevitable and can occur at any time from many potential causes. Taking into account that breast cancer patients may confront the real threat of death, they probably have a tendency to experience death anxiety (Bibi and Khalid, 2020; Karampour et al., 2018). Beck’s cognitive model has indicated that anxiety may activate and induce a selective processing that makes one exposed to the risk of threat, danger, and helplessness, and it tends to lead to negative “automatic” thoughts, which highlights that the persistence of subjective anxious feelings may be associated with negative cognitions about the self, world, and future (Clark and Beck, 2010). Similarly, in view of the limited lifespan, patients suffering from death anxiety may have more negative feelings and cognitions (e.g. it is all over for me) in this situation, which was related to the low assessment of their lives. This means that breast cancer patients who perceived death anxiety may tend to experience lower levels of SWB.
Previous studies have established a link between death anxiety and life satisfaction among elderly individuals (Roshani, 2012; Taghiabadi et al., 2017) and young Catholics and Protestants (Cohen et al., 2005), however, there is still a gap in our understanding of the above relationship among breast cancer patients, particularly in the Chinese context. Considering the rising mortality rates and the cultural taboo of discussing death (Ding et al., 2022; Wang et al., 2023; Zhang et al., 2021; Zheng et al., 2015), we expect the relationship between death anxiety and SWB to be amplified among Chinese breast cancer patients.
Self-esteem and SWB
Self-esteem refers to the global positive appraisal of one’s self-value or worth (Rosenberg, 1965), which has been shown to be a strong predictor of SWB across various populations, including elderly individuals, adolescents, high school and college students, and cancer patients in Germany (Chen et al., 2021; Duy and Yıldız, 2019; Kong et al., 2013; Pinquart and Fröhlich, 2009; Tian, 2016). However, it remains unclear whether these findings can be generalized to Chinese breast cancer patients. Stress and coping models (Lazarus, 1999; Moos and Schaefer, 1993) have pointed out that sufficient resources are supported as tools to cope with stressful encounters, which subsequently have the effect on well-being. According to the above theory, when individuals were suddenly diagnosed with cancer, they may realize that there is no opportunity to develop self-values across the life and work domains, which may be associated with poor self-esteem (Taylor, 1983). Furthermore, when patients with declined self-esteem failed to deal with the stress of cancer due to inadequate personal resources, they may experience low levels of SWB. Therefore, we speculate that self-esteem also positively predicts SWB among Chinese breast cancer patients.
Social support and SWB
Social support is defined that individuals perceive the spiritual and material help from others (Wills, 1991). Similarly, social support is recognized as a beneficial predictor of SWB in adolescents, the elderly, and breast cancer patients from the United States (Jiang et al., 2020; Kong et al., 2021; McDonough et al., 2014), but less is known about Chinese breast cancer patients. In light of stress and coping models (Lazarus, 1999; Moos and Schaefer, 1993), social support performs as a social resource that helps release external pressures and then contributes to one’s well-being. However, when breast cancer patients perceived lower social support from others, they may have difficulty in dealing with stresses, such as the threat of disease, as well as emotional and cognitive issues, thereby relating to lower levels of SWB. Therefore, we hypothesize that social support is also a positive predictor of SWB among Chinese breast cancer patients.
The present study
Based on the existing studies (Duy and Yıldız, 2019; Kong et al., 2021; Rudaz et al., 2019; Taghiabadi et al., 2017), the present study has been extended as follows. First, it is crucial to recognize the uniqueness of breast cancer patients in China, who are facing increasing incidence and mortality rates and influenced by traditional cultural taboos about death (Ding et al., 2022; Wang et al., 2023; Zhang et al., 2021; Zheng et al., 2015). Such factors make it essential to shed more light on this population. Second, given that it has been shown that cancer patients experienced low levels of SWB (Rudaz et al., 2019), considering the significance of SWB for patients, this study systematically explored the potential factors related to SWB. Third, the study concentrated on breast cancer patients in China and examined the unique contributions of death anxiety, self-esteem, and social support to SWB, which have never been simultaneously considered together. It is necessary and important because the study tested both protective and risk predictors of SWB, which offered new insights into improving the SWB levels of breast cancer patients.
Taken together, our study investigated the unique contributions of death anxiety, self-esteem, and social support to SWB among Chinese breast cancer patients. Informed by the literature and theories, three hypotheses were proposed: (1) Death anxiety independently correlated with poor SWB among Chinese breast cancer patients; (2) Self-esteem had a uniquely positive effect on SWB among breast cancer patients in China; and (3) Social support was independently related to high levels of SWB among Chinese breast cancer patients.
Methods
Participants and procedure
A sample of 531 females diagnosed with breast cancer was recruited from a public 3A hospital (a first-class hospital in a medical system with high-quality care and safety as well as high levels of technology) in an urban area (Beijing, China). The inclusion criteria were as follows: (1) diagnosed with breast cancer by clinical pathology, and (2) aged between 18 and 70 years and able to understand the content of questionnaires. Patients were excluded if they also had severe psychiatric or neurological disorders or other cancers. Finally, a sample of 514 females with breast cancer (Mage = 46.69, SD = 9.94, range from 24 to 70 years) was included. In addition, in order to execute a correlation analysis, it is reported that at least 314 participants are needed to test a medium-sized effect (r = 0.20, α = 0.05, 1−β = 0.95) using G*Power software (Faul et al., 2007). Thus, the current study had enough power to detect the assumed effect size.
The present study was a cross-sectional design. The data was collected in March 2021 before patients took the surgery in the hospital. All processes were carried out by the medical staff. First, patients were invited to participate in the survey and informed about the purpose of the study to know their mental health status and the confidentiality of the survey. Next, they volunteered to take part in the current study and signed the informed consent. Afterward, patients were provided with written and verbal instructions explaining the procedure and the items on the questionnaire. All patients completed the paper questionnaire, which involved the measurements of demographic data, death anxiety, self-esteem, social support, and SWB. The patients received gifts for participating in the present study.
Measures
Death anxiety
The Templer Death Anxiety Scale (T-DAS) contains 15 items rated on a 5-point Likert scale (1 = strongly disagree; 5 = strongly agree) (Templer, 1970). A sample item is “I am very much afraid to die.” It has been widely applied to cancer patients with good reliability and validity (Hong et al., 2022; Soleimani et al., 2016). Higher scores represent higher levels of death anxiety. In the current study, Cronbach’s alpha coefficient of the T-DAS was 0.84.
Self-esteem
The Rosenberg Self-esteem Scale (RSES) contains 10 items rated on a 4-point Likert scale (1 = strongly disagree; 4 = strongly agree) (Rosenberg, 1965). A sample item is as follows “On the whole, I am satisfied with myself.” The scale has displayed great reliability and validity in cancer patients (Aprilianto et al., 2021; Cobo-Cuenca et al., 2019). Higher scores indicate higher levels of self-esteem. In addition, Cronbach’s alpha for the RSES was 0.84 in this study.
Social support
The Medical Outcomes Study Social Support Survey (MOSSS) involved 20 items to assess four resources of perceived social support, including emotional/informational, tangible, affectionate, and positive social interaction (Sherbourne and Stewart, 1991), which has been widely used in patients with breast cancer (Leung et al., 2014; Zamanian et al., 2021). It was evaluated on a 5-point Likert scale (1 = very slightly or not at all; 5 = extremely). A sample item is “Someone to love and make you feel wanted.” Higher scores represent higher levels of social support. In this study, Cronbach’s alpha for the MOSSS was 0.96.
SWB
The Satisfaction with Life Scale was adopted to assess the cognitive component of SWB (Diener et al., 1985). There are five items answered on a 7-point Likert scale (1 = strongly disagree; 7 = strongly agree). A sample item is as follows “I am satisfied with my life.” The scale was found to have good reliability and validity in cancer patients (Deimling et al., 2019; Lorenzo-Seva et al., 2019). Additionally, the affective component of SWB was appraised by the Positive and Negative Affect Schedule (Watson et al., 1988), which has shown satisfactory reliability and validity in cancer patients (Cole et al., 2008; Salsman et al., 2019). The scale contains 10 items for positive affect and 10 items for negative affect, and the items were rated on a 5-point Likert scale (1 = very slightly or not at all; 5 = extremely). Following the prompt “I felt. . .,” participants described how strongly they felt “excited,” “interested,” “upset,” and “nervous” over the past week. SWB was calculated by subtracting negative affect from the sum of life satisfaction and positive affect (Haslam et al., 2009; Martela and Ryan, 2016; Sheldon et al., 2019, 2021; Zhang et al., 2023), and the Cronbach’s alpha was 0.90. In addition, higher scores indicate higher levels of SWB.
Control variables
In the present study, some sociodemographic variables (e.g. age, marital status, education level, and subjective socioeconomic status) are related to SWB (Diener et al., 2000; Horley and Lavery, 1995; Tan et al., 2020; Witter et al., 1984); thus, we regarded them as covariates in the following analyses. In addition, we have dummy coded the categorical variables (e.g. marital status and education level).
Statistical analysis
In the current study, we utilized SPSS 22.0 to analyze the data. First, given that the rate of missing data in our dataset was less than 10%, we used mean imputation to address the missing data (Little and Rubin, 2002). Second, descriptive and correlation analyses among the major variables were examined. Third, hierarchical regression analysis was conducted. Model 1 was the baseline model, in which we entered all control variables (e.g. age, marital status, education level, and subjective socioeconomic status) as the predictors and SWB as the outcome. Based on Model 1, we also added death anxiety, self-esteem, and social support as the predictors in Model 2, which tested the unique contribution of one while controlling for the roles of the other two.
Results
Descriptive statistics
Table 1 displayed the means, standard deviations, and correlations among major variables. Specifically, death anxiety was negatively associated with self-esteem, social support, and SWB (ps <0.05). In addition, self-esteem and social support were positively correlated with SWB (ps <0.05). Besides, more details about sociodemographic and clinical characteristics were provided in Supplemental Table 1.
Descriptive statistics and correlations among major variables.
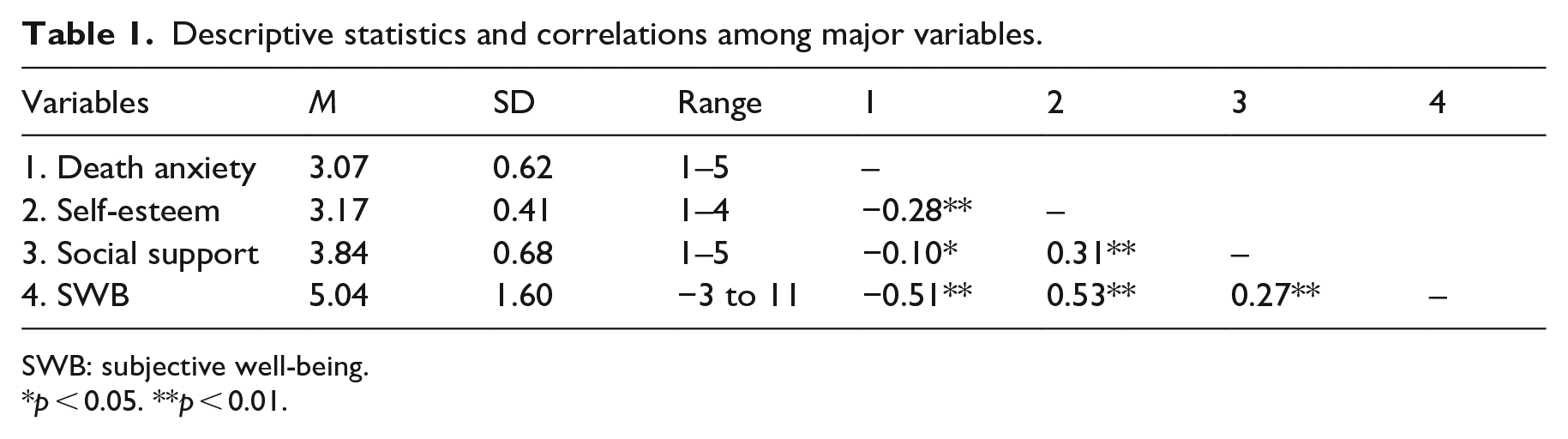
SWB: subjective well-being.
p < 0.05. **p < 0.01.
Regression analysis
As displayed in Table 2, Model 1 accounted for 10% of the variance in SWB and indicated that the widowed group (compared with the married/remarried group) reported low SWB. With increasing age and subjective socioeconomic status, participants reported better SWB. Model 2 found that death anxiety, self-esteem, and social support were significantly and uniquely related to SWB, accounting for 49% of the variance in SWB. Specifically, death anxiety (β = −0.36, p < 0.001) was negatively associated with SWB, whereas self-esteem (β = 0.38, p < 0.001) and social support (β = 0.14, p < 0.001) were positively related to SWB. 1 Taken together, the results supported our hypotheses.
Hierarchical regression results for subjective well-being.
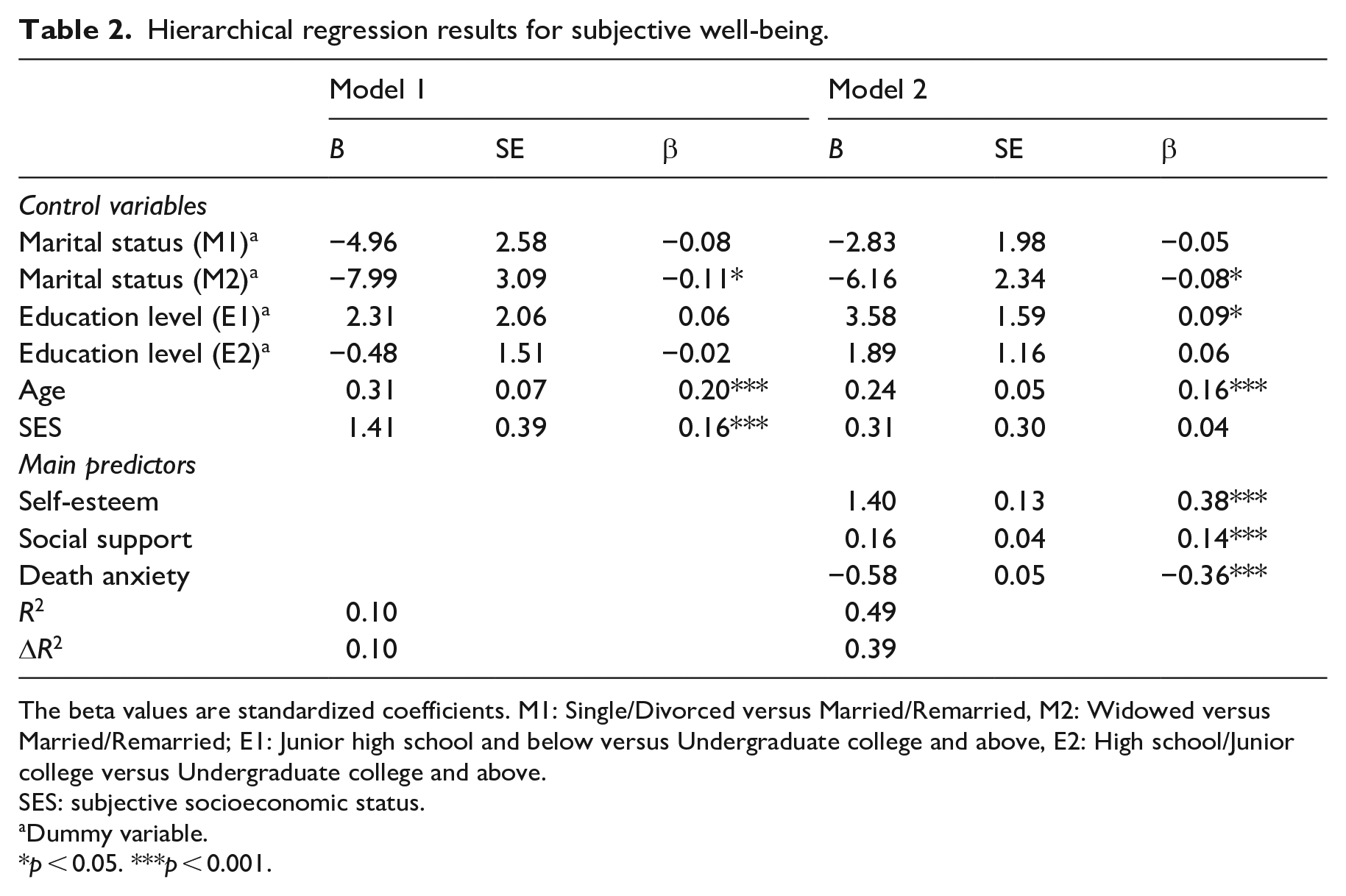
The beta values are standardized coefficients. M1: Single/Divorced versus Married/Remarried, M2: Widowed versus Married/Remarried; E1: Junior high school and below versus Undergraduate college and above, E2: High school/Junior college versus Undergraduate college and above.
SES: subjective socioeconomic status.
Dummy variable.
p < 0.05. ***p < 0.001.
Discussion
Given the unique characteristics of breast cancer patients in China, our study primarily focused on this population and inspected the unique contributions of death anxiety, self-esteem, and social support to SWB from both protective and risk viewpoints. As expected, the findings showed that all the above variables independently predicted breast cancer patients’ SWB, which was consistent with Beck’s cognitive model (Clark and Beck, 2010) as well as stress and coping models (Lazarus, 1999; Moos and Schaefer, 1993).
First, death anxiety uniquely predicted SWB in a negative direction among Chinese breast cancer patients. It represents mortality-related changes in SWB that were not derived from the debasement of one’s own value when patients felt a sense of impending death. Furthermore, these changes were not generated without the company and support of others because the average score of social support was at a high level. Actually, death was often regarded as a “taboo” topic and rarely talked about in China (Zheng et al., 2015). To some extent, cancer transmits “death messages”; for breast cancer patients, they may not know whether and how to discuss death and express their own thoughts with others. Therefore, a possible explanation for the source of death anxiety is that it not only comes from the fear of death itself, but also from the complex feelings of being suppressed from expressing as well as not knowing how to discuss it. Subsequently, patients with death anxiety may narrow their perspective and tend to generate some negative emotions and cognitions (Clark and Beck, 2010), which may relate to low levels of SWB. In addition, this is partly in accordance with previous findings in noncancer populations (Cohen et al., 2005; Roshani, 2012; Taghiabadi et al., 2017), and the effect size is larger than the above studies (ranging from −0.20 to −0.26), suggesting that Chinese cultural taboos on death may pose some challenges for these patients in dealing with death anxiety and further linking to poor SWB. In general, death anxiety uniquely predicted Chinese breast cancer patients’ SWB.
In addition, we found that there was an independent positive association between self-esteem and SWB among Chinese breast cancer patients. It has been posited that self-esteem provides individuals with a type of “energy” that supports them when struggling with stressful events (Cast and Burke, 2002). According to stress and coping models (Lazarus, 1999; Moos and Schaefer, 1993), self-esteem serves as a personal resource that helps patients deal with the distress caused by cancer when they are fighting with such event. That is, the higher self-evaluations may be linked with greater personal resources, which could be better used to confront with distress; therefore, patients may adopt some positive coping strategies and experience higher levels of SWB. Whereas low levels of self-esteem showed an opposite pattern of the relation, a possible reason is that patients may disparage their value due to the label of patients, such as “I cannot do anything because I am a patient.” These results are consistent with the research showing that self-esteem is positively correlated with SWB in other samples (Chen et al., 2021; Duy and Yıldız, 2019; Pinquart and Fröhlich, 2009; Tian, 2016), and the effect size is larger than that reported in these studies (ranging from 0.19 to 0.29), highlighting the significant role of self-esteem in Chinese breast cancer patients. Therefore, Chinese breast cancer patients with higher levels of self-esteem reported greater SWB.
Importantly, our evidence clarified that social support had a unique effect on SWB among Chinese breast cancer patients. As mentioned above, social support is considered as the important social resource by which patients can receive material and psychological support to address their illness (Hobfoll, 2001). That is, when patients perceived more help and care from others, they may accumulate more social resources to cope with the stress caused by cancer, which further had a positive effect on their SWB. This is consistent with stress and coping models (Lazarus, 1999; Moos and Schaefer, 1993), which explains that social support may be a positive factor for patients’ SWB. In addition, our findings are in accordance with existing work (Jiang et al., 2020; Kong et al., 2021; McDonough et al., 2014), and the effect size is smaller than that observed in previous studies (ranging from 0.17 to 0.39). This discrepancy may be attributed to the cultural emphasis on obligations toward family members in Chinese society (You and Lu, 2014). However, breast cancer patients may encounter challenges in reciprocating social support to their families, which may lead to additional pressure and have a small effect. Taken together, our study provided empirical evidence that social support independently predicted SWB among Chinese breast cancer patients.
There are several limitations to our study. First, although a cross-sectional design grounded in theories and empirical research is valuable (Shrout, 2011), this method still has limitations. Longitudinal or experimental designs should be used to verify our findings and explore the causal effect in the future. Second, although the measurements had satisfactory psychometric indicators, our findings were based on self-report measures which may induce recall bias and social desirability, thus future studies should employ a multi-informant method (e.g. self-report and caregiver report) to replicate and expand our results. Third, the findings were drawn from a sample of Chinese breast cancer patients in urban areas, with higher incidence and mortality rates than in rural areas (Lei et al., 2021). Besides, breast cancer incidence is increasing in Western countries, but the mortality rate is decreasing (Ding et al., 2022; Leong et al., 2010). Therefore, considering these variations, future studies should be conducted in patients from different areas and countries to test our findings.
Despite these limitations, the insights gained from this study have clinical implications. Overall, according to our findings, self-esteem and social support have positive effects on SWB, and the negative effect of death anxiety cannot be ignored. Therefore, we should improve patients’ SWB from various perspectives. First, it is necessary to focus on strategies to reduce patients’ death anxiety. As reported, activities that evoke a sense of meaning are beneficial in reducing death anxiety (Grossman et al., 2018). Therefore, patients with death anxiety are advised to participate in the above programs. Second, previous studies have found that some interventions contribute greatly to self-esteem (Niveau et al., 2021). For example, the cognitive aspects of self-perception are achieved by modifying dysfunctional self-schemata (e.g. cognitive-behavioral therapies) or altering the processing of self-perceptions in memory (e.g. reminiscence-based interventions). Therefore, it is recommended for patients to engage in self-esteem interventions; furthermore, their SWB may be potentially enhanced. Third, given the positive effect of social support on patients’ SWB, interventions such as those aimed at increasing network size and building social skills can be implemented to build and maintain social support (Hogan et al., 2002). Fourth, it is interesting whether an integrative approach of interventions targeting death anxiety, self-esteem, and social support would confer benefits to patients’ SWB.
Conclusion
This is the first study to focus on Chinese breast cancer patients and explore the unique contributions of death anxiety, self-esteem, and social support to SWB. Specifically, death anxiety has an independent and negative effect on patients’ SWB. In addition, self-esteem and social support have independent positive effects on SWB. The findings provide new insights into improving SWB for breast cancer patients, such as decreasing death anxiety as well as promoting self-esteem and social support.
Supplemental Material
sj-docx-1-hpq-10.1177_13591053231195391 – Supplemental material for Subjective well-being among Chinese breast cancer patients: The unique contributions of death anxiety, self-esteem, and social support
Supplemental material, sj-docx-1-hpq-10.1177_13591053231195391 for Subjective well-being among Chinese breast cancer patients: The unique contributions of death anxiety, self-esteem, and social support by Kairong Yang, Yinpeng Ren, Wenya Peng, Xiangyu Wang, Xiaopeng Du, Jing Wang and Jiang Jiang in Journal of Health Psychology
Supplemental Material
sj-docx-2-hpq-10.1177_13591053231195391 – Supplemental material for Subjective well-being among Chinese breast cancer patients: The unique contributions of death anxiety, self-esteem, and social support
Supplemental material, sj-docx-2-hpq-10.1177_13591053231195391 for Subjective well-being among Chinese breast cancer patients: The unique contributions of death anxiety, self-esteem, and social support by Kairong Yang, Yinpeng Ren, Wenya Peng, Xiangyu Wang, Xiaopeng Du, Jing Wang and Jiang Jiang in Journal of Health Psychology
Supplemental Material
sj-sav-5-hpq-10.1177_13591053231195391 – Supplemental material for Subjective well-being among Chinese breast cancer patients: The unique contributions of death anxiety, self-esteem, and social support
Supplemental material, sj-sav-5-hpq-10.1177_13591053231195391 for Subjective well-being among Chinese breast cancer patients: The unique contributions of death anxiety, self-esteem, and social support by Kairong Yang, Yinpeng Ren, Wenya Peng, Xiangyu Wang, Xiaopeng Du, Jing Wang and Jiang Jiang in Journal of Health Psychology
Supplemental Material
sj-sps-3-hpq-10.1177_13591053231195391 – Supplemental material for Subjective well-being among Chinese breast cancer patients: The unique contributions of death anxiety, self-esteem, and social support
Supplemental material, sj-sps-3-hpq-10.1177_13591053231195391 for Subjective well-being among Chinese breast cancer patients: The unique contributions of death anxiety, self-esteem, and social support by Kairong Yang, Yinpeng Ren, Wenya Peng, Xiangyu Wang, Xiaopeng Du, Jing Wang and Jiang Jiang in Journal of Health Psychology
Supplemental Material
sj-spv-4-hpq-10.1177_13591053231195391 – Supplemental material for Subjective well-being among Chinese breast cancer patients: The unique contributions of death anxiety, self-esteem, and social support
Supplemental material, sj-spv-4-hpq-10.1177_13591053231195391 for Subjective well-being among Chinese breast cancer patients: The unique contributions of death anxiety, self-esteem, and social support by Kairong Yang, Yinpeng Ren, Wenya Peng, Xiangyu Wang, Xiaopeng Du, Jing Wang and Jiang Jiang in Journal of Health Psychology
Footnotes
Acknowledgements
The authors thank the participants who participated in this study. Moreover, the authors are grateful to Wen Jiang from Department of Psychology, The Chinese University of Hong Kong for the help in reviewing the manuscript.
Author contributions
Kairong Yang, Jiang Jiang, Wenya Peng, and Xiaopeng Du conducted the conceptualization and formal analysis. Wenya Peng, Kairong Yang, Jing Wang, Xiangyu Wang, and Yinpeng Ren participated in the data collection. Kairong Yang wrote the manuscript, which all authors helped revise, and all authors contributed to and approved the final manuscript.
Data sharing statement
The current article is accompanied by the relevant raw data generated during and/or analysed during the study, including files detailing the analyses and either the complete database or other relevant raw data. These files are available in the Figshare repository and accessible as Supplemental Material via the Sage Journals platform. Ethics approval, participant permissions, and all other relevant approvals were granted for this data sharing.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Project for Humanities and Social Science of Ministry of Education, China (Grant No. 18YJA190005).
Ethics approval
All study procedures were reviewed and approved by the Ethics Review Committee of Cancer Hospital of Chinese Academy of Medical Sciences (Approval Number: NCC2907).
Informed consent
Informed consent was obtained from all individual participants included in the study.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.